
Abstract
Introduction
S
Depending upon the type of laser and the irradiation protocol in laser-assisted root canal treatment, a wide range of temperature increases has been reported. 2,3 This would correspond to a temperature of 47°C that has been described by Eriksson and Albrektsson 4 as being unsafe for periapical structure. Accordingly, both Gutknecht et al. 5 and Machida et al. 6 stated that the temperature threshold for laser root canal treatments is 7°C above body temperature, to avoid impaired bone regeneration and any damage to the periodontal tissues.
The degree and magnitude of laser effects on dental hard tissue are influenced by wavelength, power density, irradiation mode, duration of exposure, and type of tissue. 6,7 The amount of heat conducted to the tooth-supporting tissue depends also on the use of air and water during irradiation. The anatomical constriction and the least dentin thickness made the apical region more susceptible to thermal insult. 8
In 2010, Hmud et al. assessed thermal changes on the surface of root canals by using 940 and 980 nm lasers. The temperature measurement was accomplished by thermocouples placed in different positions on the root surface, with power settings of 2.5 W, 25 Hz for 980 nm, and 4 W, 10 Hz for 940 nm. After 5 sec of laser exposure, the external root surface temperature increased by a maximum of 4°C. 9
George and Walsh studied temperature changes on the apical third of root surfaces during irradiation with Er:YAG and Er;Cr:YSGG lasers using 4 W at 20 Hz and 1.25 W at 20 Hz for the two wavelengths, respectively, delivered by a conical side-emitting fiber tip compared with bare tips. The two laser systems and fiber designs elicited temperature increases <2.5°C. 8
Several theories have been suggested regarding the possible mechanisms for smear layer removal with Er,Cr:YSGG laser. Blanken and Verdaasdok assumed that the mechanism of action of Er,Cr:YSGG laser during root canal treatment is based on the rapid expansion and implosion of water vapor bubbles. By instantly heating the water to boiling temperature, high pressure vapor is expanded at high speed. The pressure of the surrounding liquid reverts to an implosion. The pressure inside the bubble might drop below the ambient pressure. The surrounding water accelerates inward creating high velocity water jets along the canal walls, removing the smear layer. 10
For endodontics, a significant restrictive factor for the use of this wavelength combination within the root canal is the magnitude of energy transmission and heat conduction to the tooth-supporting tissue by the two wavelengths.
The unique profile of laser emission in radial firing tips has shown to be an improvement regarding the disinfecting properties of root canals. In addition, these tips can provide a homogenous coverage of the root canal walls with laser energy that can lead to uniform removal of smear layer. 11 –14
To increase the success rate of endodontic treatment, the removal of the smear layer along with the eradication of bacteria residing deeply inside dentin tubules seems to be crucial. These two goals can be fulfilled by the innovative combination of the ablation efficacy of 2780 nm Er,Cr:YSGG laser together with the greater penetration depth in dentin of diode laser. 15,16
Irradiation parameters that ensure a safe clinical use of such dual wavelength laser should be defined before any in vivo application.
The aim of this in vitro study was to assess the surface and subsurface radicular dentin temperature changes at cervical, middle, and apical root thirds during laser irradiation with the selected parameters.
Materials and Methods
Samples selection and preparation
Fifty sound single-rooted human teeth, extracted for periodontal reasons, stored in distilled water containing 0.1% thymol were used. The teeth were scaled with curatte and the crowns of the whole teeth were discarded to a length of 14 mm with a slow speed handpiece and diamond disc, allowing a direct access to the canal. Patency of the apical foramen was confirmed with an ISO #8 K-file. The biomechanical preparation of the root canals was accomplished by using nickel–titanium Pro-Taper files to an apical size corresponding to an F4 Pro-Taper file (Dentsply, Switzerland) with a working length 1 mm shorter than the total root length.
Using a straight carbide bur (Meisinger LLC, Germany), small holes were drilled on the buccal surface of the root at a depth of 1 mm in the cervical and middle thirds. To prevent perforation in the apical third, a hole depth of 0.5 mm was prepared 2 mm from the apex.
Each root was fixed in a polyurethane resin material mixed in a 5:1 ratio (ISO-PUR K 760; ISO ELEKTRA; Elze/Germany) to possess a thermal conductivity of 0.6 W/m K and density of 1.4 × 103 kg/m3, except for 2 mm from the cervix of the roots for stabilization with a clamp and rubber dam. All models were polished to have a final dimension of (10\10\12 mm). Six thermocouples were fixed on each model; three on the lingual surface of the root. The other three thermocouples were fixed on the buccal surface of the prepared root inside the predrilled holes. Care was taken to secure the position of the buccal thermocouples directly opposite to the lingual thermocouples. A heat conductive silicone compound was used to improve heat conduction from the root surface to the thermocouples. Thermocouples were covered externally with sticky wax, thereby maintaining constant contact with the external model surface. The position of all thermocouples was confirmed radiographically (Fig. 1).
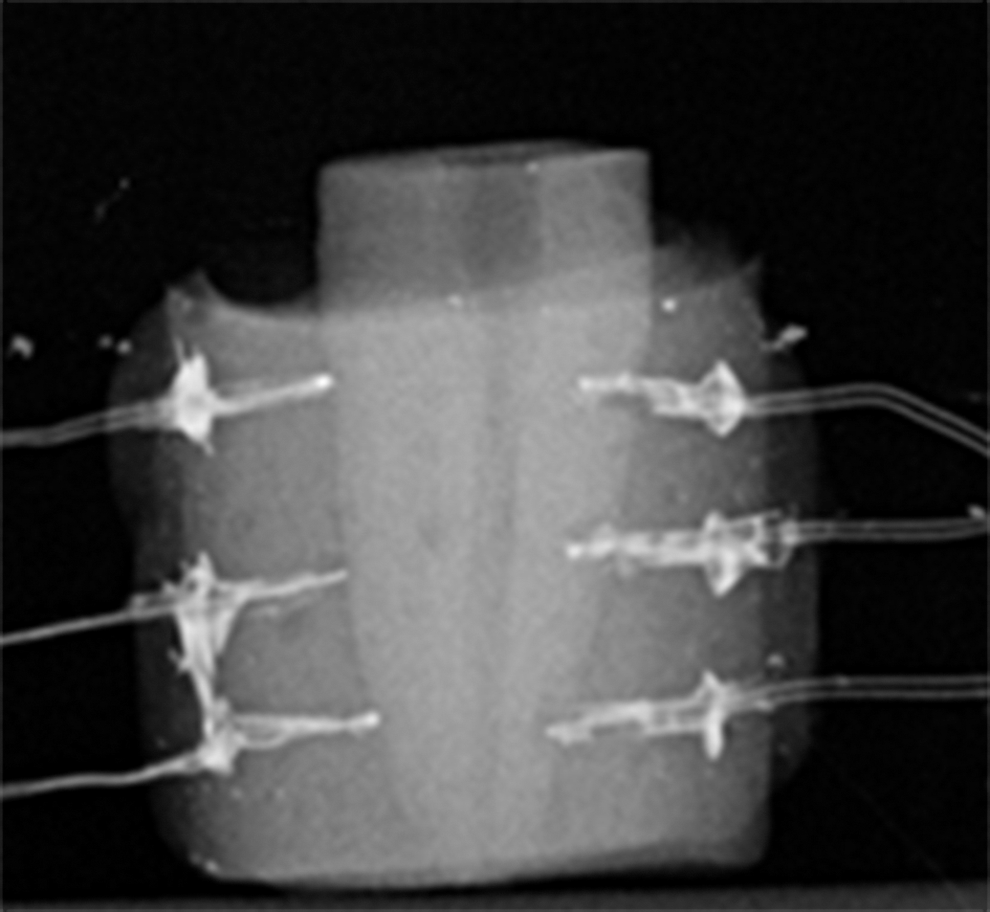
Radiograph of prepared sample with six attached thermocouples.
Temperature measurement
The whole experiments were conducted at an ambient temperature of 22°C ± 1°C. The model and six attached K-Type thermocouples (5TC-TT-KI-36-1M, Omega Engineering Inc., Stamford, USA) with wire diameter of 0.13 mm and an accuracy of ± 0.691°C were immersed inside a water bath. Temperature was set to 36.6°C ± 0.6°C with a seventh thermocouple fixed inside the water bath to monitor the water temperature. An eighth thermocouple was placed inside a cup filled with distilled water to record the temperature of water spray and irrigant solution.
The model was fixed in place by clamp and movable holder, isolated by a rubber dam and clamp. The data logged to the PC via an USB data acquisition module (OM-USB-TC, Omega Engineering Inc.; Stamford, USA) (Fig. 2). Sampling rate was set to 5 Hz.
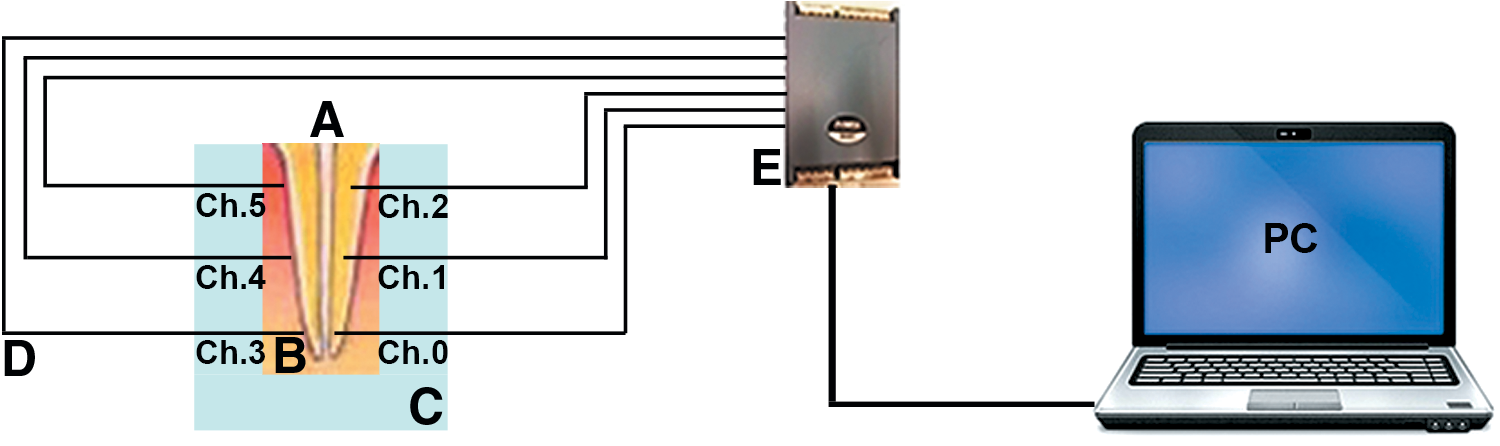
Schematic experimental setup.
Laser system
The dual wavelength laser (Biolase, San Clemente, CA) emits both 2780 nm Er,Cr:YSGG laser and 940 nm diode laser simultaneously, delivered via Radial Firing Tip (RFT) fiber (diameter 415 μm, length 21.17 mm, calibration factor 0.85). Power settings were 1.25 W, 50 Hz, 50 μs with 60% water level and 30% air pressure for Er,Cr:YSGG laser, and 2 W, in pulsed mode, for diode laser. The output power for both lasers was measured by FieldMaxII-Top powermeter (Coherent, USA) using MZ6 laser tip with a calibration factor of 1. The measured value was then multiplied by the calibration factor of the RFT fiber. The calculated output power from the RFT laser tip was 1.06 W for the Er,Cr:YSGG laser and 0.51 W for the diode laser. This difference was because of the calibration factor of the RFT laser tip (0.85). Also, additional losses were detected because of optics coupling in diode laser.
Sample grouping and irradiation protocols
Samples were divided randomly into two groups. Group A was irradiated with Er,Cr:YSGG laser, and group B was irradiated with a dual wavelength combination using different laser settings (Table 1). Each root canal was filled with distilled water before the laser fiber was placed in its starting position 1 mm short of working length (12 mm total working length). During irradiation, the RFT fiber tip was kept in constant helicoidal motion and withdrawn in a coronal direction at a speed of 1 mm/sec. According to the methodology of Ramalho et al. and Esteves-Oliveira et al., 17,18 the irradiation protocol for group A was composed of one round. Each sample received three irradiation cycles (total irradiation time 54 sec) separated by 5 sec rest time. In group B, the irradiation protocol was composed of three rounds, and each sample received nine irradiation cycles. In the first round, the samples were irradiated with the same power settings as group A, whereas in the second round, the wavelength combination of Er,Cr:YSGG and diode lasers was used with power settings of Pave = 0.51 W, pulse duration of 4 ms equivalent to duty cycle of 20%. For the third round, the same wavelength combination was used but with a different pulse duration of 10 ms for a diode laser, resulting in a duty cycle of 50%. The total irradiation time was 162 sec, and an interval time of 20 sec was set between laser rounds as can be seen in Table 1. Before each laser round, the canal was irrigated with 2 mL of distilled water at room temperature. Data were captured every 0.2 sec. Baseline temperatures immediately before and during laser irradiation, the maximum temperature during laser activation and the succeeding cooling periods were logged for each cycle, and differences were calculated.
To measure dentin thickness, roots were separated from the polyurethane resin material, dried, and polished from both sides (coronally and apically) using a polishing machine (Saphir 360, ATM GmbH, Mammelzen/Germany) to create a flat surface. Roots were sectioned vertically using a low-speed diamond saw (Exakt Apparatebau, Norderstedt/Germany) under continuous water cooling. They were then split into two halves, and the thickness of the dentin at the spot where thermocouples had been placed was measured by a vernier caliper (TOPEX Sp. z o.o. S.K., Warsaw, Poland).
Data analysis
All data were analyzed for normality using the Shapiro–Wilk's test. Data were normally distributed for both groups. One-way ANOVA and post-hoc Tukey tests were performed for multiple comparisons. p Values < 0.01 were considered statistically significant. Analyses were performed using the SPSS program (SPSS INC, Chicago, IL) version 20.0.
Results
In group A, a mean temperature increase of 4.43°C and 2.67°C was recorded for the buccal subsurface apical channel (Ch0) and lingual surface apical channel (Ch3), respectively (Table 2). Temperature changes on buccal root surfaces were significantly higher than on lingual root surfaces along the apical and middle thirds (p = 0.0001). For group B (Er,Cr:YSGG Pave = 1.06 W, diode laser Pave = 0.51 W), the mean temperature increase was 7.72°C and 5.07°C for the buccal subsurface apical channel (Ch0) and the lingual surface apical channel (Ch3), respectively (Table 3), for < 10 sec. During irradiation, the temperature dropped below baseline temperature by −4.30°C and −3.47°C in the buccal subsurface cervical thermocouples (Ch2) for group A and B, respectively. There were significant differences between surface and subsurface temperature changes of the same root third; apical and middle thirds (p < 0.001).
Differences in temperature between the same channel numbers of group A compared with group B differed significantly at the apical and middle thirds of the roots. Temperature elevation was significantly higher in group B than in group A (p < 0.00001).
Regarding dentin thickness, there were no statistical differences at positions of the same channel numbers of both groups (p = 0.671). There was an inverse linear relation between thermal stress and dentin thickness (R = −0.69, p < 0.001).
Discussion
The objective of this in vitro study was to investigate the thermal changes on root surface and subsurface during laser irradiation with dual wavelength of 2780 nm Er,Cr:YSGG and 940 nm diode lasers using group B irradiation protocol compared to conventional irradiation with Er,Cr:YSGG laser.
After biomechanical preparation of root canals the primary goals for a laser-assisted root canal treatment are the optimum removal of smear layer 19 and deep penetration of laser energy into dentin for means of disinfection against microorganisms that can breach >1000 μm inside dentin. 20
The different effects of these lasers (2790 nm Er,Cr:YSGG and 940 nm diode) arise from their differences in absorption coefficients in dentin. According to Beer– Lambert law, diode laser can penetrate deeper in dentin than Er,Cr:YSGG laser, because of its longer optical penetration (Lopt = 1/α) where Lopt is the optical depth and α is the absorption coefficient. 21
In fact, 940 nm diode laser is not absorbed strongly in either hydroxyapatite crystals or water, rather it penetrates deeply and transmits through the dentin to give the disinfection action. 2,16,22,23 Conversely, Er,Cr:YSGG laser can ablate efficiently dental hard tissue because of its high absorption coefficient in dentin that is approximately equal to 67 mm−1. This means that light penetrates only 17 μm in dentin. 24,25 Therefore, this wavelength does not have the ability to penetrate through deep dentin. This could explain the significant differences in temperature changes between all the same channel numbers from the two laser groups. In our study, regardless of the type of wavelength used, there were significant differences between the subsurface and its corresponding surface thermocouples, mainly because of the difference in dentin thickness between the subsurface and surface position of thermocouples.
The combination of two wavelengths in group B may possibly fulfill both goals at the same time. Although a critical temperature of 7.57°C and 11.7°C was recorded in the apical root surface and subsurface thermocouple of group B, respectively. This elevation was for 10 sec, which is far shorter than the 1 min critical threshold time. 4 On the contrary, this temperature may have a positive influence on killing the microorganisms deep in the dentin. This is in agreement with Gill et al., 26 when measuring the temperature elevation in the apical segment at a depth of 110 μm.
The behavior of the temperature change course of group A (Fig. 3) is almost the same for the apical and middle third channels, with different altitude because of differences in the position of thermocouples. Each peak represents the pass of the optical fiber opposing the thermocouples, where temperature elevation is maximum. These peaks take a pulse-like shape for the three cycles. In the last round of group B (Fig. 4), there was a compression in the width of the pulse, whereas the peaks were sharper and the temperature was higher. The maximum temperature elevation, which lasted for < 10 sec, was not the same for the last three cycles, where the highest peak could be seen in the last cycle of the third round. The temperature rose rapidly, reaching its peak value as the fiber tip was moved against the thermocouple, and dropped sharply as the fiber was moved away. 27 This can be regarded as evidence that 940 nm diode laser was transmitted through dentin, and that an additional absorption of laser light by thermocouples took place. Meanwhile, Er,Cr:YSGG laser was well absorbed in dental hard tissue. The heat that converted from absorbed energy was conducted and the temperature rose slowly. Afterwards, the tissue dissipated this excess temperature in the same manner.
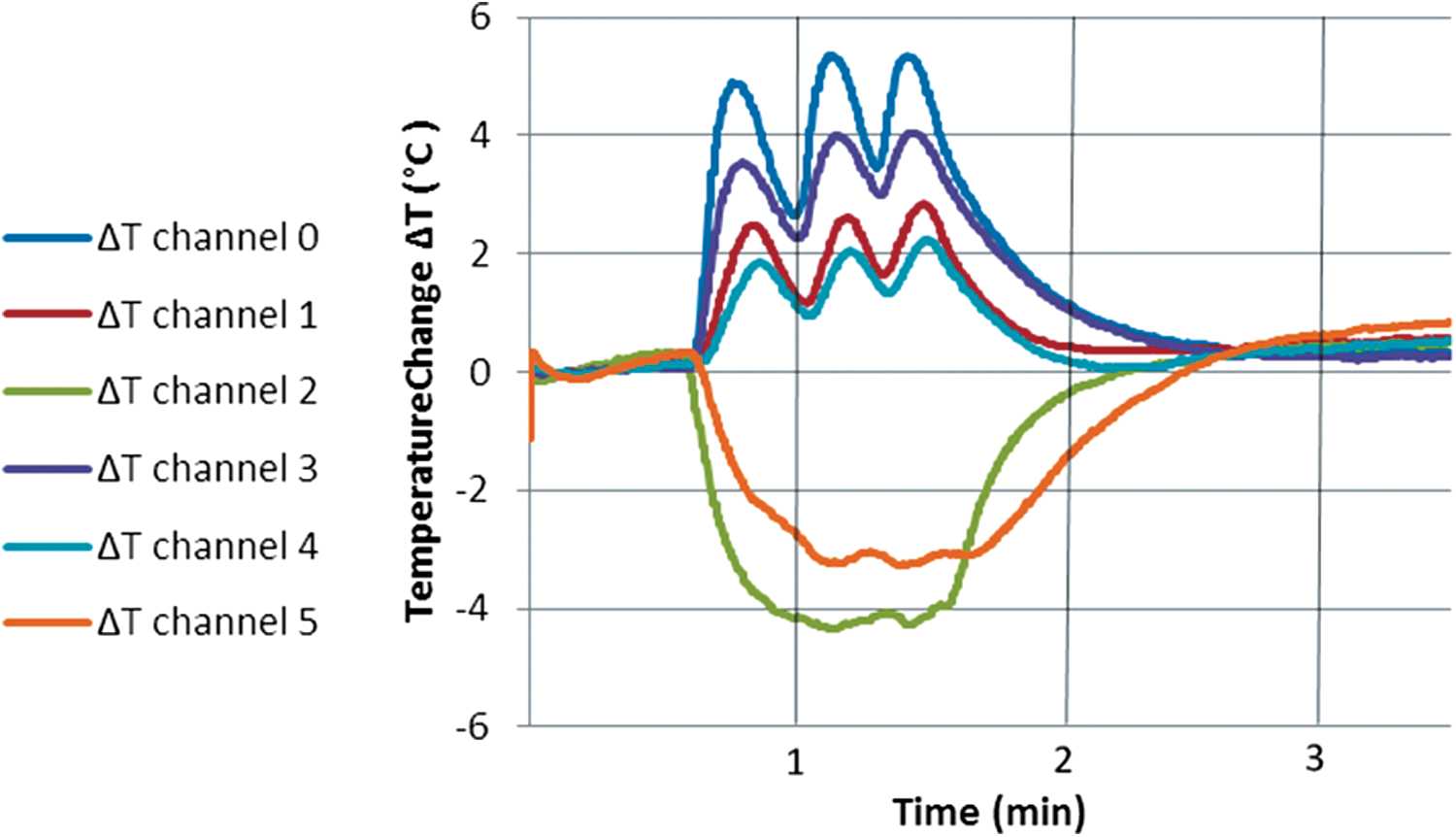
Data from a representative root treated according to the protocol of group A (Er,Cr:YSGG, Pave = 1.06 W) showing changes in the temperature of the buccal surface in hole channels (channel 0, channel 1, channel 2) and in the lingual surface channels (channel 3, channel 4, channel 5) at the same level of root thirds (apical, middle, and coronal).
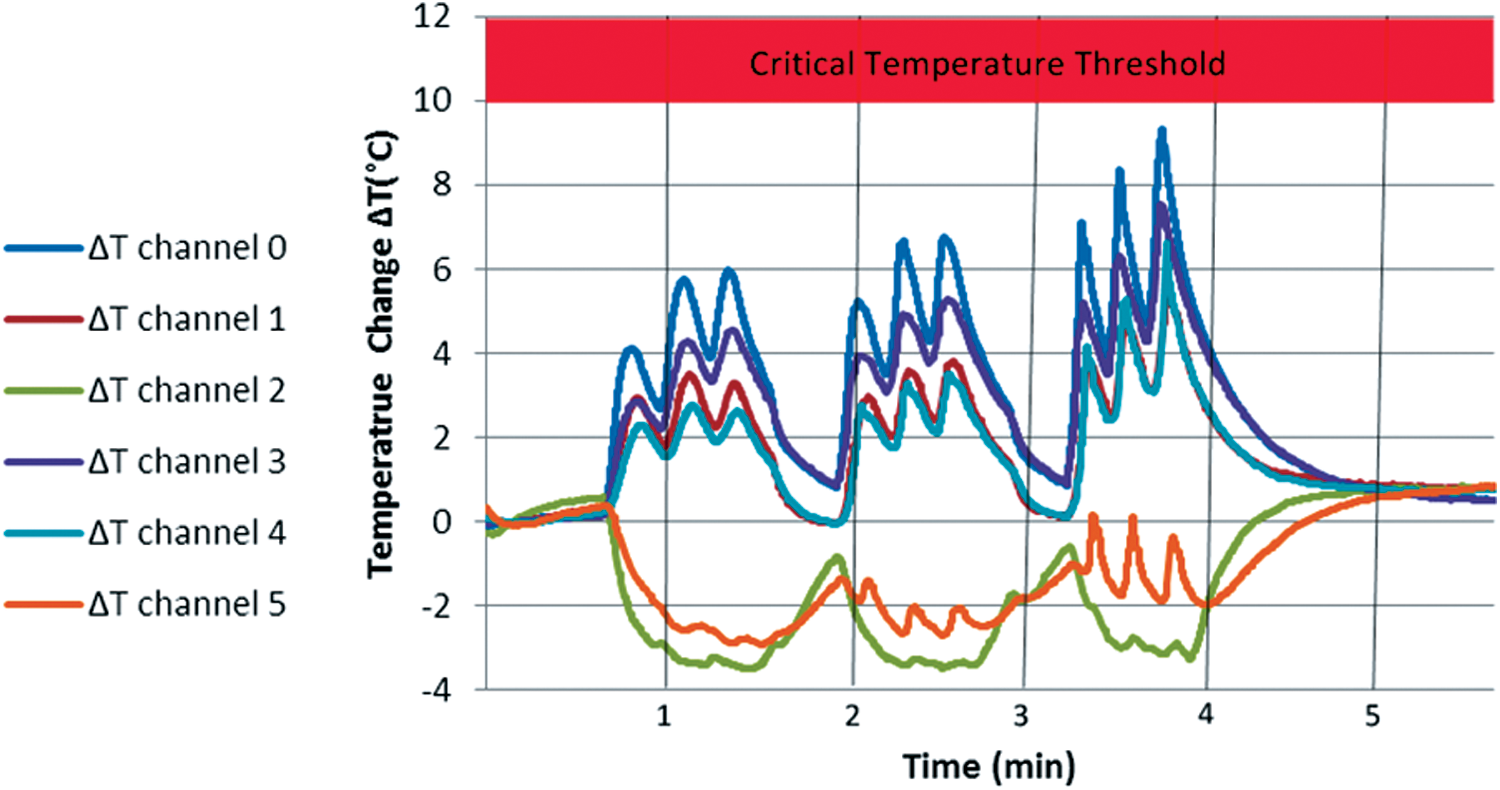
Data from a representative root treated according to the protocol of group B: Er,Cr:YSGG, Pave = 1.06 W; diode laser, Pave = 0.51W, and pulse width (4, 10) ms for rounds 2 and 3, respectively, showing changes in the temperature of the buccal surface in hole channels (channel 0, channel 1, channel 2) and the lingual surface channels (channel 3, channel 4, channel 5) at the same level of root thirds (apical, middle, and coronal).
Even when we used a rubber dam and clamps to secure a good isolation of the prepared root during laser irradiation, there was a decrease in the temperature below the baseline in the cervical thermocouples (Ch2 and Ch5) in both groups. This was mainly because of their position close to the water/air spray from the handpiece and water irrigation. Also, root canal anatomy upsurged the cooling effect cervically, where the diameter of root canal varied approximately from 200 μm at the apex to 2500 μm at root cervix. The combination of irrigant solution with diode laser intensified its bactericidal action in root canal treatment. 28 Preethee et al. confirmed a superior bactericidal efficacy of 908 nm diode laser combined with irrigants, compared with canals disinfected with diode laser alone. 15 This can be because of the cavitational effects that generate in aqueous fluids around the top of the laser fiber tip. This process results in the formation of pressure wave characterized by rapid change in pressure. A forced collapse of bubbles causes implosions that impact on surfaces, causing shear forces, rupture bacterial cell walls, and remove smear layer and debris. 29 Therefore, the use of an irrigant solution and constant moving of laser fiber tip could be a prerequisite for safe and efficient application of a dual wavelength laser in endodontic treatment.
Regarding the remaining dentin thickness (RDT), there were no significant differences in dentin thickness at positions of the same channel numbers in either group. This result could exclude the effect of thickness on the temperature measurement; that is, the results were mainly caused by the wavelength change from Er,Cr:YSGG laser in group A to a combination of Er,Cr:YSGG and 940 nm diode lasers in group B.
In the present study, polyurethane casting resin has a thermal conductivity of 0.6 W/m K and a density of 1.4 × 103 kg/m3 was used to mimic the in vivo conditions, where thermal conductivity of the bone 30 ranges from 0.58 to 1.2 W/m K and a density 31 of 1.3 × 103 kg/m3. Even though we did not take into account the blood perfusion rate of the surrounding bony tissue (1.8 mL/100 g/min), blood circulation can add an additional cooling effect. Therefore, the results of this study are expected to be higher than in the in vivo conditions.
Further investigations that implement the antibacterial efficacy and verify the inner root surface morphology by scanning electron microscopy of the experimental settings of the dual wavelength laser should be inspected before bringing these parameters into clinical trials.
Conclusions
Within the limits of this in vitro study, the use of dual wavelength laser can be considered safe in laser-assisted root canal treatment. Power settings of 1.06 W, 50 Hz, and 50 μs for Er,Cr:YSGG laser and 0.51 W for diode laser with a pulse duration of 4 and 10 ms generated an acceptable temperature rise on the external root surface. A correlation between RDT and temperature elevation could not be found, provided that the fiber was moved continuously and irrigation was performed between laser exposures.
Footnotes
Author Disclosure Statement
No competing financial interests exist.