
Abstract
Introduction
D
Most optimal irrigation protocol requires the use of the organic and inorganic irrigants in addition to an antimicrobial agent. As there is no single solution that has the ability to remove both organic and inorganic materials, sequential use of two or more solutions is required. Currently, sodium hypochlorite (NaOCl) (0.5–6.15%) and ethylenediaminetetraacetic acid (EDTA) (15–17%) are the two most commonly used intracanal irrigants to remove the smear layer. 5,6 QMiX 2in1 (DENTSPLY Tulsa Dental Specialties, Tulsa, OK) is also a new solution with antimicrobial agents for smear layer removal, proving to be as effective as 17% EDTA. 7 Its chemical composition contains EDTA, chlorhexidine (CHX), and a specific detergent. 6
Removing the smear layer from the apical thirds of root canals is very difficult, regardless of the solution used. The irrigating solutions can be inefficient at this point. Therefore, researchers have improved some irrigation agitation methods to overcome this challenge. 8 Recently, agitation of irrigants with laser devices has become popular. 9 –11 Use of neodymium-doped: yttrium-aluminum-garnet (Nd:YAG) laser with 1064 and 1320 nm wavelengths was reported to enhance cleansing of the root canals compared with NaOCl irrigation. 11,12 Moreover, in a recent study it was reported that agitation of 15% EDTA with an 808 nm diode laser for 20 sec was effective in removing the smear layer in the apical thirds of root canals. 13 Therefore, the aim of this study was to evaluate the efficiency of agitation of 17% EDTA and QMiX with an 810 nm diode laser on removal of smear layer.
Materials and Methods
A total of 75 human mandibular premolar teeth extracted for periodontal reasons collected from both sexes ranging from 45 to 55 years of age were used. This study was approved by Ethical Committee of Bülent Ecevit University (Protocol number: 2015-07-13/05). The teeth were cleaned to remove soft tissues and calculus, and were stored in distilled water until use. All teeth were analyzed with digital radiographs in buccal and proximal directions to check for single canals. The canal patency was controlled with a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland). The working length (WL) of each canal was determined as 1 mm short of the length where a 10 K-file was visible from the major apical foramen.
The crowns of all teeth were removed at the level of the cementoenamel junction, in order to obtain a standardized root length of ∼13 mm. The root canals were prepared with ProTaper rotary instruments (Dentsply Maillefer, Ballagues, Switzerland) up to size #30 (F3). Root canals were irrigated with 2 mL 5% NaOCl (ImidentMedEndosolve-HP, Konya, Turkey) between instrument changes. After the preparation of the root canals, the specimens were irrigated with 5 mL of 2.5% NaOCl for 1 min, then divided randomly into the following five groups according to final irrigant used (n = 15/per group): Group 1 (control group): no irrigation performed Group 2 (EDTA group): a final flush with 5 mL of 17% EDTA (Wizard; Rehber Kimya San, Istanbul, Turkey) solution for 1 min Group 3 (QMiX group): a final flush with 5 mL QMiXsolution for 1 min Group 4 (EDTA+Laser group): 1 mL 17% EDTA solution was placed in the canals of the specimens and then agitated with a fiber tip (Ø = 400_μm) at 2 W using the pulsed mode (10 Ton ms/Toff 10 ms) of the diode laser (81010 nm, AMD Picasso, Indianapolis, IN) for 20 sec. The specimens were then irrigated for 40 sec with 4 mL 17% EDTA as a final flush. Group 5 (QMiX+Laser group): 1 mL QMiX solution was placed in the canals of the specimens and then agitated at 2 W using the pulsed mode (10 Ton ms/Toff 10 ms) of the diode laser for 20 sec. The specimens were then irrigated for 40 sec with 4 mL QMiX as a final flush.
All irrigation procedures were performed by using 30 gauge irrigation needles (Vista-Probe; Vista Dental, Racine, WI) with an up and down motion to 1–2 mm short of the WL. All the laser applications were performed parallel to the root canal. The tip of the laser was kept 2 mm from the working length, and was withdrawn gently from the apical region to the coronal region with a helical movement. Following the use of an irrigation regime, each specimen was rinsed with 5 mL of distilled water to remove the precipitate of the test solutions, and dried with paper points.
Two longitudinal grooves were prepared on the buccal and lingual surfaces of each root with a diamond bur used with a high-speed, water-cooled handpiece to facilitate vertical splitting with a chisel after root canal preparation. Teeth showing evidence that the groove had penetrated into the root canal or exhibiting an irregular cleavage were discarded and replaced with a new specimen.
Scanning electron microscopic (SEM) evaluation
The roots were split longitudinally and prepared for SEM investigation. Each specimen was coded and mounted on an aluminum stub, coated with gold-palladium, and examined under a scanning electron microscope (Quanta™ 450 FEG, FEI, OR). Serial scanning electron photomicrographs were made at × 500, × 1000, and × 2000 magnification covering the total circumference of the canal walls at the levels of the apical, middle, and coronal thirds of the root canal (Fig, 1).The amount of smear layer was scored by one calibrated blinded observer according to the following criteria used by Torabinejad et al. 14
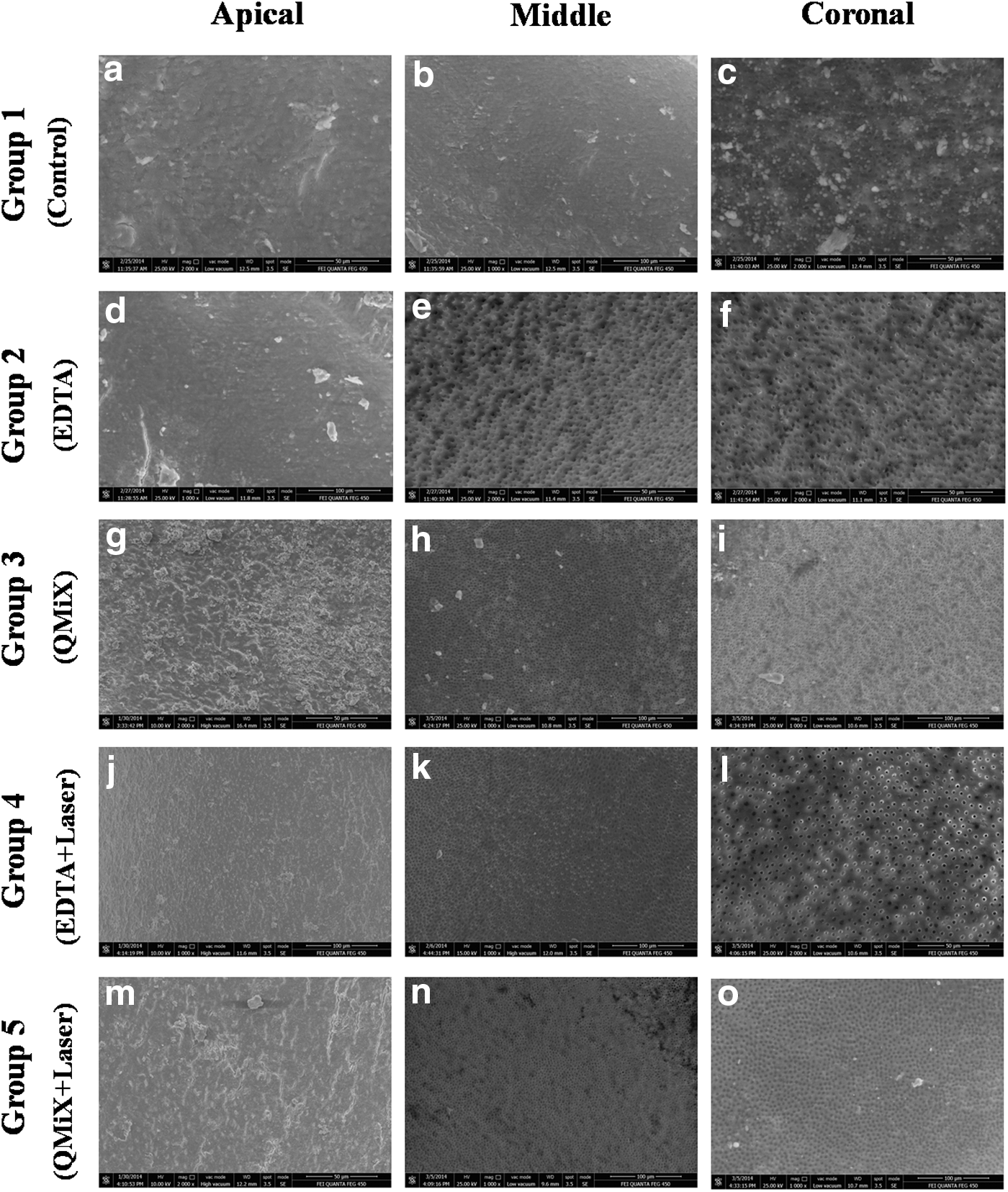
Representative photomicrographs of groups with × 1000
Scores were: 1 = no smear layer (no smear layer on the surface of the root canals; all tubules were clean and open); 2 = moderate smear layer (no smear layer on the surface of root canal, but tubules contained debris); and 3 = heavy smear layer (the smear layer covered the root canal surface and tubules).
The scores obtained from SEM evaluation were compared using the Kruskal–Wallis test. The Dunn's test was used for post-hoc testing after the Kruskal–Wallis test. p < 0.05 was considered to be significant.
Results
Figure 1 demonstrates the representive SEM images of the groups. The means and standard deviations of groups in the coronal, middle, and apical thirds are shown in Table 1. Regardless of the region of the root canal, all tested groups showed significantly lower smear layer scores than the control group (p < 0.001). In all experimental groups, the smear layer scores of the apical thirds were significantly higher than those of the coronal and middle thirds (p < 0.001). A significant difference between the coronal and middle thirds was solely observed in EDTA group (p < 0.001).
EDTA, ethylenediaminetetraacetic acid.
A comparison of intergroup findings according to region of root canal demonstrated a significant differrence in apical thirds between the EDTA group and the other experimental groups (p < 0.001), whereas no difference was found in the coronal and middle thirds (p > 0.001). There was a significant difference between the EDTA and the EDTA plus laser groups at the apical area (p < 0.001).
Discussion
To achieve a successful endodontic treatment, chemomechanical treatment of the root canal system, especially in the apical third, is very important. Laser-activated irrigation has been recently introduced for the purpose of smear layer removal. 10,15,16 This procedure is based on the activation of the irrigant with the cavitation process. During laser activation, the formation of vapor bubbles, the collapse of the bubbles, acoustic streaming, and, finally, cavitation processes occurred. 17 The mechanism for the laser agitation of irrigants based on the absorption of laser energy is related to the type of irrigants and the wavelength of the laser. Lasers with wavelengths from 940 to 2940 nm have been suggested to efficiently activate irrigants in the root canal. 18,19 However, in a recent study, an 808 nm diode laser was used with 15% EDTA, and according to results, the highest number of open dentinal tubules was observed in the middle and apical thirds of root canals with 20 sec of laser agitation. 13 In the present study, 810 nm diode laser agitation was evaluated for the removal of smear layer. According to the present study results, regardless of the different region of root canals, all the irrigation solutions and their agitation with the laser resulted in more smear layer removal than with the control group. Comparing the different regions of the root canal walls, the results of the present study showed that smear layer removal in the coronal and the middle segments in the QMiX, QMiX plus laser, and 17% EDTA plus laser groups was equal, that these two areas were cleaner than the apical third of the root canal, and that all were different from control group. However, in the 17% EDTA group, the coronal area was cleaner than the middle, and the middle area was cleaner than the apical area. These results showed that all the solutions and combinations with laser were more effective in the coronal third than in the middle and apical thirds. These observations are in agreement with the results of previous studies showing that the apical third of the canal is more difficult to clean. 11,20 These results can be explained by root canal morphology. Because of the wide openings of dentinal tubules in coronal and middle thirds, laser and irrigants can act more effectively.
In contrast to a previous study of Arslan et al., 13 the present study results showed that laser agitation did not improve the removal of the smear layer in the apical third. 13 The differences between these studies may be related to the methodology used. Arslan et al. closed the apexes of the root canals with the boxing wax. This situation resulted in gas entrainment at the end of this region, which produced a vapor lock effect during the irrigation procedure. 13 Moreover, in the previous study, the exposure time with EDTA was 120 sec, whereas, in the present study, EDTA was applied for 60 sec. 13 Prado et al. reported that the amount of smear layer removed by EDTA in 30 sec was poor. 21 This result is in accordance with another study, which applied EDTA for 1 min. 22 These could be explanations why there was poor smear layer removal from the apical thirds in the present study.
QMiX is composed of EDTA, CHX, and a surfactant, which enhanced the demineralization of radicular dentine with the chelating effect of EDTA, while disinfecting at the same time. 7 The purpose of adding a surfactant in QMiX is to lower the surface tension of irrigant and increase its wettability, and to enhance the flow of the irrigant into the root canal and its contact with the smear layer. 23 According to the present study results, QMiX and its agitation with laser showed better results than in control group in removing smear layer, with significance.
Conclusions
In conclusion, QMiX demonstrated comparable efficiency with EDTA in removing the smear layer. The application of diode laser significantly increased the efficiency of EDTA solution at the apical thirds.
Footnotes
Author Disclosure Statement
No competing financial interests exist.