
Abstract
Introduction
T
Bone surgery is an intervention that generates a great deal of discomfort to the patients, and because of this, research has been conducted with the intention of making the surgery more comfortable and precise, and to offer to the patient a more efficient treatment with fewer physical and psychological traumas. 4,7,8 Now, the most used instrument for osteotomy is the bur mounted on a high speed handpiece which, despite its efficiency, promotes vibrations because of its direct contact with bone to perform the cut, and this induces discomfort to patients. 5,7,9
Therefore, the use of lasers for osteotomy procedures has been proposed. However, for this to be possible, surgical lasers could promote the removal of bone tissue without causing thermal damage. 10,11 In the beginning, bone tissue surgery with lasers was discouraged, because of the histological results that demonstrated a high degree of thermal damage caused by the use of CO2 and Nd:YAG lasers. 12 –14 However, the use of Er:YAG and Er,Cr:YSGG lasers, which have emission wavelengths highly absorbed by water (2.94 and 2.78 μm, respectively), show bone tissue ablation with absence of thermal damage and good patterns of wound healing, 8,15 and because of the noncontact mode of operation, the discomforts caused to patients are reduced. 4,5
Despite the characteristics of the Er:YAG and Er,Cr:YSGG lasers systems, they have promising possibilities for use in bone surgeries, 4,16 and some studies showed that even these can cause some thermal alterations in the bone tissue. 11,17 One study that performed osteotomies on the calvaria bone with the Er,Cr:YSGG laser and bur showed presence of necrotic bone tissue in the vicinity of the irradiated areas. 11 In another study, osteotomies with the Er:YAG laser in the mandible bone were performed, and the bone tissue healing was compared with the osteotomies made by the bur. Zones of necrotic bone and a delay in the bone tissue healing in the osteotomies performed by the Er:YAG irradiation were observed. 17
As the thermal damages have a correlation with the bone healing, 11,17 the use of the ex vivo bone samples can provide a clue about the differences between these lasers in the thermal damage to the irradiated bone. To the best of our knowledge, the comparison between these laser irradiations on bone tissue has not been previously tested. Therefore, the aim of this study was to evaluate ex vivo the bone sections performed with Er:YAG, Er,Cr:YSGG lasers and a high speed handpiece in osteotomy of ex vivo bovine bone blocks, the time taken to perform the section, and the morphology of the surfaces, in addition to the histological description, in order to verify the presence of thermal damages.
Material and Methods
Sample preparation
The body of a fresh bovine mandible was used, and the ramus was sectioned by means of a high precision cutting machine (Buehler Isomet 1000, Lake Bluff, USA) at a speed of 275 rpm. The samples (n = 60; 5 mm wide, 3 mm thick, and 10 mm long) were cut and individually stored in small plastic receptacles and conserved at −20°C in a distilled water solution until treatments were performed.
Experimental groups
The samples were randomly divided into three groups containing 20 blocks each with the aid of a randomization table generated by a computer.
For Group 1 (control), the samples were sectioned with a cylindrical carbide bur N° PM703 (KG Sorensen, São Paulo, Brazil) mounted on a high-speed handpiece (Roll Air III, Kavo do Brasil, São Paulo, Brazil) with external irrigation with distilled water. The bur was changed after every five osteotomies.
For Group 2, the samples were irradiated with the Er:YAG laser (Fotona D. D. Liubliana, Slovenia). The delivery system consisted of an optical fiber, to which an angled handpiece was coupled, and a rigid sapphire tip 17 mm long and an active tip ∼8 mm in length and 1.3 mm in diameter were fitted to it. The emission wavelength was 2.94 μm, and the following parameters were used: 18 frequency of 8 Hz, with 100 pulses/ms and pulse energy of 400 mJ under deionized water irrigation and fluence of 20 J/cm2/pulse. The blocks were irradiated with the laser tip in a perpendicular position at a focal distance of 1–2 mm from the surface.
For Group 3, the samples were irradiated with the Er,Cr:YSGG laser (Waterlase, Biolase Technology, San Clemente, USA). The emission wavelength was 2.78 μm, and the delivery system consisted of an optical fiber to which an angled handpiece was coupled, fitted with a G6 sapphire tip, with a beam diameter of 0.6 mm. The parameters used were as follows: 11 20 Hz, with 140–200 pulses per μs and a pulse energy of 300 mJ under an air/water ratio of 40%/50% and fluence of 10.71 J/cm2/pulse. The blocks were irradiated with the laser tip in a perpendicular position at a focal distance of 1–2 mm from the surface.
Two irradiations/cuts were made in each sample. First, a complete section was performed by means of scanning movements perpendicular to the long axis of the block, until it was completely separated into two fragments. The time required for complete sectioning was recorded in seconds by means of a stopwatch that was only activated when the lasers or bur were in operation. The second irradiation/cut was performed in one of the halves of each section without completing the section, and a 1 mm deep groove was made.
Scanning electron microscopy SEM analysis
Ten samples of each group were dehydrated with increasing concentrations of ethanol (25, 50, 75, 95, and 100%) for 1 h in each concentration. After dehydration, the samples were placed on acrylic plates where a solution of hexamethyldisilazane (HMDS) was applied. First, a solution of 0.8 μL of HMDS + 0.8 μL of absolute alcohol using an automatic pipette (Boeco, Hamburg, Germany) was applied, and the samples were left to rest for 30 min. Afterwards, the solution was removed and the plates were filled with 1 mL of pure HMDS, and the samples were left to rest for 10 min. The specimens were air dried for 20 min. All samples were placed on metal stubs, coded, and kept in a desiccator under a vacuum for 48 h. After this period, the samples were submitted to a sputter-coating process for 120 sec in a Balt-Tec SDC-050 appliance (Jeol-JSM, Tokyo, Japan), and then the samples were coated with gold for analysis under SEM (Jeol-JSM, Tokyo, Japan) with voltage acceleration of 20 Kv. 19 The SEM images obtained were analyzed at 1000× and 2000× magnifications.
The morphological analysis induced by the thermal changes on the bone surfaces were performed on one of the surfaces of each section (lateral to the application) and in the deepest area of each groove performed (frontal to the application). A blinded and calibrated examiner performed evaluation of the thermal damage to the bone surface, using the following index: Score 0, surfaces on which there was no thermal change; Score 1, surfaces with the presence of debris; Score 2, surfaces with the presence of condensed tissue; and Score 3, carbonized surfaces.
Descriptive histological analysis
Ten remaining samples of each group were submitted to decalcification for 30 days in a Morse solution (50% of formic acid +20% sodium citrate) with a pH of 7.4. After this period, the samples were embedded in paraffin and the sections were obtained (6 μm thick), which were afterwards stained by the hematoxylin/eosin (HE) technique and examined under a light microscope (Leica Reichert & Jung Products, Wetzlar, Germany) at 50× magnification. The analysis was performed in the same regions already mentioned regarding the regularity of the cut margins and the presence of thermal changes in the bone tissue.
Statistical analysis
For qualitative analysis of the morphological and thermal changes by SEM, the statistical test χ2 was applied. The reproducibility of the examiner on the SEM and thermal changes analysis of the HE images was assessed using duplicate measurements of the all the samples at 1-week intervals. No differences between the evaluations were shown with the Wilcoxon test (p > 0.05). In addition, Spearman's correlation showed an intra-examiner correlation of r = 0.91 for the SEM analysis, whereas the κ index was 1.00 for thermal analysis.
For analysis of the time required during the section, the Shapiro–Wilk normality test was used to evaluate whether the data were distributed according to the central distribution theorem (p > 0.05). Analysis of variance (ANOVA) was used to compare the groups. When statistically significant differences were found, analysis was complemented with Tukey's test. The significance level adopted was 95% (p < 0.05). The software program Biostat 5.0 (Belém, PA, Brazil) was used to perform statistical analyses.
Results
Analysis of time taken to section the samples
The bur was demonstrated to be the tool that sectioned the bone fragment in the shortest amount of time (p < 0.05), followed by the Er:YAG laser (p < 0.05). The Er,Cr:YSGG laser was the tool that promoted the slowest sectioning in comparison with the other two tools (p < 0.05). Table 1 shows the means and standard deviations of the groups and the statistically significant differences found.
p < 0.05, shorter time than for Er:YAG laser group. One way ANOVA complemented by Tukey.
p < 0.05, shorter time than Er,Cr:YSGG laser group. One way ANOVA complemented by Tukey.
Morphological and thermal analysis by SEM
In the evaluation of the central region of the sulci, it was verified that the specimens irradiated with the Er,Cr:YSGG laser presented a greater degree of thermal damage than the specimens in the bur and Er:YAG laser groups. When the sectioned side was evaluated, it was observed that the bur group presented lower degrees of thermal change than the Er:YAG and Er,Cr:YSGG laser groups (p < 0.05). In addition, the laser irradiation produced more irregular sections than the bur. Tables 2 and 3 show the frequency of distribution of the evaluation index scores of thermal damage to the bone surface from the sulci and sectioned side, respectively. Figure 1 presents representative images originated by SEM from all the groups (1000× magnification).
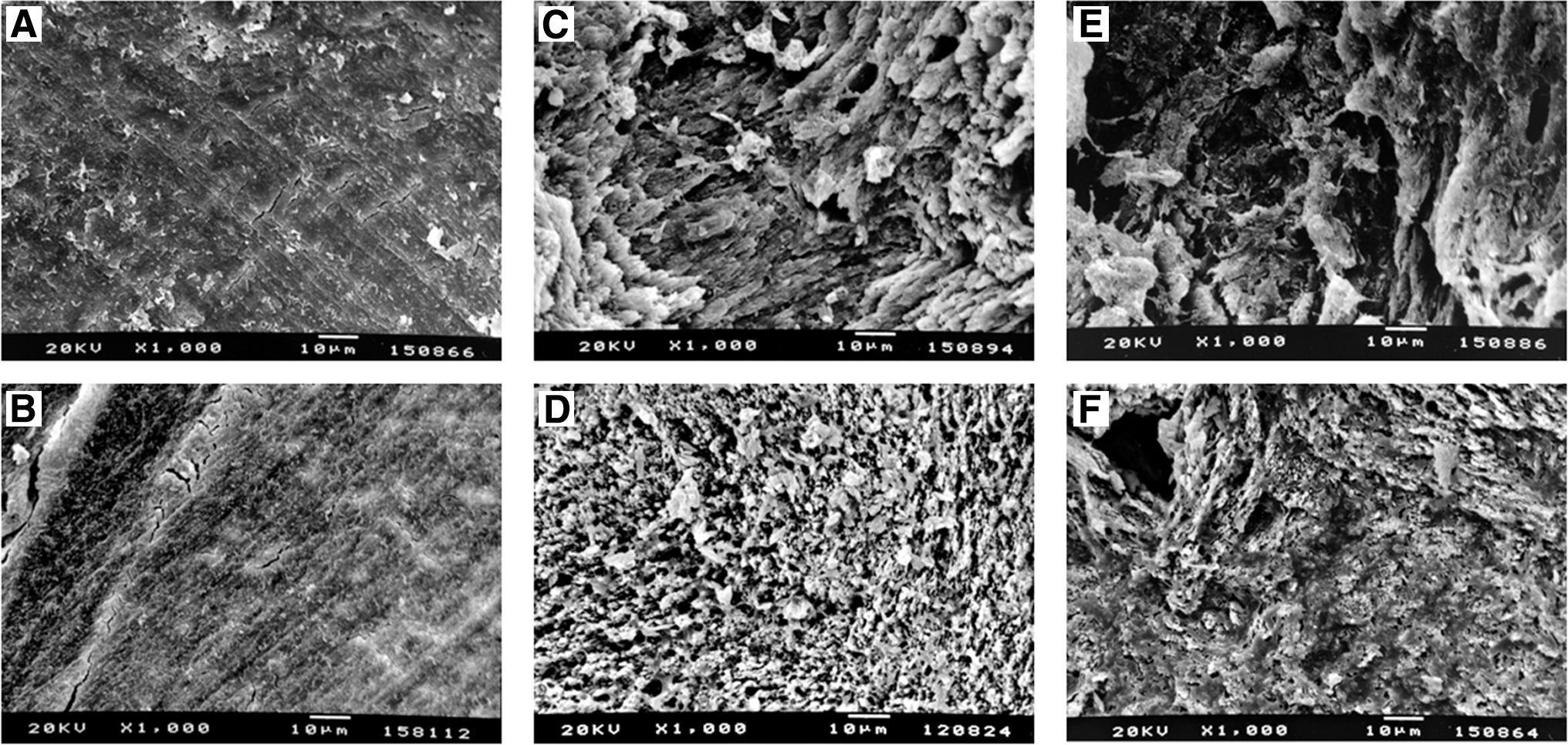
Morphological aspect of bone surfaces after osteotomy with the different tools. (
p < 0.05, lower degrees of thermal changes than in the Er,Cr:YSGG laser group, χ2 test.
p < 0.05, lower degrees of thermal changes than in the laser group, χ2.
Histological analysis
In the histological analysis, it was verified that in the specimens that were sectioned with the bur, the margins were shown to be regular, with 4 of the 10 specimens presenting foci of a band of tissue with a darkened color that represented a thermal alteration of the tissues, whereas in the region of the sulci, a regular cut was verified and foci of a darkened color in 7 of the 10 samples, which demonstrated that they underwent a slight thermal damage. In the group treated with the Er:YAG laser, it was verified that all the specimens presented regular margins, without the presence of thermal damages in the sectioned areas, whereas in the areas of the sulci, irregular ablation without the presence of thermal damage was verified. In the group submitted to treatment with the Er,Cr:YSGG laser, it was verified that the sectioned specimens of bone tissue presented an irregular surface, with 3 of the 10 specimens presenting some degree of thermal damage. In the region of the sulci, it was verified that all the specimens presented irregular surfaces and that three specimens presented foci of thermal damage. The groups irradiated with the laser formed a sulcus in the form of a gap, whereas in the bur group, this sulcus presented a rounded formation. Figure 2 shows representative images of all the groups, which originated with histological analysis (50× magnification).
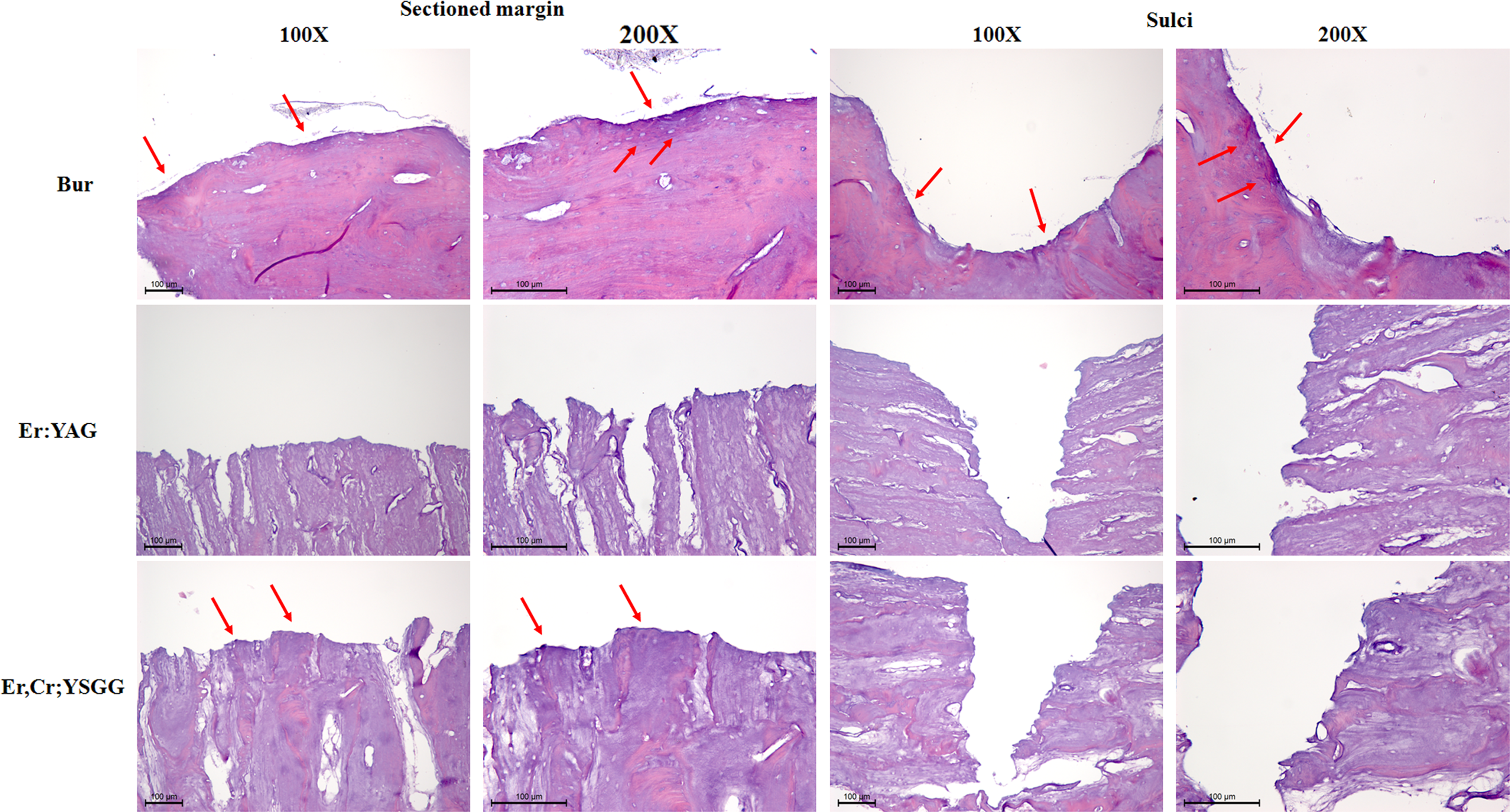
Histological aspect of bone surfaces after osteotomy. Bur A: regular margin with a small area of stronger staining by hematoxylin, which represents superficial thermal damage, was observed at the sectioned side. The sulci presented a regular surface with foci of thermal damage in the bottom of the sulcus, which was shown to have a rounded shape. Er:YAG laser: the sectioned margins presented a regular bone surface with presence of hematoxylin staining with uniform intensity in the entire sample, which demonstrated absence of thermal damage. The sulci presented an irregular surface with absence of thermal damage, and have a gap shape. Er,Cr:YSGG laser: An irregular bone surface with stronger presence of hematoxylin staining on the bone margin was observed at the sectioned side, which demonstrates the occurrence of superficial thermal damage after the use of this laser. The sulci presented an irregular surface with absence of thermal damage, and have a gap shape (Arrows localize the thermal damages). (Original magnifications 100× in first and third columns, and 200× in second and fourth columns.)
Discussion
The results of this study demonstrated that the Er,Cr:YSGG and Er:YAG lasers applied in the noncontact mode were capable of promoting bone tissue ablation; however, in a longer time in comparison with the cut promoted by the bur mounted on a high-speed handpiece. Further, it was verified that the Er:YAG and Er,Cr;YSGG lasers promoted limited superficial thermal damage in the irradiated tissues; however, these alterations did not propagate deeply into the bone tissue blocks.
One of the great limitations that has been revealed in other studies with regard to the use of Er:YAG and Er,Cr:YSGG lasers for bone tissue ablation is the time required for removal of the desired tissue in comparison with burs mounted on high-speed handpieces. 4,20,21 This limitation has been a reason for discouraging the clinical application of lasers. 23 However, the alteration in the pulse mode of lasers was shown to be an alternative for accelerating bone tissue ablation, and, thus, to resolve this limitation. 7,8
Another important fact verified in this study was that the Er:YAG laser promoted significantly faster bone ablation than that obtained by the Er,Cr:YSGG laser. Despite the low disparity in the wavelength values of these two lasers, water absorbs approximately two times more Er:YAG laser energy than that of the Er,Cr:YSGG laser, which may have influenced the ablation speed in our study. 22
The thermal damage to bone tissue caused by irradiation with lasers has also been a topic of discussion with reference to limitation on the use of lasers for bone ablation. High intensity lasers, such as CO2 and Nd:YAG, promote high degrees of thermal damage to irradiated bone tissues; 12 –14 however, this fact was not found in our study and in other studies that have evaluated bone ablation with Er:YAG and Er,Cr:YSGG lasers. 6 –8,23 –25 The discrepancy in these results occurred because of the different modes of ablation promoted by the different types of lasers. The Nd:YAG and CO2 lasers promote photothermal ablation, in which ablation occurs by the melting of the hydroxyapatite crystals, 12 –14 whereas the Er:YAG and Er, Cr:YSGG lasers promote thermomechanical ablation, which occurs because of an abrupt evaporation of water that induces microexplosions in the interprismatic substance, causing detachment of the hydroxyapatite crystals. 8,15,23,24 This type of ablation promoted by the Er:YAG and Er,Cr:YSGG lasers occurs because of the high degree of absorption of the laser irradiation by water presented into the hard tissues because of the wavelength of light emitted by these lasers, which induces the hard tissue ablation at lower temperatures. This fact justifies the limited thermal damage promoted by lasers that promote thermomechanical ablation. 5,11,23
In our study, the presence of superficial thermal damage promoted by the Er:YAG and Er,Cr:YSGG lasers was verified in the images obtained by SEM, whereas there was not damage of this type caused by the burs mounted on a high-speed handpiece. However, the dissipation of this thermal damage in the depth of the samples was verified in only three specimens irradiated with the Er,Cr:YSGG laser, a result similar to that found with burs mounted on high-speed handpieces. The high level of laser light absorption by water prevents the dissemination of laser light energy to the deeper layers, with a concentration of this energy occurring in small portions of superficial tissue. 15,23 Therefore, this concentration of energy may explain the superficial thermal damage verified with both lasers, but the limited dissemination of this thermal damage into the depth of bone tissue. Our findings are in accordance with the data obtained in other ex vivo studies, which showed no thermal damage induced on bone tissue irradiated by the Er:YAG 16,26 and Er;Cr:YSGG. 15,17 In addition, a clear and precise cut with irregular edges was obtained after the use of the both lasers for osteotomy in bone samples, 15,26 as was observed in our study.
The histological and morphological findings in our study cannot be directly related to the wound healing events that occurred after surgical intervention in bone tissue with Er:YAG and Er,Cr:YSGG lasers; however, some histological studies have discussed bone repair after laser irradiation. A study that evaluated the effect of Er,Cr:YSGG lasers on bone healing in the calvaria of rats verified that the repair occurred in the same way as the repair after intervention with burs mounted on high-speed handpieces, despite the thermal damage observed with the use of lasers. 11 Another study that evaluated the repair in sheep tibias after sectioning with Er:YAG lasers and piezoelectric ultrasound demonstrated that bone repair occurred in a similar manner with the two tools, and that there was no thermal damage in the Er:YAG laser group. 8 Despite the thermal damage found after irradiation with the lasers in our study, it is probable that this damage did not interfere negatively with the bone healing process, as has been observed in other studies. 11,23 –25 Further, it is probable that the irregularities observed after irradiation with the lasers in our study would be beneficial to healing because they facilitate adhesion of the fibrin network, which represents the first event of hard tissue healing. 14,26,27
According to the literature, to date, there has not been any study that directly evaluated bone ablation promoted by Er:YAG and Er,Cr:YSGG lasers and by a bur mounted in a high-speed handpiece. However, this research was limited to an ex vivo study, in which only one parameter of pulse and irradiation energy was tested for each of the lasers, and the aim was not the reproduction of a clinical situation itself. In addition, the thermal effects were analyzed using indirect methods, and the histological analysis was descriptive. Our histological and morphological findings cannot provide an inkling of projections as regards healing. Therefore, further studies are necessary to histologically elucidate healing events and thermal damage induced in bone tissue by Er:YAG and Er,Cr:YSGG lasers, and the behavior regarding the time of ablation, surgical access, and control of ablation in different clinical situations.
Conclusions
In view of the preliminary results presented in this pilot study, we conclude that the Er:YAG laser induced the lowest degree of superficial thermal damage in bone tissue after osteotomy; however, the time required to perform the osteotomy was significant shorter with use of the bur. In addition, the laser irradiation promoted a more irregular bone surface than that in the bur group after osteotomy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.