
Abstract
Introduction
B
Curative surgery has been proven to be the most effective treatment for NMIBC, among which transurethral resection of the bladder tumor (TURBT) remains the gold standard. 4,5 Initial TURBT is a crucial procedure in the diagnosis and treatment of NMIBC and is associated with appropriate treatment decisions and follow up strategies. 6 However, optimization of TURBT procedure could be challenging, because substantial morbidities and complications such as obturator nerve reflex, bladder perforation, and intraoperative bleeding may occur. 7 –10
To overcome the limitations of TURBT, various laser types have been used in the treatment of bladder cancer; 2 μm continuous-wave (2 μm CW) thulium laser for bladder cancer resection was first introduced in 2008. 11 Since then, this treatment strategy has demonstrated efficacy and a favorable safety profile in benign prostatic hyperplasia resection and management of NMIBC. 12,13 In a recent report by Wong et al., outpatient laser ablation of NMIBC was confirmed to be safe and tolerable, especially in elderly patients. 14 However, 2 μm CW laser in the treatment of primary NMIBC has not been reported. In this study, we aim to evaluate the efficiency and feasibility of 2 μm CW laser in a prospective, randomized study in patients with primary NMIBC.
Methods
Patients
From January 2006 to December 2010, 400 consecutive patients with newly diagnosed Ta or T1 bladder cancer were enrolled in this study. Those patients were collected and accumulated prospectively. This study was approved by the institutional review board and registered in the Chinese clinical trial registry (ID:ChiCTR-IOR-15006634).
Patients were randomized to receive TURBT or laser vaporesection for bladder tumor (LVRBT). The inclusion criteria for each group were as follows. (1) Patients should have primary single or multiple papillary neoplasms in the bladder with no upper urinary tract abnormalities, so that the confounding bias could be controlled. (2) Additional imaging examinations, such as magnetic resonance urography (MRU) or positron emission tomography(PET)-CT demonstrated the absence of extravesical extension, lymph node metastasis, or adjacent organ invasion. The exclusion criteria for each group were as follows. (1) The biopsy showed evidence of inverted papilloma. (2) The imaging examinations showed extravesical tumor extension, lymph node metastasis, or adjacent organ invasion. (3) The patient could not tolerate the general anesthesia. (4) Other contraindications for the following operation, such as severe cardiovascular or pulmonary disease, or disturbance of blood coagulation. In the TURBT group, patients were treated with standard transurethral resection with bipolar electrocautery system, whereas in LVRBT group, transurethral vaporesction of bladder neoplasm with 2 μm CW thulium laser was performed.
Surgical techniques
Baseline information such as the number of tumors and maximum tumor diameter, as well as the concurrent carcinoma in situ (CIS), was recorded, and a biopsy at the root of the tumor was performed.
TURBT was performed by using an ACMI 25.6 French (F) continuous flow resectoscope with loop electrode. Small size tumors were resected en bloc. Larger tumors were resected separately and completely in fractions, including the exophytic part of the tumors, the underlying bladder wall with detrusor muscle, and the edges of resection area. The specimens from different parts as well as from cystoscopic biopsy were under pathologic examination separately. In the LVRBT group, Revolix™ thulium laser system (LISA Laser Products, Lindau-Katlenburg, Germany) was used in CW mode. A 550 nm bare-ended laser fiber was introduced in the working element of a 26 F continuous-flow resectoscope. After a regular biopsy, vaporesection was started around the tumor with a margin of ∼2 mm. With blunt dissection by a resection loop auxiliary device at the tip of a resectoscope, a complete tumor sample was removed by vaporesection. If a tumor size was >3 cm, it was necessary to incise longitudinally and/or across the lesion and bladder wall at the base into two or more parts. Then vaporesection proceeded toward deeper layers until the underlying bladder wall with detrusor muscle was exposed. Unlike TURBT, to obtain the detrusor muscle that was underlying the tumor, another cystoscopy was repeated and a biopsy was performed from bladder muscle for separate histopathology evaluation. Repeated biopsy at one site was necessary to obtain detrusor muscle for pathologic examination. During the operation, all related complications, such as bladder perforation and bleeding, were recorded. During the early postoperative stage, those complications, including bleeding and infection, were also noted. All things, mentioned above, were performed by the operator.
Postoperative treatment and follow-up
Patients in both groups received continuous intravesical irrigation with sterile water for at least 12 h after initial procedure. The catheter was removed 24–48 h after the procedure. Adjuvant intravesical chemotherapy was given to all patients 1–2 weeks after the initial procedure if uroepithelial carcinoma was confirmed by the pathologists. All patients in this study received an intravesical treatment of 40 mg epirubicin (Pharmorubicin®) once a week for 8 weeks. Approximately 3–4 weeks after the initial procedure, patients who underwent incomplete initial resection (or vaporization), had suspected tumor residue, missing detrusor muscle information, or CIS, had a second procedure for restaging.
All patients received cystoscopy every 3 months during the first 2 years, then every 6 months afterwards. During cystoscopy, a biopsy was taken as a routine practice. The primary end-point of this study was tumor recurrence rate. Meanwhile, the recurrence and progression scores were calculated by European Organization for Research and Treatment of Cancer (EORTC) scoring system. X.-R. Z. and C. F. evaluated the final outcome.
Statistical analysis
The PASS 11.0 (NCSS, USA) was used for sample size calculation. Two independent proportions analyses were chosen to calculate the final sample size, based on the results of preliminary study. Meanwhile, the power of the final results was analysis by non-inferiority tests of two independent proportions tests. The other data were collected by prospective completed data forms, and the following statistical analyses were performed by using IBM SPSS v.16.0.0 (SPSS, Chicago, IL). Difference was considered significant if p < 0.05. The χ2 test, independent samples t test, and log-rank test were used to assess the related clinical variables. Recurrence-free survival was analyzed with the used of the Kaplan–Meier method and the log-rank test.
Results
Patients
Of 400 patients enrolled, 292 were included in our analysis. The profiles of the missing patients is seen in Table 1. There were no significant differences in the remaining patients' general characters and pertinent tumor related characteristics between the two treatment groups (Table 2).
TURBT, transurethral resection of bladder tumor; LVRBT, transurethral laser vaporesection for bladder tumor; MIBC, muscle-invasive bladder cancer.
TURBT, transurethral resection of bladder tumor; LVRBT, laser vaporesection of bladder tumor; CIS, carcinoma in situ; WHO, World Health Organization.
Patients' recurrence and progression scores were calculated by the EORTC scoring system and risk tables recommended by European Association of Urology (EAU) guidelines. 3 No differences were found in recurrence and progression scores between the two treatment groups. The average recurrence scores were 3.47 ± 2.97 in the TURBT group and 4.26 ± 3.54 in the LVRBT group (p = 0.837). The average progression scores in the TURBT and LVRBT groups were 3.91 ± 3.67 versus 4.26 ± 3.54 (p = 0.404).
Recurrence rates
Tumor recurrences were identified in 129 patients (44.2%) during 36 months of follow-up: 61 (42.7%) in the TURBT group and 68 (45.6%) in the LVRBT group [p = 0.608, hazard ratio (HR) = 1.129, 95% confidence interval (CI) 0.71–1.79, power 0.9147]. Two patients (one in the TURBT group and one in the LVRBT group) were confirmed to have residual tumor in the repeated TURBT. Ten patients (six in the TURBT group and four in the LVRBT group) had tumor recurrence 3 months after the initial procedure. Tumor-free survival was 25.16 ± 12.99 months: 25.46 ± 13.18 months in the TURBT group and 24.88 ± 12.85 months in the LVRBT group (p = 0.727, Fig. 1).
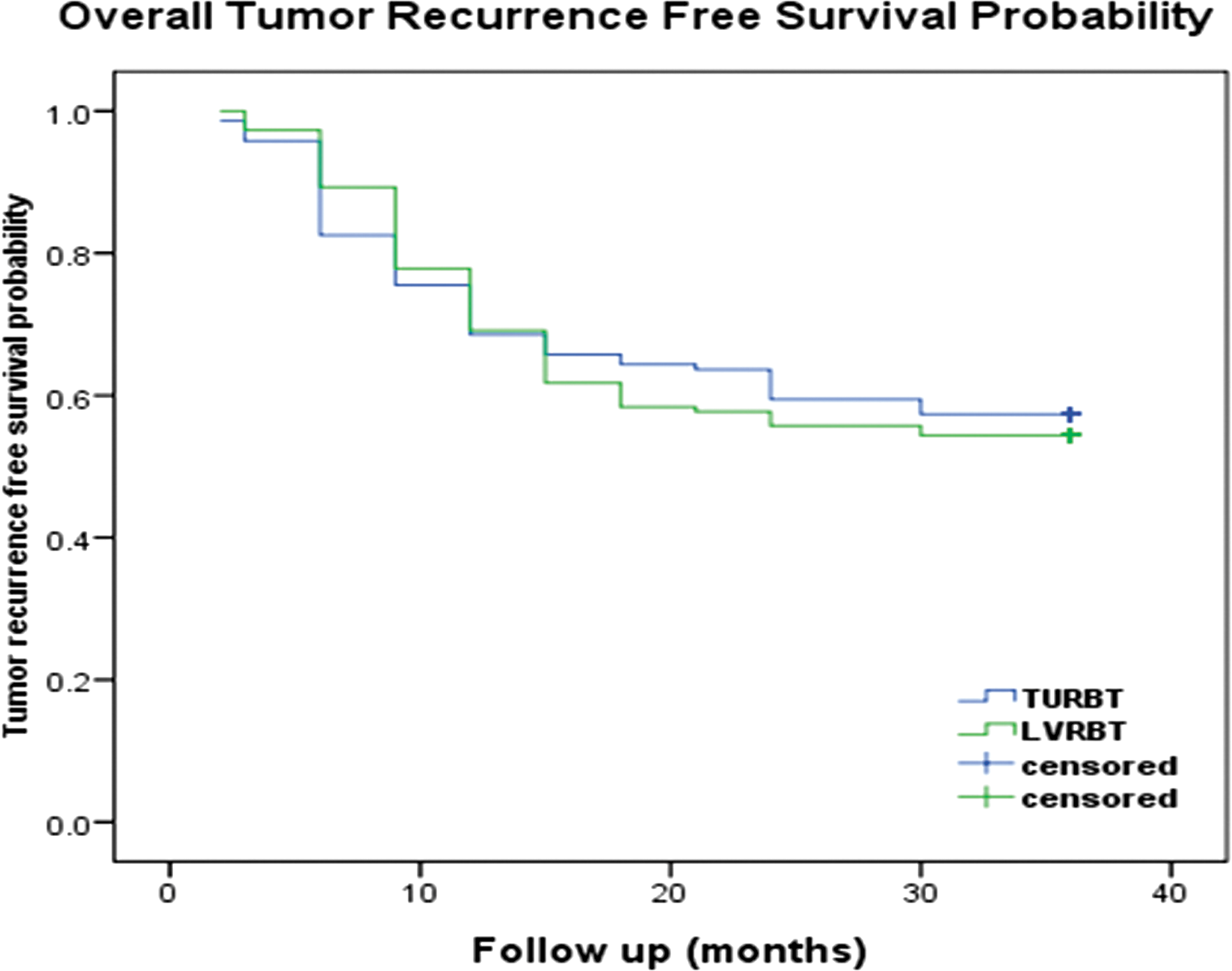
Tumor-free survival for patients who underwent transurethral resection of bladder tumor (TURBT) and laser vaporesection of bladder tumor (LVRBT). Log-rank p value: 0.748; estimated median tumor recurrence free interval: TURBT, 25.4 ± 1.1 months; 95% confidence interval (CI), 23.3–27.6 months; hazard ratio (HR), 1.064; LVRBT, 24.9 ± 1.0 months; 95% CI, 22.9–27.0 months; HR,0.943.
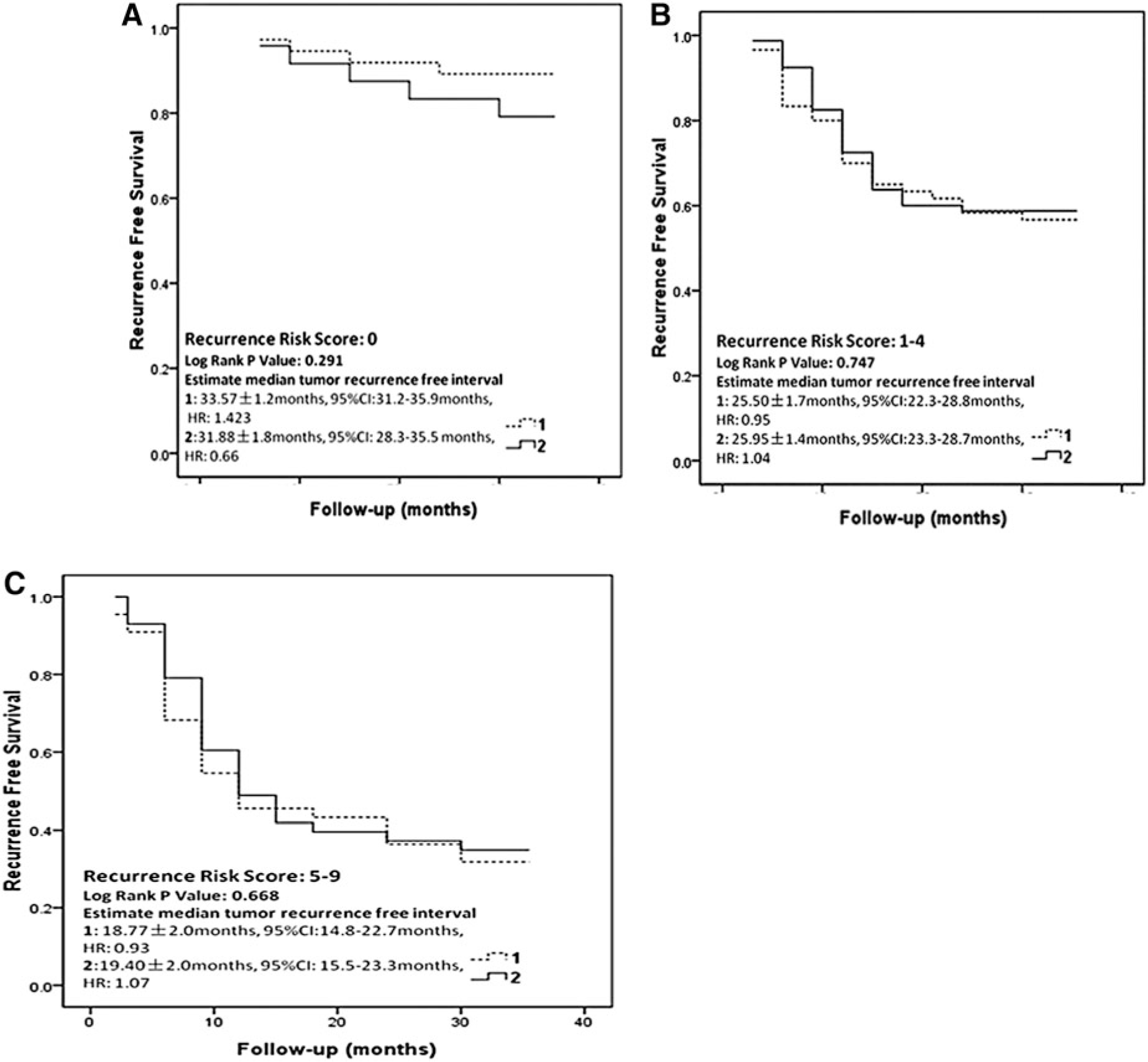
Recurrence rates were further analyzed based on four risk subgroups defined by recurrence and progression scores calculated per scoring system and risk tables recommended by EAU guidelines: low risk (recurrence score = 0), intermediate low risk (recurrence score = 1–4), intermediate high risk (recurrence score = 5–9), and high risk group (recurrence score ≥10). One- and 3-year recurrence rates for each risk subgroup in both treatment groups are shown in Table 3. No statistically significant differences were noted between the two treatment groups.
N/A because of the limited patient numbers.
TURBT, transurethral resection of bladder tumor; LVRBT, laser vaporesection of bladder tumor.
No statistical significant differences were noted in recurrence-free survival in patients who had low, intermediate low, and intermediate high risk (Fig. 2). Only two patients had high recurrence risk at baseline in each treatment group. Statistical analysis was not performed.
Nineteen patients (6.5%, 19/292) had tumor upgrade during 3-year follow-up, 11 patients in the TURBT group (7.7%, 10/143) versus 8 patients (5.4%, 8/149) in the LVRBT group (p = 0.421, HR 0.681, 95% CI 0.27–1.75).
Operation time and treatment complications
The operation time was significantly lower in the TURBT group than in the LVRBT group (28.43 ± 13.19 vs. 31.51 ± 12.80 min, p = 0.044). Six patients in the TURBT group experienced bladder perforation caused by obturator nerve stimulation. The procedure was terminated in one patient because of severe bladder perforation. No complication occurred during procedure in the LVRBT group.
Two patients in the TURBT group extended postoperative continuous irrigation caused by bleeding. One patient in the LVRBT group had the catheter removed 7 days after initial procedure because of anterior urethral injury caused by resectoscope insertion.
A total of 44 patients (15.1%), 17 patients in the TURBT group and 27 in the LVRBT group (p = 0.137, HR 1.315, 95% CI 0.89–-1.95) had a second procedure within 3–4 weeks after the initial procedure. The reasons included suspected incomplete resection with perioperative complications (n = 4, all in the TURBT group), multifocal tumor (n = 13, 4 vs. 9 in each group), and absence of detrusor muscle in the specimen (n = 27). For 27 patients with absence of detrusor muscle, 9 (6.3%, 9/143) were in the TURBT group and 18 (12.1%, 18/149) were in the LVRBT group. The difference between treatment groups was not statistically significant (p = 0.088, HR 1.517, 95% CI 0.88–-2.62). Among those patients who underwent a second procedure, one patient in each group had confirmed residual tumor.
Discussion
The main goals of the initial procedure for primary NMIBC are to make a correct diagnosis and prognosis as well as to remove all visible lesions. Obtaining detrusor muscle underlying the bladder neoplasm provides direction for future treatment and is crucial for accurate prognosis. 15 It was recommended that cauterization should be avoided as much as possible to avoid tissue damage. 6 As a standard procedure in the diagnosis and treatment of NMIBC, TURBT is able to retrieve enough specimens for pathology evaluation, including the exophytic part of the tumor, the underlying bladder wall with the detrusor muscle, and the edges of the resection area.
Successful use of Ho:YAG laser in the treatment of NMIBC has proven the feasibility of laser technology in this disease area. 8,16 The 2 μm CW thulium laser demonstrated advantages over conventional laser. 17 –19 This laser technology has been used successfully in several studies for benign prostatic hyperplasia. 20,21 Its benefit was further confirmed in several clinical and animal studies in bladder-neck contractures, urethral and ureteral strictures, and, possibly, lithotripsy 22 or laparoscopic partial nephrectomy (LPN). 23 We believe that precise tissue cutting and the vaporization capacity of 2 μm CW thulium laser make it possible to retrieve enough detrusor muscle for accurate diagnosis and prognosis in NMIBC.
In our study, superficial cauterized tissues could be easily swept out by using the enucleated plus cold-cup sample mode. Enough detrusor muscle underlying the tumor could be retrieved for pathologic examination by regular cystoscopy. The results in our study showed that no statistically significant differences were noted in specimen integrity between two treatment groups, demonstrating that primary NMIBC could be effectively treated by 2 μm CW thulium laser. Nevertheless, it was noteworthy to emphasize the advantage of using a ring-like attached device in the procedure. For pedunculated tumors, a resection loop could lift the tumor body during vaporesection for better base of tumor exposure in the resectoscope, making it easier to vaporesect the tumor at the bottom. After vaporesection, this ring-like loop could help to eradicate the eschar for muscle tissue exposure.
In our study, tumor-free survival in the two treatment groups was similar (Fig. 2), indicating that 2 μm CW thulium laser vaporesection provided similar treatment effects as those of TURBT en bloc resection for NMIBC patients. We must mention that all patients in this study had NMIBC. Endoscopic surgery did not usually impair their quality of life. Therefore, we choose tumor-free survival duration instead of quality of life as the main point to compare surgical effectiveness between TURBT and LVRBT. However, we have to point out that more patients in the LVRBT group than in the TURBT group had a second procedure because of absence of detrusor muscle. We noticed that most of the cases with missing detrusor muscle were found in the beginning of the study, indicating that our vaporesection plus cold cup method still required a learning curve, and that refining our techniques in using LVRBT treatment is needed.
During surgical resection in TURBT, there is a chance that some tumor cells may be shed and replanted in the bladder. Theoretically, frequent changing of endoscopic equipment in 2 μm CW thulium laser vaporsection could not only prolong the operation time, but also increase the risk of tumor spreading, which may conflict with surgical oncologic principles for tumor resection. In our study, postoperative continuous intravesical irrigation with sterile water was used to minimize this risk. It was thought that by exposing to an intravesical hypotonic environment, deciduous tumor cells might experience dynamic changes, including cell swelling and death. In our study, only 10 patients experienced tumor recurrence during the first follow-up cystoscopy after the initial procedure. The short-term recurrence rate was comparable to what was reported in the study by Brausi et al., with local recurrence rates varying from 3.5% to 20.6% during the first follow-up cystoscopy. 24
However, taking the overall recurrence rates into consideration, in our study, using continuous intravesical irrigation with sterile water was not able to effectively increase treatment outcomes. Most patients in our study were unwilling to have a 5-year cystoscopic follow-up. Therefore, only 3-year follow-up data were collected. In our study, the 3-year overall recurrence rate was > 40%. It was estimated that 5-year recurrence rates might be even higher should the 5-year cystoscopic follow-up data be collected. Our results indicated that continuous intravesical irrigation with sterile water could only be marginally effective in preventing scatter tumor cells spreading during the endoscopic procedure. Immediate single intravesical chemotherapy instillation has been shown to eliminate circulating tumor cells from TURBT and to destroy residual tumor cells at the resection site and from some small unnoticed sites. 25 In Di Stasi et al.'s study, immediate pre-TURBT intravesical electromotive drug administration of chemotherapy has also been effective in patients with primary NMIBC, showing a recurrence rate of 38%. 26 These studies demonstrated that early administration of intravesical instillation of chemotherapy may contribute to the improved disease-free survival and long-term outcomes. Therefore, despite the fact that continuous intravesical irrigation with sterile water after 2 μm CW thulium laser may provide an alternative option in some selected patients who are not eligible for intravesical instillation of chemotherapy or who had postoperative hemorrhage or bladder perforation, an immediate single intravesical chemotherapy instillation is still necessary. However, this study was initiated in 2006. At that time, immediate single intravesical chemotherapy instillation for NMIBC has not been widely accepted. Therefore, we designed continuous intravesical irrigation with sterile water as the standard strategy in our study plan. Although the treatment opinion has changed within the following several years, we still used the first strategy in order to minimize the bias from the different treatment strategies.
In 2006, the EORTC Genito-Urinary Group published the risk tables for NMIBC. 27 Subsequently, this system was incorporated into the EAU guidelines. According to this system, patients were divided into low, intermediate, and high risk groups based on risk scores. 3 However, it is important to note that data used in the EORTC scoring system were from seven randomized trials; in these studies, patients with primary disease were not distinguished from those with recurrent disease. Even though using EORTC risk tables and scoring systems, in Ding et al.'s study 28 indicating that this system could provide valuable prognostic insights into Chinese patients with NMIBC, this study did not provide additional analysis of patients with primary versus recurrent disease. Because only patients who had primary NMIBC were enrolled in our study, previous recurrence status or intravesical chemotherapy history were not valid factors for score calculation. As such, it is possible that our patients had relative lower risk scores compared with that in the EORTC risk table. Only four patients in our study had risk scores ≥ 10 (two in each treatment group). Although our results showed that tumor-free survival was similar in all risk subgroups between two treatment arms, higher recurrence rates were observed in the low intermediate risk (risk score 1–4) and high intermediate risk groups (risk score 5–9) compared with the patients with similar risk scores reported in the EORTC scoring system. It is possible that enrolling only patients with primary NMIBC may impact the effective prognostic value of the EAU risk scoring system. The 3-year recurrence rates observed in our study were higher than the 5-year recurrence rate reported by the EAU risk scoring system, implying that the recurrence or progression score system might need to be modified for its prognostic value in primary NMIBC.
Conclusions
Overall, 2 μm CW thulium laser is feasible for use in the treatment of primary NMIBC, which can provide sufficient diagnostic and prognostic specimens with similar treatment outcomes to those from TURBT. Meanwhile, immediate postoperative intravesical instillation of chemotherapy is necessary for patients who have had 2 μm CW thulium laser tumor vaporesection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.