
Abstract
Introduction
B
In order to accommodate the growing number of osteonecrosis cases associated with other antiresorptive and antiangiogenic therapies, the American Association of Oral and Maxillofacial Surgeons (AAOMS), in a position paper from May 2014, changed the term to “medication-related osteonecrosis of the jaw” (MRONJ). 6
The prevalence of MRONJ in patients under oral BP therapy (BPT) for osteopenia, osteoporosis, and Paget's disease is significantly lower (from 0.1% to 0.21%) than in those treated intravenously for multiple myeloma and bone metastases (from 0.7% to 6.7%). 6
MRONJ therapy remains an unresolved problem, and there are no evidence-based guidelines on the management of this disorder. 7 The different proposed conservative and surgical treatment regimens are associated with contradictory success rates. 8 However, the increased experience with MRONJ management suggests that surgical therapy can halt the progression of the disease, and can allow a histology-based diagnosis of the osteonecrosis. 8
A treatment success rate of >80% was reported in literature for different surgical approaches. 9 –14 Moreover, the results obtained by the authors using a surgical approach with Er:YAG laser are significantly different than those obtained using a medical conservative treatment or a traditional surgical approach. 15,16
In 2012, the authors reported a clinical improvement of 96.55% and a complete mucosal healing of 89.65% in a group of patient surgically treated with Er:YAG laser and Nd:YAG low-level laser therapy (LLLT). 16 These results were statistically higher than those obtained in groups of patients treated only with medical therapy, with medical therapy and LLLT, or with medical therapy and conventional surgery. Nd:YAG LLLT causes a biomodulation of soft and hard tissues that consists of different effects, particularly anti-inflammatory, biostimulating, antibacterial, and analgesic. The biostimulating effect acts on the immune system and on the collagen tissue, increasing proliferation and activity of fibroblasts, on the epithelial tissue increasing cellular turnover, and on bone increasing proliferation and activity of osteoblasts and the amounts of calcium and alkaline phosphatase. 17,18
One of the difficulties typically encountered during the surgical removal of a MRONJ is the precise individuation of the necrotic bone margins. 19,20 However, the complete removal of osteonecrosis seems to be essential for avoiding recurrence or progression of the disease. 8
A technique recently used to discriminate necrotic from viable bone is fluorescence induced by tetracycline and stimulated by an appropriate excitation light. In order to standardize the surgical treatment and reduce its invasiveness, some authors proposed tetracycline fluorescence-guided bone resection, with very high success rates. 21,22
The autofluorescence (AF) examination is currently used to detect soft tissue dysplasia and malignancies. The fluorophores in the normal oral mucosa produce an emission of green AF. On the other hand, alterations in the stromal architecture of dysplastic tissue are associated with a loss of autofluorescence (LAF). 23 A recent report suggests that vital bone is autofluorescent, whereas necrotic bone lost AF, induced by a fluorescence lamp. 24
The aim of this article is to describe an AF-guided surgical approach based on the use of Er:YAG laser and Nd:YAG LLLT.
Case Report
A 73-year-old male patient was affected by a multiple myeloma for which he received 24 infusions of zoledronic acid and corticosteroids. General medical anamnesis did not disclose any relevant pathology. The patient was diagnosed with a Stage III osteonecrosis of the left maxilla not related to dental surgical interventions. The dental anamnesis revealed the spontaneous loss of canine and first premolar teeth 4 months before.
According to the AAOMS staging system, Stage III indicates exposed and necrotic bone or a fistula that probes to bone with pain, infection, and at least one of the following: exposed and necrotic bone extending beyond the region of alveolar bone resulting in pathologic fracture, extraoral fistula, oral antral or oral nasal communication, or osteolysis extending to the inferior border of the mandible or sinus floor. 6
A fistula at the same side of the lesion could be detected on the alveolar edentulous ridge (Fig. 1A). As shown in a computed tomography (CT) scan, the necrosis massively involved the left maxillary sinus, resulting in face swelling, pain under compression, and the other typical symptoms of sinusitis (Fig. 1B).
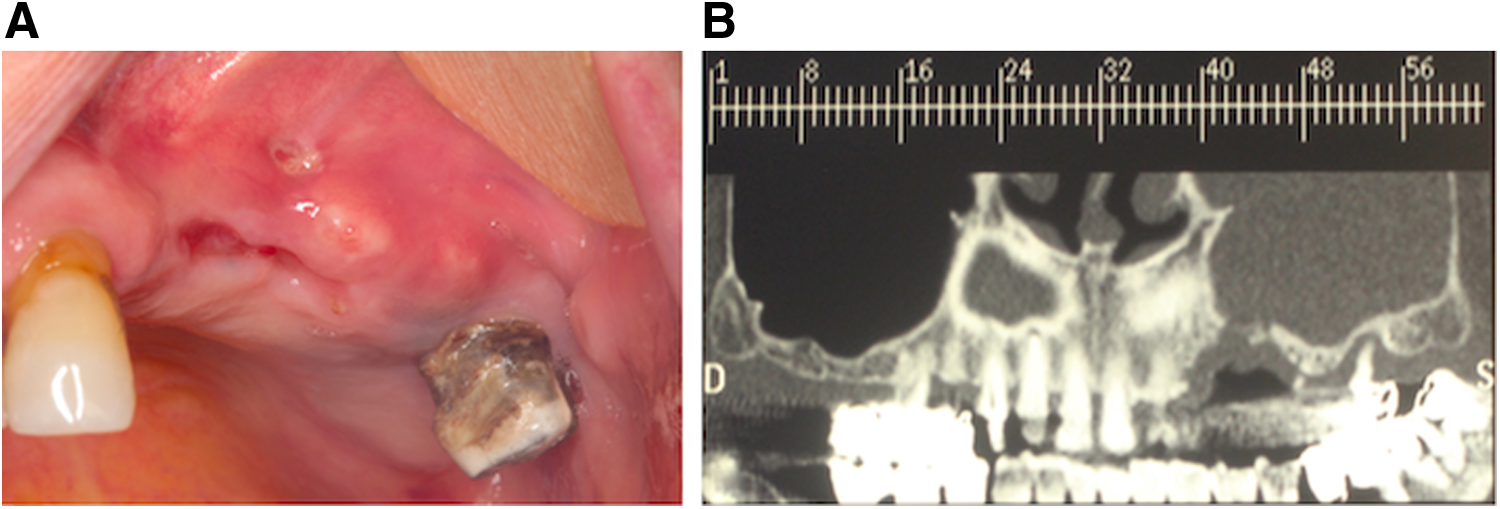
Stage III osteonecrosis of the left maxilla:
Surgical technique
The surgical treatment was performed with the patient under local anaesthesia. Antibiotic therapy with amoxicillin (2 g/day) and metronidazole (1 g/day) was administered from 3 days before to 3 weeks after intervention. No preoperative tetracycline labelling was performed. After bone exposure through the mucoperiosteal flap, the VELscope™ (LED Medical Diagnostics Inc., Barnaby, Canada) system was used to induce and visualize AF of the maxillary bone. It was evident that necrotic bone areas showed no or only pale AF (Fig. 2A and B).
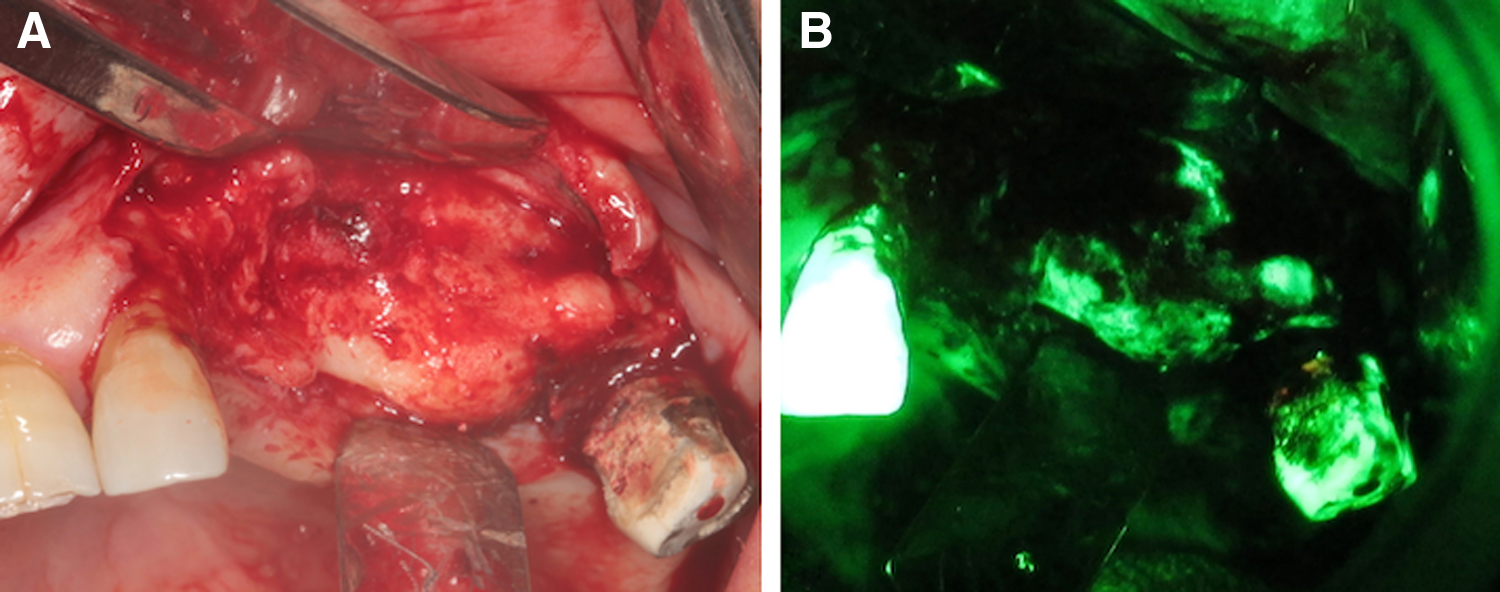
Surgical field after mucoperiosteal flap elevation:
Osteotomy was performed through Er:YAG laser (Fidelis Plus®, Fotona - Slovenia) (Parameters: 300 mJ, 30 Hz, fluence of 60 J/cm2). After the removal of the necrotic bone block, AF visualization was used to guide the marginal bone osteoplasty. The maxillary sinus was completely cleaned from infected tissue and sinusal mucosa. Osteoplasty was performed through the use of a traditional ball-shaped bur that is not traumatic to soft tissues and is useful to remove sharp angles of bone.
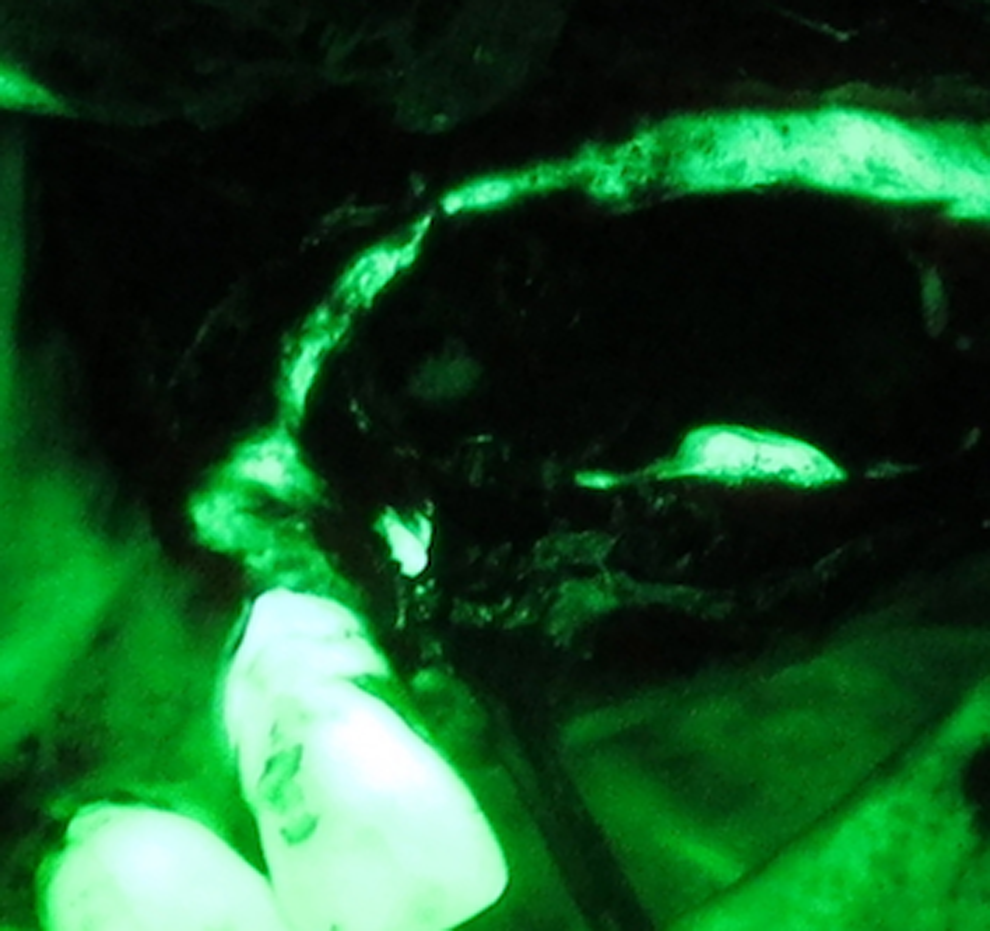
The AF image obtained after osteoplasty showed an evident appearance of fluorescent bone surrounding the maxillary sinus antrum (Fig. 3A and B). According to the AF image guide (Fig. 3B), Er:YAG laser was used for the vaporization of necrotic bone, up to the comparison of healthy bone.
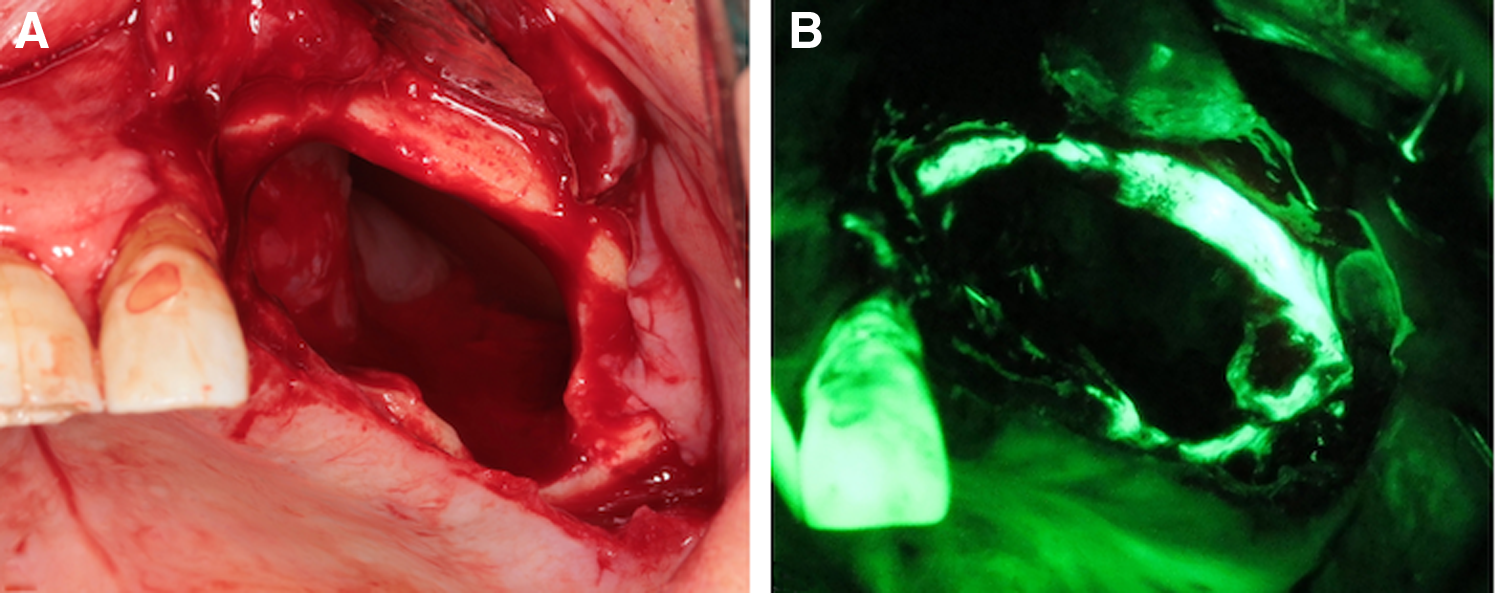
Surgical field after osteoplasty performed through traditional ball-shaped bur:
This laser is useful in the removal of residual bone after osteoplasty (Fig. 4). Moreover, through minimally invasive action, it is possible to act in the areas where nonfluorescence or hypofluorescence has been displayed (Fig. 5).
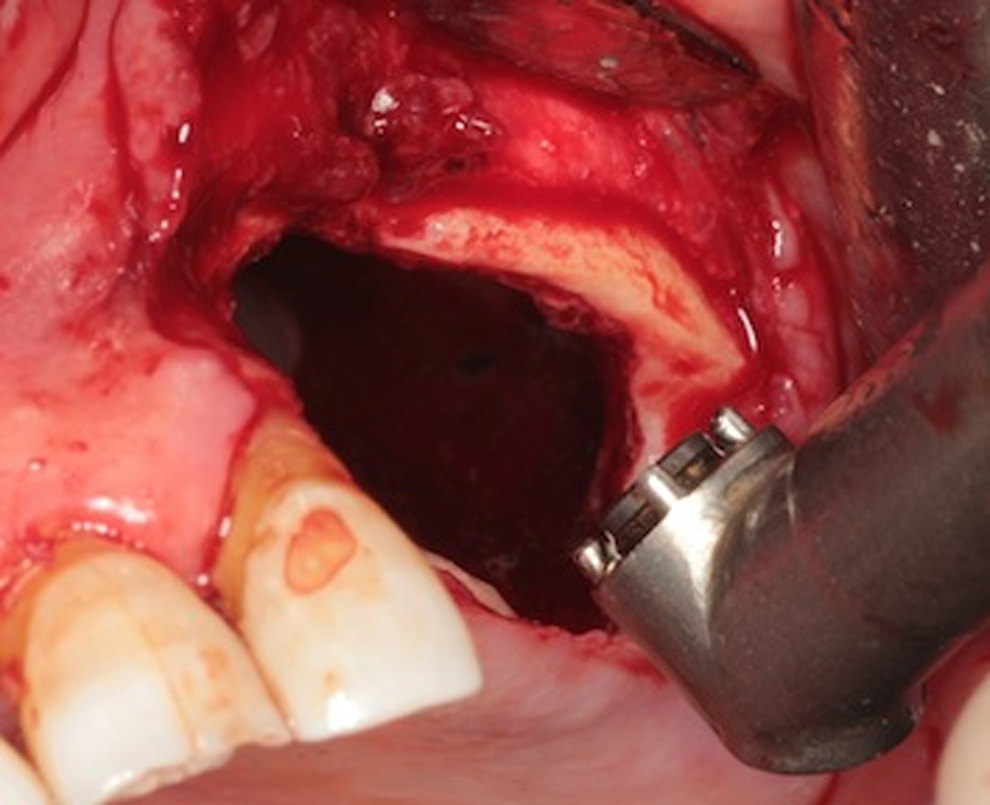
Er:YAG laser evaporation creating bone microperforations in order to stimulate vascularization and pomote healing and attachment of the soft tissue.
Autofluorescence (AF) image after Er:YAG evaporation: appearance of hyper-fluorescence in the area distal to the incisive tooth.
The patient received intraoperative irrigations with povidone iodine solution 10% and application of LLLT (Nd:YAG laser, 1064 nm, Fidelis Plus, Fotona®, Slovenia – power, 1.25 W; frequency, 15 Hz; diameter of the fiber, 320 μm) which was administered in nonfocused mode, at 2 mm distance from the tissues, for 1 min (power density, 1562.5 W/cm2; fluence, 7 J/cm2), repeated five times.
A tension-free wound closure was achieved using continuous locked suture. The patient received weekly applications of LLLT for 3 weeks after intervention. After 7 months of follow-up, the complete mucosal healing was evident and the patient was free of symptoms (Fig. 6). The follow-up orthopantomography (OPT) shows no signs of osteonecrosis (Fig. 7).

Complete mucosal healing after 7 months of follow-up.

Orthopantomography (OPT) after 7 months of follow-up: no signs of osteonecrosis.
Discussion
According to the outcomes defined by Ristow and Pautke, 24 a successful surgical therapy of MRONJ will be achieved if (1) histological workup highlights the complete removal of the necrotic bone, (2) the mucosa is closed, and (3) the patient will remain free of symptoms no later than 4 weeks after the operation.
In the case presented here, all those results are well acknowledged. In particular, 3 weeks after the interventions, complete mucosal healing and the absence of symptoms were evident. Six months after surgery, OPT showed no radiological signs of bone necrosis or signs of sinusitis.
A surgical approach with Er:YAG laser is associated with significantly better results when compared with medical treatment and a traditional surgical approach. 15,16,25,26 Er:Yag laser is used with a distilled water irrigation system, thus reducing the thermal damage to the adjacent tissue. It does not produce coagulation or carbonization, and enables avascular portions of the bone to be clearly distinguished from those that are still vascularized.
Each spot of the laser induces a vaporization of 0.1 mm of tissue. Er:YAG laser produces a gradual and safe ablation of the necrotic areas until healthy bleeding bone is detested. Particularly, the minimally invasive technique of bone evaporation at the end of the procedure is used to create microperforations in order to stimulate new vascularization and promote soft tissue attachement. 27 –29 The additional advantages of laser surgery and postoperative LLLT compared with traditional surgery are the bactericidal and biostimulating actions, with a better healing and postoperative course in terms of less pain and better quality of life. 16
All reported surgical techniques (e.g., laser or traditional debridement/resection) cannot be standardized because of the lack of guidance in defining surgical margins. 8 At the moment, the extent of surgical debridement/resection is defined mainly through radiological diagnostic images (e.g., CT scans, nuclear magnetic resonance), and through subjective intraoperative values including bone color, texture, and bleeding. 30,31 Some authors, such as Ristow et al. reported that bone bleeding is not always correlated with histological findings of vital bone. 8
Because of its affinity to calcium, tetracycline is incorporated into the remodelling and apposition areas of the bone. Therefore, it is incorporated into viable but not into necrotic bone, and can be visualized using an excitation light of 390–430 nm. 32,33
Ristow and Pautke suggested that vital bone can be highlighted because of its AF. 24 This phenomenon was obtained through a blue spectrum excitation light (400–460 nm) and authors such as Fleisher et al. reported that the same effect was not obtained using an ultraviolet spectrum excitation light (e.g., Wood's lamp; 365 nm). 34 A blue spectrum excitation light device is the Visual Enhanced Lesion scope (VELscope) system.
The VELscope™ system consists of a noninvasive device designed to visualize early mucosal changes using the principles of tissue AF. A similar effect of LAF has been shown for necrotic bone tissue. 22,24 However, there are no explanations as to why necrotic bone seems to lose AF. It has been speculated that this could be caused by alterations in the extracellular calcified osteoid matrix or in the bone cells. 24 In our opinion, it can be stated that viable bone AF exists, and that an LAF seems to be present in areas of necrotic bone in patients affected by MRONJ.
VELscope™ intraoperative examination seems to be a suitable guide during surgical debridement/resection of MRONJ. The technique is not invasive, easy to apply, and independent of the subjective impression of the surgeon.
Conclusions
To the best of our knowledge, the AF-guided surgical approach performed with Er:YAG laser and Nd:YAG LLLT has not been previously reported.
Taking into account the demonstrated advantages associated with laser therapy compared with traditional surgery, and the possible effectiveness of the AF in highlighting surgical margins, this approach would probably achieve excellent outcomes. Further studies, particularly controlled clinical trials, are necessary in order to validate and standardize the surgical technique reported here.
Footnotes
Author Disclosure Statement
No competing financial interests exist.