
Abstract
Introduction
P
Effective treatment for the management of chemotherapy-induced OM is not yet available. 7 However, recents studies have shown the effectiveness of low-level laser therapy (LLLT) for preventing and treating chemotherapy-induced OM, as a result of its anti-inflammatory, biomodulator, and tissue repair properties. 8 –12
With regard to the impact of LLLT on the QoL of patients receiving cancer treatment, recents studies involving patients undergoing chemoradiation for head and neck cancer have shown positive effects of LLLT on their QoL. 13 –16 Most studies related to LLLT deal with the clinical aspects of laser treatment in chemotherapy-induced mucositis, 10,11,17 but there is no evidence of its effect on subjective aspects of patients undergoing HSCT. Consequently, there is a need to understand the subjective aspects experienced by patients receiving LLLT, in order to assess if this therapy has an influence on their QoL during treatment. This study aims to evaluate the impact of LLLT on OM and QoL in patients undergoing HSCT using the Oral Health Impact Profile (OHIP-14) and the Functional Assessment of Cancer Therapy-Bone Marrow Transplantation (FACT-BMT) questionnaires.
Material and Methods
Study design and participants
This study was designed as a randomized, controlled, and double-blinded clinical trial. Patients hospitalized in the Hematopoietic Stem Cell Transplantation Unit of the Hospital Araújo Jorge/ Associação de Combate ao cancer em Goiás (HAJ/ACCG) between February 2012 and May 2014 were included in the investigation. The research was performed in compliance with the Research Ethics Committee of the Federal University of Goiás and HAJ/ACCG (protocols 382/2011 and 024/2012, respectively). This investigation was conducted in full accordance with the ethical principles of the World Medical Association Helsinki Declaration, and all patients signed an informed consent form. Parents or guardians signed for those <18 years of age.
A post-hoc power test was performed considering the use of laser as the dependent variable, the FACT and OHIP scores as the independent variables, and a two sided 95% confidence interval by the normal approximation method. The power estimates were low (OHIP – 11.24%) to moderate (FACT – 57.06%). Therefore, this is a pilot study that provides valid estimations for future trials investigating the association between oral health and QoL in patients undergoing HSCT.
Patients were block randomized on the day of admission (AD) into two groups, one that would receive LLLT (laser group) and the other that would not (control group). One member of the team performed a permuted-block randomization of participants using Research Randomizer site (
Conditioning regimens
The characteristics of the conditioning regimens are summarized in Table 1. It is noteworthy that no patient received chemotherapy protocol with TBI. Patients received 200 mg fluconazole intravenously every 12 h, and 500 mg/m2 acyclovir intravenously every 8 h prior the transplant, from D-2 until neutrophil recovery (granulocytes=500/mm3).
Busulfan 16 mg/kg and cyclophosphamide 120 mg/kg (D-7 to D-2).
Fludarabine 30 mg/m2 and busulfan 16 mg/kg (D-5 to D-2)/prophylaxis of GVHD with MTX (D+1/D+3/D+6/D+11).
Melphalan 200 mg/m2 (D-3 to D-1).
Carmustine 300 mg/m2, cytarabine 1600 mg/m2, etoposide 800 mg/m2, and melphalan 140 mg/m2 (D-7 to D-2).
HSCT, hematopoietic stem cell transplantation; GVHD, graft-versus-host disease; MTX, methotrexate.
Laser therapy protocol
In the intervention group, an InGaAIP diode laser was used to irradiate the oral mucosa. The parameters used were 660 nm wavelength, output power of 40 mW, and an energy density of 4 J/cm2 measured at the fiberoptic end with 0.04 cm2 of section area. A dentist with expertise in laser irradiation performed the laser therapy to the upper lip mucosa, lower lip mucosa, right and left bucal mucosa, right and left lateral tongue, ventral tongue, and mouth floor. Laser was applied to 10 points in each mouth region, with an exposure time of 4 sec per point, using 0.16 J of energy per point. The total energy applied per day was 12.8 J, and the total number of irradiated spots was 80 points (660 nm, 40 mW, 0.16 J, 4 J/cm2, per point). Subjects received LLLT daily from the 1st day of the conditioning regimen through to the 7th day after transplantation (D+7).
For ethical purposes, and because there is evidence in the literature showing the effectiveness of laser therapy in the treatment of OM, 10 –12 in the present study laser treatment was applied to patients in the control group who had developed grade 3 OM. Only three patients in the control group had received laser prior to D+7, and the statistical analyses without these patients did not change the results.
Evaluation of OM
A clinical evaluation of the severity of OM was conducted in both groups in accordance with the World Health Organization (WHO) scale 18 as follows: grade 0, no signs or symptoms; grade 1, erythema without lesion, or mild soreness; grade 2, ulceration, but able to eat solids; grade 3, painful ulcers, but able to swallow liquids; and grade 4, requiring parenteral support and continuous analgesia.
Two professionals at the HSCT Unit, one oncologist and a nurse, performed the OM evaluation using artificial light. Both were blinded for the randomization, in order to minimize interobserver variation; for accuracy in classifying, the OM was assessed in seven patients before the study by means of a pilot test. There was a high agreement between the evaluators (agreement rate 93%). Each patient was assessed daily from the day of transplantation (D0) until the 20th day (D+20) or until discharge (DC).
QoL measurements
A single member of the HSCT Unit staff administered the two QoL questionnaires, the FACT-BMT and the OHIP-14 to the patients in both groups (laser and control) at three time points: at AD, on D+7, and at DC. The questionnaires were administered by interview and the researchers were blinded for the randomization allocation.
The OHIP-14 instrument consists of 14 questions related to oral health, whose responses options are five scores: 0 Never, 1 Hardly ever, 2 Occasionally, 3 Fairly often, 4 Very often. 19 The FACT-BMT consists of 41 questions divided into six dimensions related to general health (physical well-being, family/social well-being, relationship with physician, emotional well-being, functional well-being, and additional worries). Each question has five response options: 0 Not at all, 1 Slightly, 2 More or less, 3 A lot, and 4 Very much. This questionnaire is intended for subjects>18 years of age, and it is specific to HSCT patients. 20 On the FACT-BMT, the positive impact questions' scores were inverted to obtain the final score. In both questionnaires, the higher the final score, the worse the patients' QoL. For the OHIP-14, the total score can vary from 0 to 56 points, whereas for the FACT-BMT, it can vary from 0 to 164.
Statistical analysis
The primary outcomes of this study were the occurrence and severity of OM and the QoL of patients according to the FACT-BMT and OHIP-14 scores, when the laser and control groups were compared. The secondary outcomes were the progression of the mucositis and QoL from AD to hospital DC, the influence of mucositis on QoL, and the relationship between FACT-BMT and OHIP-14 scores.
Descriptive, bivariate, and multivariate statistics were determined using SPSS version 17.0 software, with a significance level set at 5%. The Spearman rank correlation, Mann–Whitney, and Friedman nonparametric relations tests were used to compare two groups of non-normal distribution. When the distribution was normal, the t test was used to compare the two paired groups. To statistically evaluate OM severity in both groups, the highest degree of OM presented by a patient from AD to DC in the HSCT Unit was considered.
As the QoL data were assessed at three different time points, the Generalized Estimating Equation (GEE) was used for the multivariate analysis of the longitudinal changes in the FACT-BMT and OHIP-14 scores involving the variables “laser application,” “OM severity,” and “time of application of the questionnaire,” The GEE 21 is a method of analyzing a variety of regression models that considers correlated measures between subjects and between groups, data missing for a given measurement, and covariates that change over time. In addition, it does not require a normal distribution of the outcome variable.
Results
Characteristics of patients
A total of 39 patients (22 females and 17 males) met inclusion criteria and were accepted to participate in the study. They were randomly assigned to two groups: control (n=19) and laser (n=20). Mean age of the total sample was 39 years (minimum of 14 and maximum of 63) (Table 1). There was no difference (p>0.05) between the clinical and demographic characteristics of the laser and control group patients, which shows homogeneity between the groups.
Clinical evaluation of OM
Percentage distribution of the highest degree of OM severity according to the WHO scale is in Fig. 1. The majority of patients in the laser group presented grade 1 OM, whereas in the control group the cases were distributed over grades 0–3 (Fig. 1). It is important to note that the laser group showed no grade 3 mucositis.
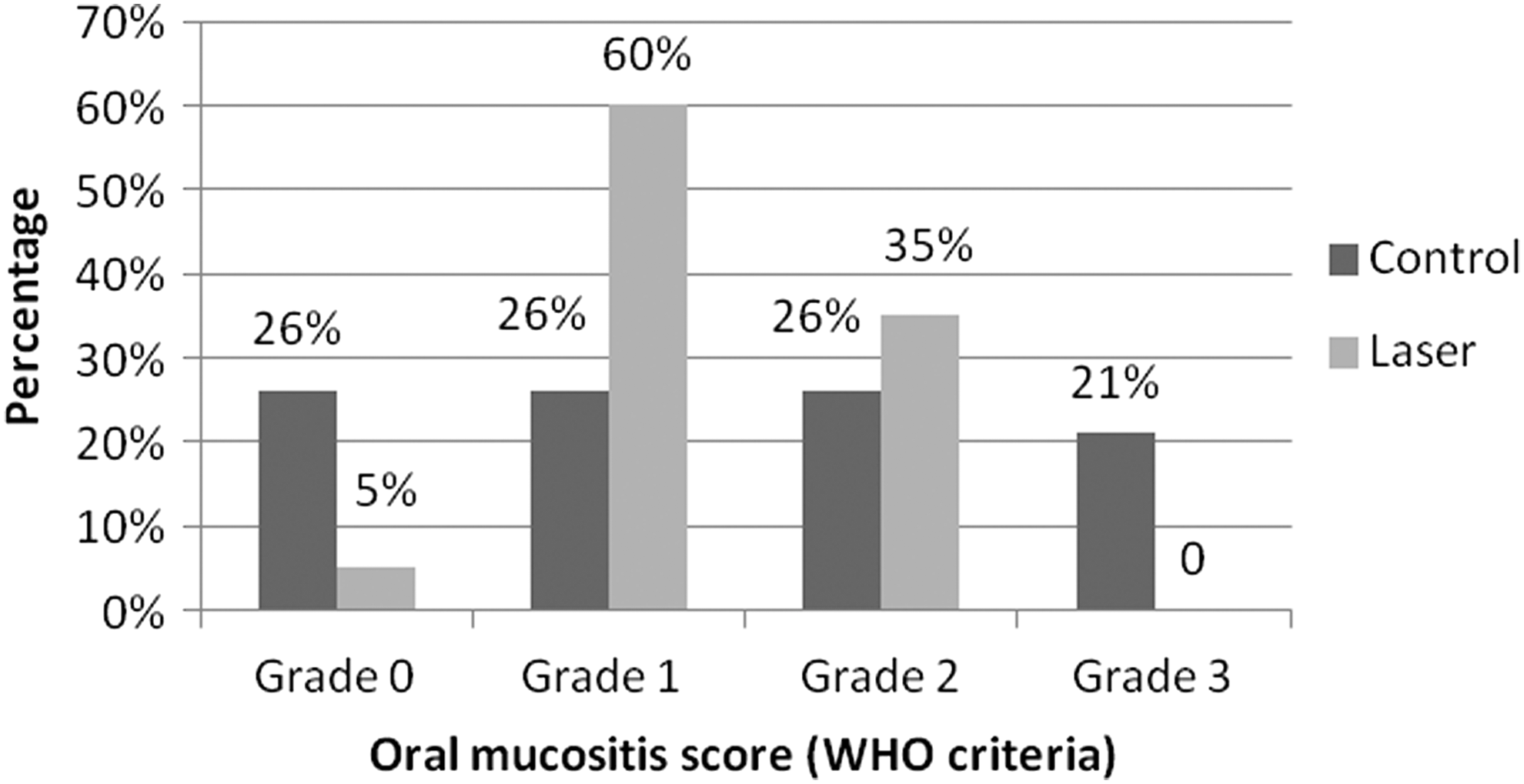
Comparison between the two groups in relation to the highest oral mucositis (OM) severity grade from admission (AD) to discharge (DC) from the Hematopoietic Stem Cell Transplantation (HSCT) Unit.
On analyzing the degree of OM from D0 until hospital DC, it was seen that it peaked between D+9 and D+10, and from D+7 onwards, the degree of OM was lower in the laser group. It was also seen that OM healing improved in the laser group, reducing the healing time of ulcers when compared with the control group (Fig. 2).

Mean oral mucositis (OM) scores of patients over their hospitalization period, analyzed from day of transplantation (D0) until discharge (DC) of each patient. *χ2, p=0.05 on day D+10 when laser and control groups were compared.
Effect of LLLT on QoL
The FACT-BMT and OHIP-14 questionnaires correlated poorly (Spearman's rho=0.342, p=0.002); therefore, both QoL indicators were included in the analyses. The bivariate analysis showed that the use of the laser was not statistically associated with total scores for the FACT-BMT (paired samples t test, p=0.074) or the OHIP-14 (Mann–Whitney test, p=0.749). Therefore, laser therapy did not improve patients' QoL at any of the three time points, when compared with the control group.
The highest scores, indicating poor QoL, were found on D+7 in both control and laser groups when evaluated by the two instruments. When the OHIP-14 was analyzed, there was a considerable reduction in the score for the D+7 until the DC period for the laser group but not for the control group (Fig. 3). When the overall sample was analyzed, total FACT-BMT scores returned to baseline levels at DC, but this did not occur with the OHIP-14 instrument (Table 2). In addition, there was a deterioration in QoL for the whole sample on D+7. It is important to note that, as the FACT-BMT questionnaire is intended for subjects>18 years of age, fewer patients answered FACT-BMT when compared with the OHIP-14 questionnaire (Table 2).

Distribution of total score means for Functional Assessment of Cancer Therapy-Bone Marrow Transplantation (FACT-BMT) and Oral Health Impact Profile (OHIP-14), according to time of observation and use of laser.
Paired samples t test
Friedman test
Along the same line, different letters indicate that values differed significantly at the three time points.
FACT-BMT, Functional Assessment of Cancer Therapy-Bone Marrow Transplantation; OHIP-14, Oral Health Impact Profile.
Effect of OM severity on quality of life
OM severity was not associated with FACT-BMT total scores (Spearman's rho=0.143, p=0.199), but showed a positive, although weak, correlation with OHIP-14 scores (Spearman's rho=0.224, p=0.019).
The effect of laser and OM severity over time presented different models in the GEE for the FACT-BMT and OHIP-14 continuous variables (Table 3). The beta values are interpreted as an increase or decrease in the scores of the QoL tools assessed, when the other independent variables are controlled. The FACT-BMT scores on D+7 were higher than at AD and DC, when laser application and OM severity were controlled. There was a reduction in OHIP-14 scores by approximately five points between nonulcerated and ulcerated OM when the variables related to the use of laser and time of administration of the questionnaire were controlled.
FACT-BMT, Functional Assessment of Cancer Therapy-Bone Marrow Transplantation; OHIP-14, Oral Health Impact Profile.
Discussion
The major finding of this trial is that the QoL of HSTC patients is so deteriorated at D+7 that any effect of a local treatment such as LLLT for OM could not have a substantial impact on patients' perceptions. The participants of this study significantly felt the repercussion of the intensive treatment regimens on their physical and functional well-being (FACT-BMT subscales), and the oral-related QoL was also an issue for their general QoL, as FACT-BMT and OHIP-14 were correlated.
Chemotherapy-induced OM during HSCT is a genuine concern for both patient and healthcare team, as it can lead to serious medical complications for the patient, 17 and thereby compromise the patient's QoL. Members of our research group published two studies recently showing the clinical effectiveness of LLLT for the prevention and treatment of OM in patients undergoing HSCT. 11,12 Their findings coincide with the clinical findings of this study.
The laser parameters in the present study were established based on randomized controlled research by our group 12 as well as being based on studies in bone marrow transplantation patients with similar LLLT parameters. 17,22
In the present study, despite the clinical improvement seen as a result of LLLT, there was no improvement in QoL related to general or oral health in the laser group when compared with the control group. On the other hand, previous studies have shown an improvement in QoL measures of patients receiving LLLT for the prevention and treatment of mucositis, but these studies were conducted with head and neck cancer patients who had undergone radiotherapy and/or chemotherapy. 14,23 Their situation is totally different from that of HSCT patients, who often experience many psychological and physical threats.
Some studies report that factors such as diagnosis, lengthy hospitalization, invasive and noninvasive procedures, withdrawal from day-to-day activities, removal from the family atmosphere, isolation, mental suffering, and the uncertainty of a cure with high doses and intensive treatment regimens could overlap and directly influence the overall QoL of patients. 24,25 Hence, we suggest that such factors could have hindered the analysis of improvement in QoL with LLLT application. Therefore, it appears that the clinical improvement in OM with LLLT, when assessed by the FACT-BMT, cannot by itself annul the many other complications and suffering that the patient faces, and could have made it difficult for patients to realize the benefits of laser therapy to their QoL. Furthermore, the FACT-BMT, a validated instrument for HSCT and an excellent choice for use in HSCT clinical trials, has been primarily used in studies to assess QoL in post-treatment survivors of HSCT, 25,26 whereas in this study, it was used for patients during hospitalization in the HSCT Unit.
Oral cytotoxicity usually begins in the first days after the conditioning regimen, and a peak is reached between the 7th and 11th days after transplant (D+7 to D+11), and this nearly always coincides with the patients' period of immunosuppression. 5,27 These data corroborate with our findings in this study. We also observed higher total scores of FACT-BMT and OHIP-14 when compared with AD and DC in both groups (control and laser) on D+7, which reflects a poorer QoL at this stage of hospitalization. Furthermore, these data coincide with the OM peak seen between D+9 and D+10 in this study.
With regard to OM severity on D+7, the laser group presented a greater total FACT-BMT score for grade 0, when compared with grade 3 OM. These subjective outcomes of the patients' reported measures suggest that as the FACT-BMT questionnaire mainly addresses subjective factors related to general health, it could have compromised the evaluation of the effect of the laser on general health-related QoL. Furthermore, it is important to emphasize that the potent analgesics, very frequently used during hospitalization and commonly used to control the pain of severe mucositis, could be a confounding factor for this study, as they can seriously interfere with the patients' perception of QoL.
When evaluating the OHIP-14, the worsening of OM severity accompanied the worsening of QoL on D+7 for both groups. Although LLLT had no positive effect on QoL on D+7, at DC there was a tendency toward improvement in QoL in relation to oral health in the laser group when compared with D+7, and this was not evident in the control group. Furthermore, when evaluating the degree of OM from D0 (day of the transplant) to DC, it was seen that healing time was shorter in the laser group. These data corroborate the study by Antunes et al. 28 on HSCT patients who had received LLLT. They found that in the laser group, the healing time for the ulcers was shorter (6 days on average). 28 Therefore, we hypothesize that the laser group experienced an improvement in OM healing with a gradually reduced of OM severity, and only on hospital DC was that reflected in an improvement in their oral health-related QoL. The laser treatment effects are cumulative, and perhaps when considering the severity of the mucositis in both groups on D+7, it is not possible to detect any improvement in QoL at this time point. We suggest that at DC, with their OM severity reduced, and with the overall improvement in their general health and emotional state, patients can see the improvement, which is reflected in positive subjective outcomes.
It is important to recognize some limitations of this study, such as the reduced number of subjects enrolled in the research, the repeated use of morphine chlorinate for pain control, and the recurrent critical threats experienced by patients, which are common situations in any HSCT unit. Nevertheless, as the present study is the first that aimed to analyze subjective aspects experienced by HSCT patients receiving LLLT, we believe that our results provide a useful insight into the investigation of subjective aspects involved in laser therapy, as well as being able to contribute to the design of future studies involving the assessment of QoL in patients undergoing HSCT.
Conclusions
The use of LLLT reduced the severity of chemotherapy-induced OM, but it was not effective in improving the general and oral health-related QoL of patients undergoing HSCT.
Footnotes
Acknowledgments
This study was supported by grants from the Goiás Foundation for Research Support (FAPEG-Grant 2010102670007). The authors thank the Araújo Jorge Hospital, Goiás Combat Cancer Association, Goiânia, Brazil.
Author Disclosure Statement
No competing financial interests exist.