
Abstract
Introduction
T
There is scarce evidence relating to such data within pediatric dental patient groups. What little research exists in pediatric dentistry would suggest that fear is the most frequent emotion in general dental practice (estimated frequency ranging between 6% and 52%). 2,6
It is well recorded that injected anesthesia and the turbine handpiece with a bur are the two most disliked therapeutic instruments. 7 –10
Alternative treatment techniques with different degrees of probability of success and different abilities in anxiety and pain attenuation or suppression may be considered. Examples are hypnosis or conscious sedation with nitrous oxide and oxygen. 11 –16
Some treatment options are not completely proven or verified (i.e., different brands of electrostimulation or electronic anesthesia) or have unpleasant side effects (some topical anesthetics) or are potentially harmful (total anesthesia, conscious sedation with drugs and/or intravenous sedation). 7
Inasmuch as anecdotal claims abound surrounding anxiety, and research into such claims require objectivity and scientific rigor, two different useful techniques to obtain dental analgesia have been described. 17,18
1. The Rabbit (or Hare) Technique, in which the laser is set to high power levels (average power 3–4.5 W, 15 Hz), able to perform hard tissues ablation. This is maintained during the entire treatment of cavity preparation. Initially, the beam is “defocused” (beyond a laser beam focal distance) at 6–10 mm from the tooth (energy density is low and takes advantage of possible low-level laser photobiomodulation analgesic effects) and the delivery tip is moved around the accessible tooth neck. The delivery tip is gradually brought closer (up to 1 mm from the dental surface) prior to tooth ablation. At this point, if the patient feels some discomfort it is possible to withdraw the tip. During tooth tissue ablation, as soon as the beam passes through the enamel and reaches the dentin, the tip is withdrawn from the target; irradiation is correspondingly defocused, power density is thereby reduced and cavity preparation is completed.
2. The Turtle (or Tortoise) Technique, in which the delivery tip is placed initially at 1 mm from the tooth surface and is kept at this distance during the cavity preparation. A low power (1.5–2 W, 30 Hz) is set in order to obtain analgesia and to offer a lower risk of discomfort. The energy is gradually increased up to a sufficient level able to achieve tissue ablation, and this is continued until enamel ablation is complete. When the dentin is reached, the power is lowered to the initial level and the cavity preparation is completed. 17,19
This latter technique is considered the most reliable for minimizing dental sensitivity, because the initial use of low energy allows the pulp to gradually adapt to laser irradiation. Studies would suggest that it is better tolerated by the patient and has been reported to be more effective for obtaining dental analgesia. 17,19
Aim of this research is to evaluate which are the techniques and optimal parameters of Erbium Chromium Yttrium Scandium Gallium Garnet (Er,Cr:YSGG) laser that allow the performance of a predictable painless (or with very limited discomfort) restorative treatment without the aid of injected local anesthesia, in order to obtain patient comfort, cooperation, and compliance.
Materials and Methods
A total of 30 patients (n=15 male, n=15 female), 9–75 years old (average. 37) were treated in a private dental practice and 30 cavities were treated. Each patient had only one cavity treated in permanent teeth as follows: Upper: Two central and eight lateral incisors/one canine/three premolars/six molars Lower: one central incisor/one premolar/eight molars Breakdown of cavity design (Black's classification): 12 Class I/5 Class II/7 Class III/6 Class V
Prior to treatment, it was explained in detail to the patient (or the parents for underage patients) how the treatment would be performed. A written informed consent was obtained.
The laser used for cavity preparation was the Er,Cr:YSGG Waterlase iPlus laser (2780 nm) - Biolase Technology, Irvine, CA. (For laser specifications, see Fig. 1).
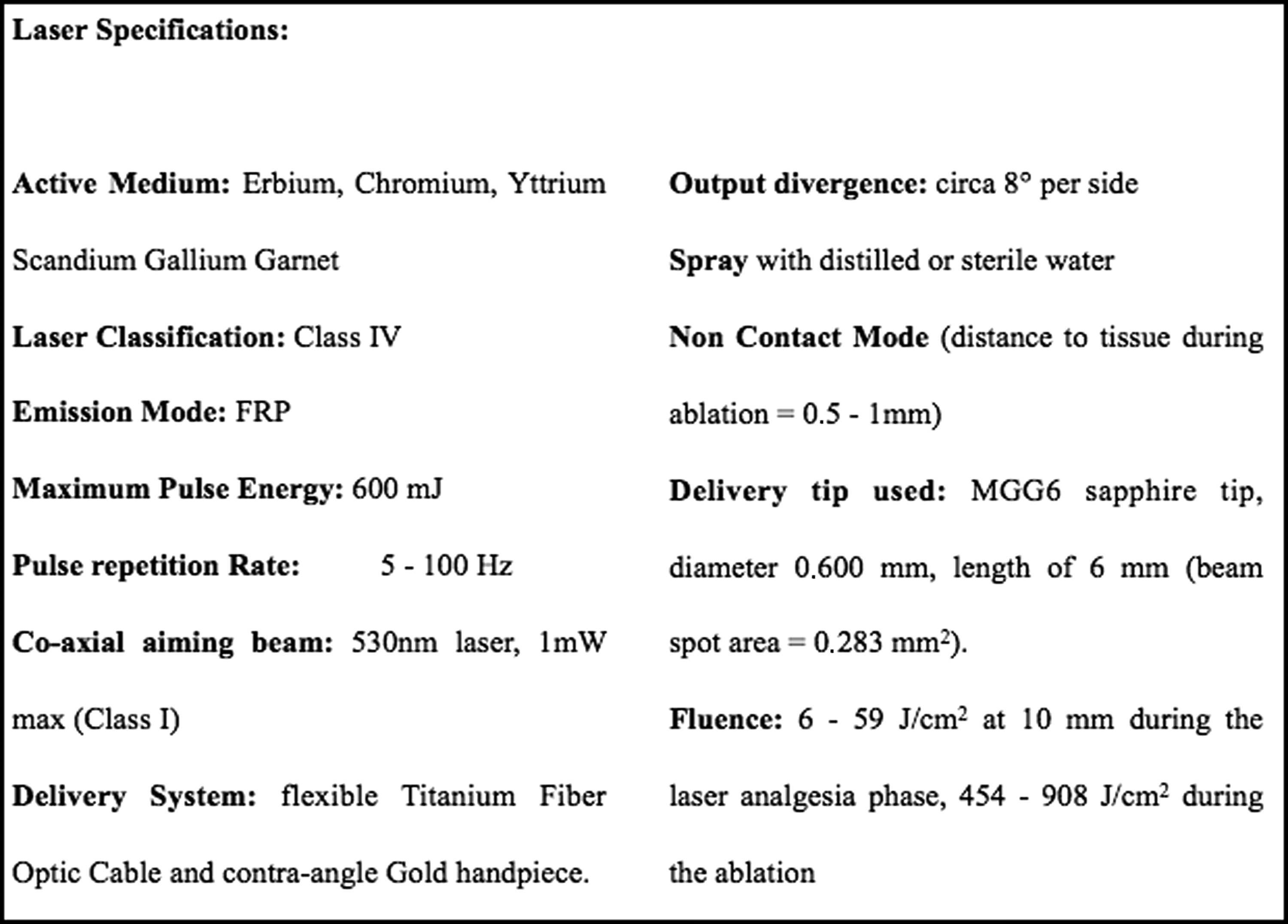
Laser specifications. FRP, free running pulse.
The delivery tip used was the MGG6 sapphire tip, diameter 0.600 mm, length, 6 mm (beam spot area=0.283 mm2).
An Electric Pulp Tester (EPT) (Digitest II Parkell Inc. - Edgewood, NY) was used to verify pretreatment dental vitality and to evaluate the variation of intra- and post-treatment dental sensibility obtaining a numerical value proportional to the delivered current intensity, and depending upon the level of dental sensibility perceived by the patient.
In order to obtain tooth analgesia a combination of the Rabbit and modified Turtle Techniques was used.
The study was performed adopting the following sequence: 1. Preliminary pulp test using the EPT 2. Beginning of dental analgesia induction using power of 0.1 and then 0.2 W (energy per pulse 10 and 20 mJ), for 30 sec each (without air/water spray), 10 Hz, tip at 10 mm from the tooth using a spacer. Subsequently, the power was increased to 0.5 and then to 1 W (33 and 67 mJ) for 60 sec each, with a spray of 15% water (∼10 mL/min) and 20% air, 15 Hz, keeping the same distance. 3. Hard tissues were preconditioned with 2 W for 30 sec, spray 50% water (∼20 mL/min) and 80% air, 15 Hz, tip at 1 mm from the tooth. The laser was defocused if the patient felt discomfort. 4. EPT to evaluate the presence of analgesia and establish how the dental sensibility threshold had changed. 5. Preconditioning and beginning of enamel ablation with 3 W for 30 sec (same as those listed in point no. 2) 6. Enamel and dentin ablation with 3–4 W 7. Preparation completion and smear layer removal with 2 W 8. EPT at the end of preparation to evaluate if dental sensibility further changed 9. EPT after 15–20 min from the end of cavity preparation to evaluate if analgesia was finished
The entire period of laser analgesia induction had an overall duration of 3 min 30 sec (210 sec). (See Fig. 2. For a summary of the protocol used in this research.)
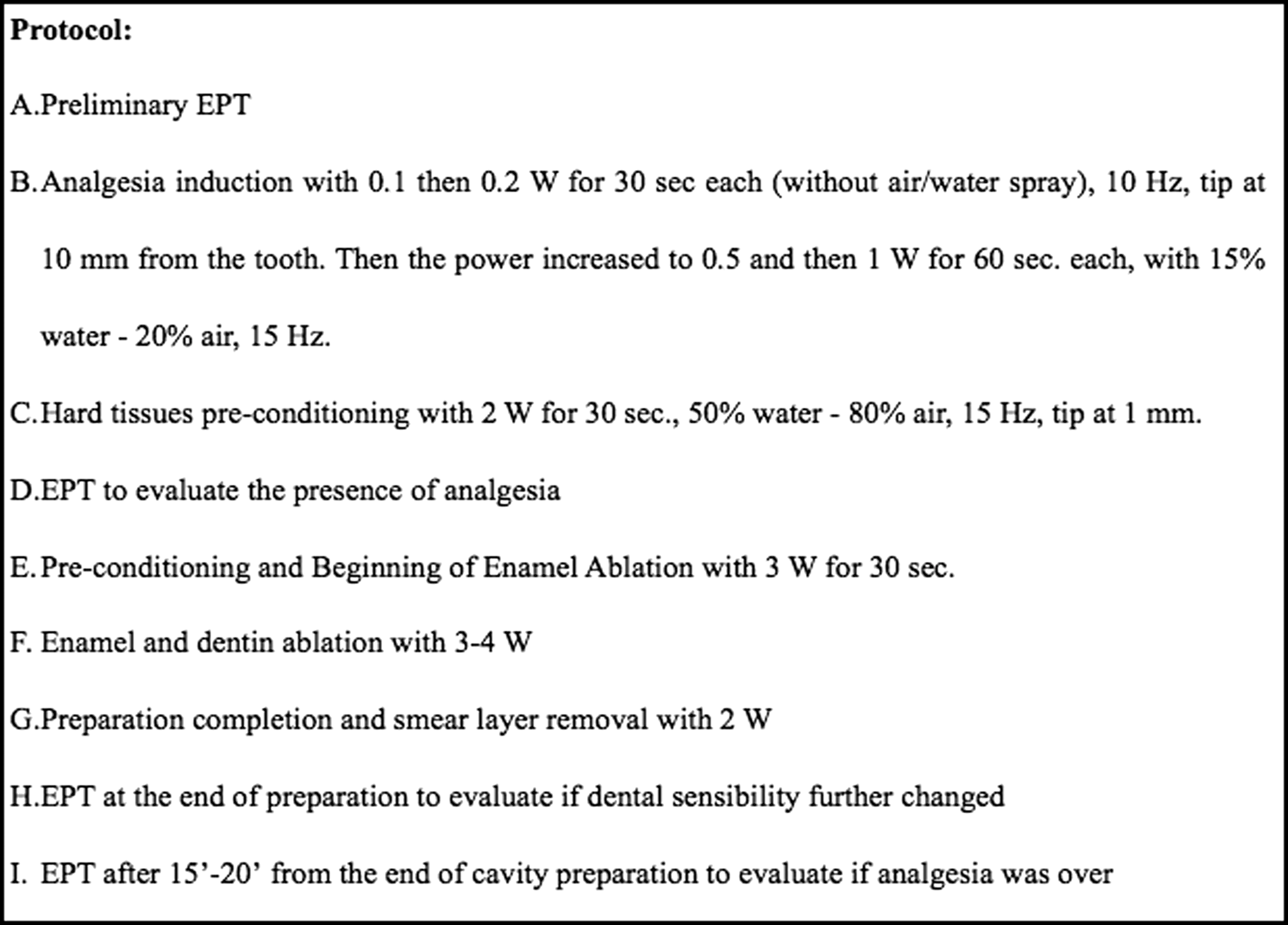
Protocol used for painless conservative treatment. EPT, electric pulp tester.
To correctly perform laser-induced analgesia, it was necessary to maintain a distance of 10 mm from the tooth, 17,18 using a mechanical tube spacer. Figure 3 shows the spacer positioned on the handpiece.

The spacer positioned on the handpiece and used to maintain the tip at 10 mm from the tooth neck.
In this way, it was initially possible to obtain very low energy density (only 6 J/cm2 with movement) and average power density (1 W/cm2), thereby allowing the pulp to progressively adapt and achieve analgesia without risking painful stimuli.
To evaluate the pain perception and the level of anxiety baseline two pain scales modified on purpose [Visual Analogue Scale for adults, Visual Numeric Score/Wong Baker and Children's Fear Survey Schedule - Dental Subscale (CFSS-DS) for children] were used in order to obtain a subjective measurement.
The CFSS-DS was used for children. 2,20 –22 A further element – a pain intensity scale – was added and patients were asked to complete their response after the completion of therapy. This scale depicts six “smile” graphics. The child is requested to choose one of these or a level between them which best represents the level of discomfort or pain experienced.
Inclusion criteria within this study were: • Carious lesion not penetrating into the pulp chamber in a permanent tooth without symptoms • No exposure of the vital pulp • Absence of periodontal impairment • Patient asking to avoid local anesthesia • Patient not in therapy with neurological, sedative, analgesic and/or anti-inflammatory drugs, and neither sedated nor anesthetized.
Restorations were placed using Optibond FL total-etch adhesive system (Kerr, Orange CA), composites Enamel Plus HFO (Micerium, Avegno, Genova Italy) for front teeth, and Herculite XRV Unidose (Kerr, Orange CA) for posteriors.
Results
The laser treatment, including the analgesia phase, lasted between 220 (3 min 40 sec) and 550 sec (9 min 10 sec), with an average value of 405 sec (6 min 45 sec). The preparation of cavities ranged between 10 and 340 sec (5 min 40 sec), average value of 195 sec (3 min 15 sec).
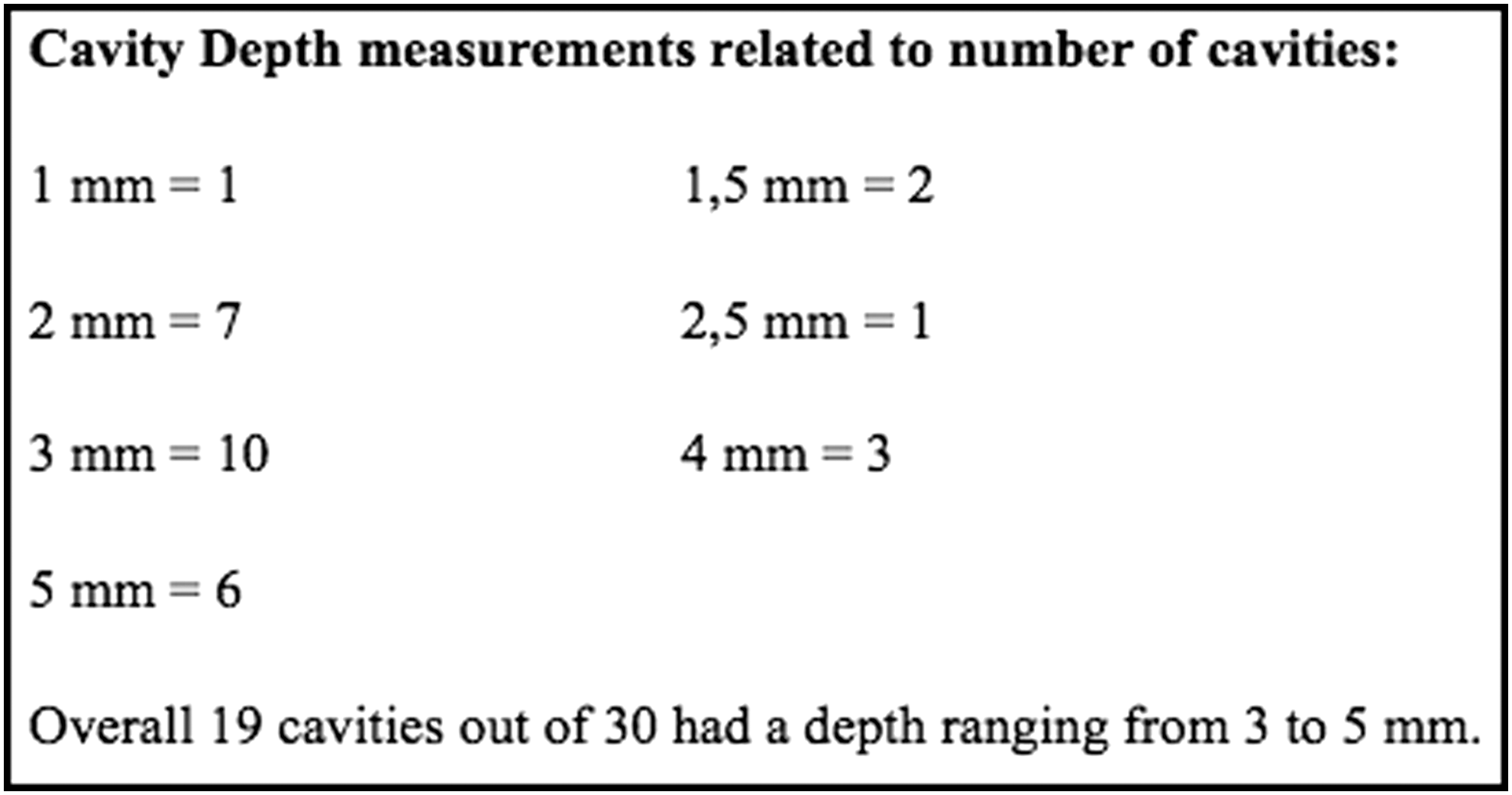
Depth measurement of the 30 cavities ranged, after ablation, from 1 to 5 mm (average 3 mm).
Depth measurements related to number of cavities were: 1 mm=1,1.5 mm=2.2 mm=7,2, 5 mm=1 3 mm=10, 4 mm=3, and 5 mm=6.
Overall, 19 cavities out of 30 had a depth ranging from 3 to 5 mm. Figure 4 shows the cavity depths.
Cavity depths.
The results regarding the level of discomfort perceived by the patients and the level of anxiety felt before the therapy has been summarized in Figs. 5 –10.
Distribution of discomfort groups in the sample of patients.
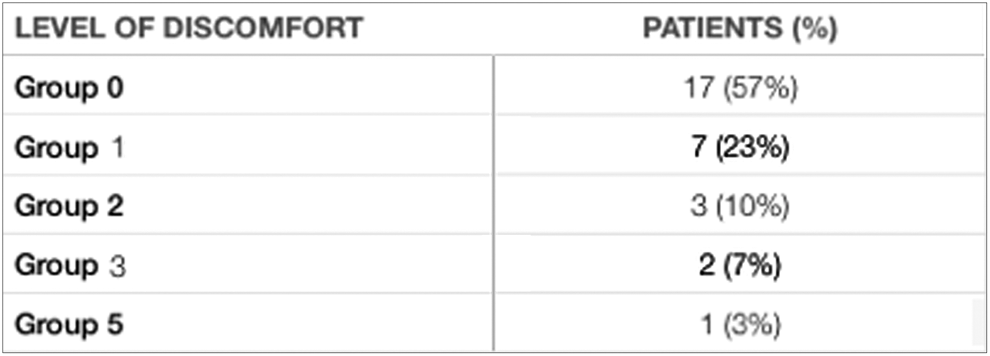
Levels of discomfort: number of patients per each group and percentage.

Levels of anxiety related to discomfort groups (mean values and range).
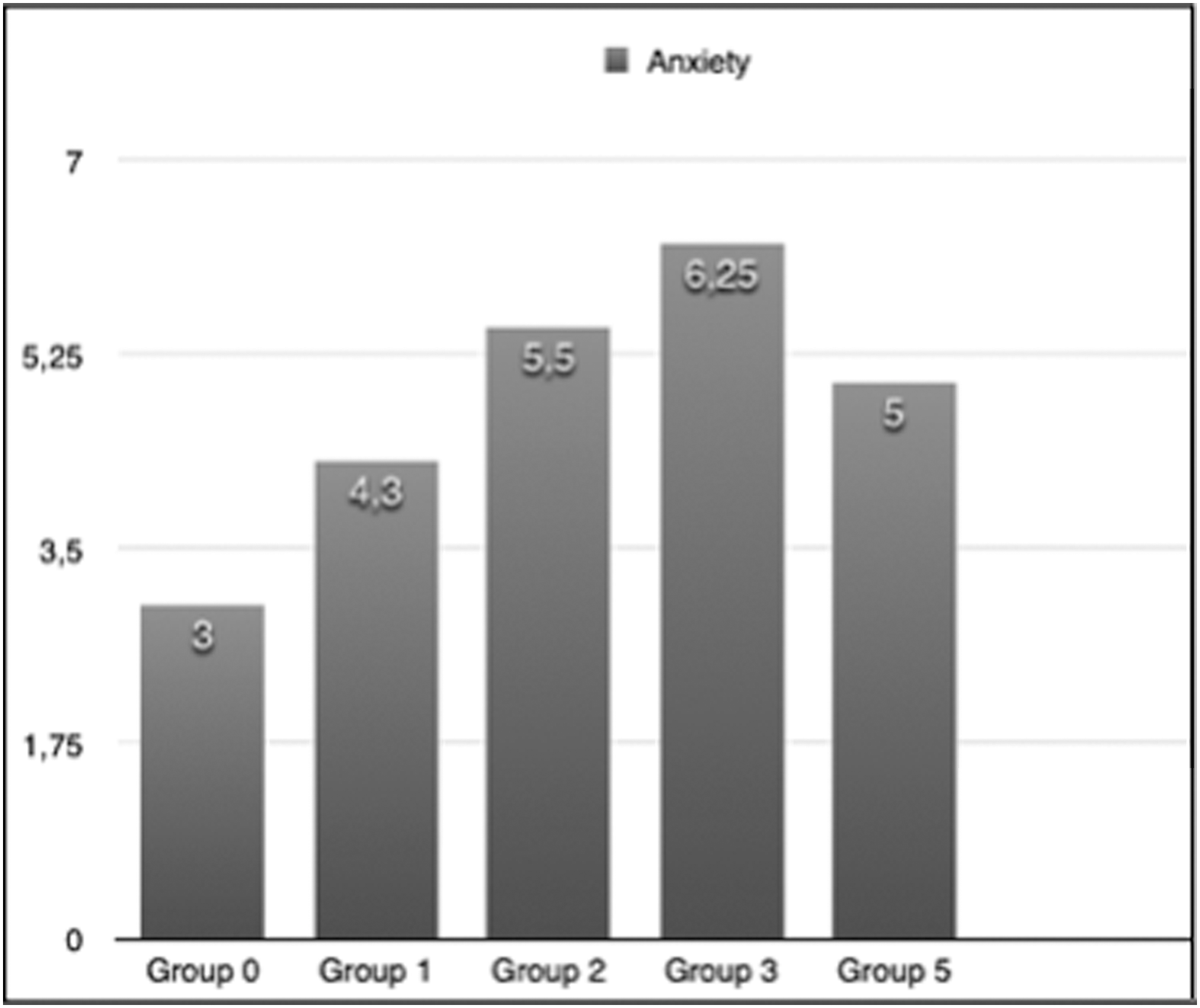
Anxiety levels per each discomfort group (mean values).
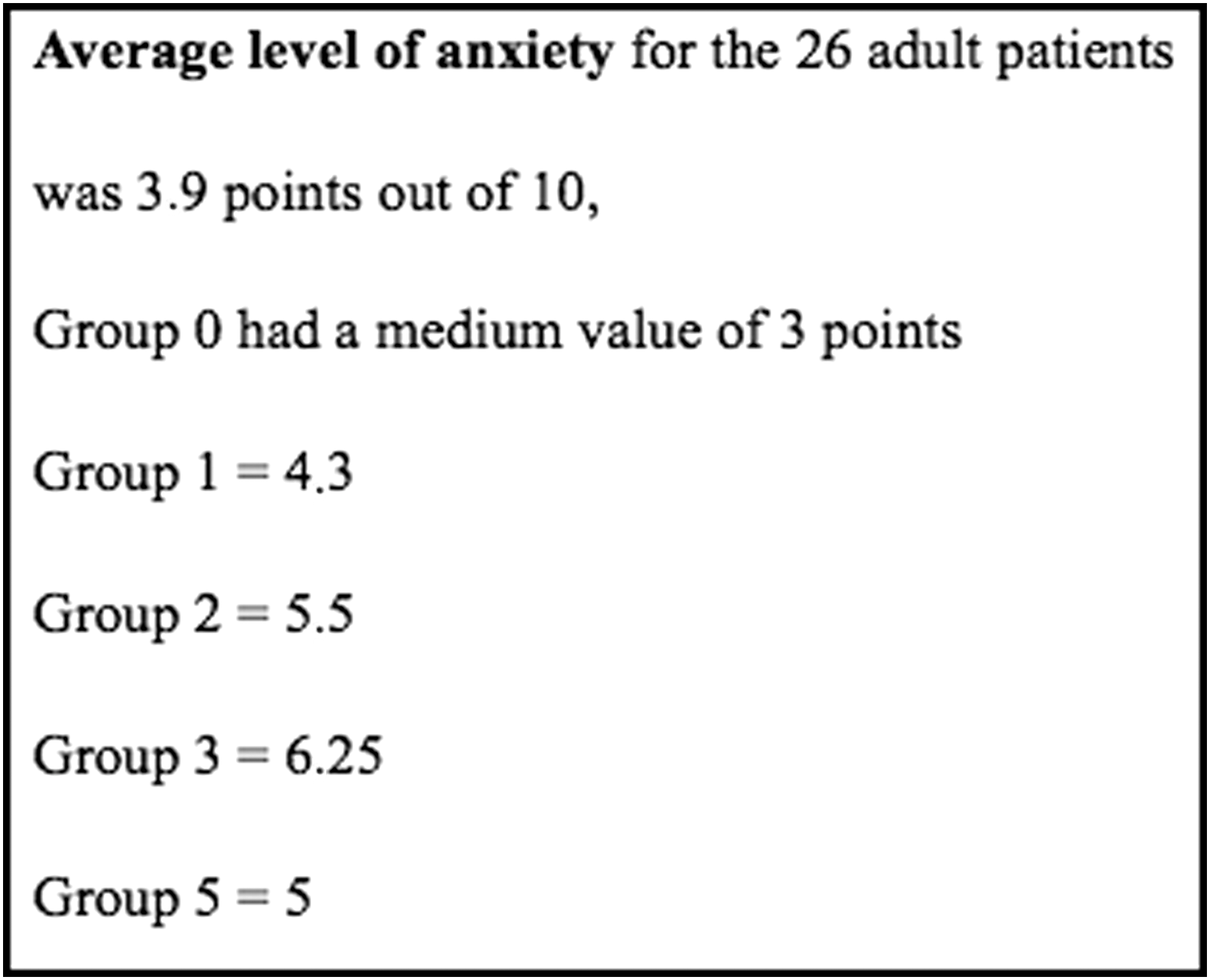
Levels of anxiety perceived by patients before the treatment.
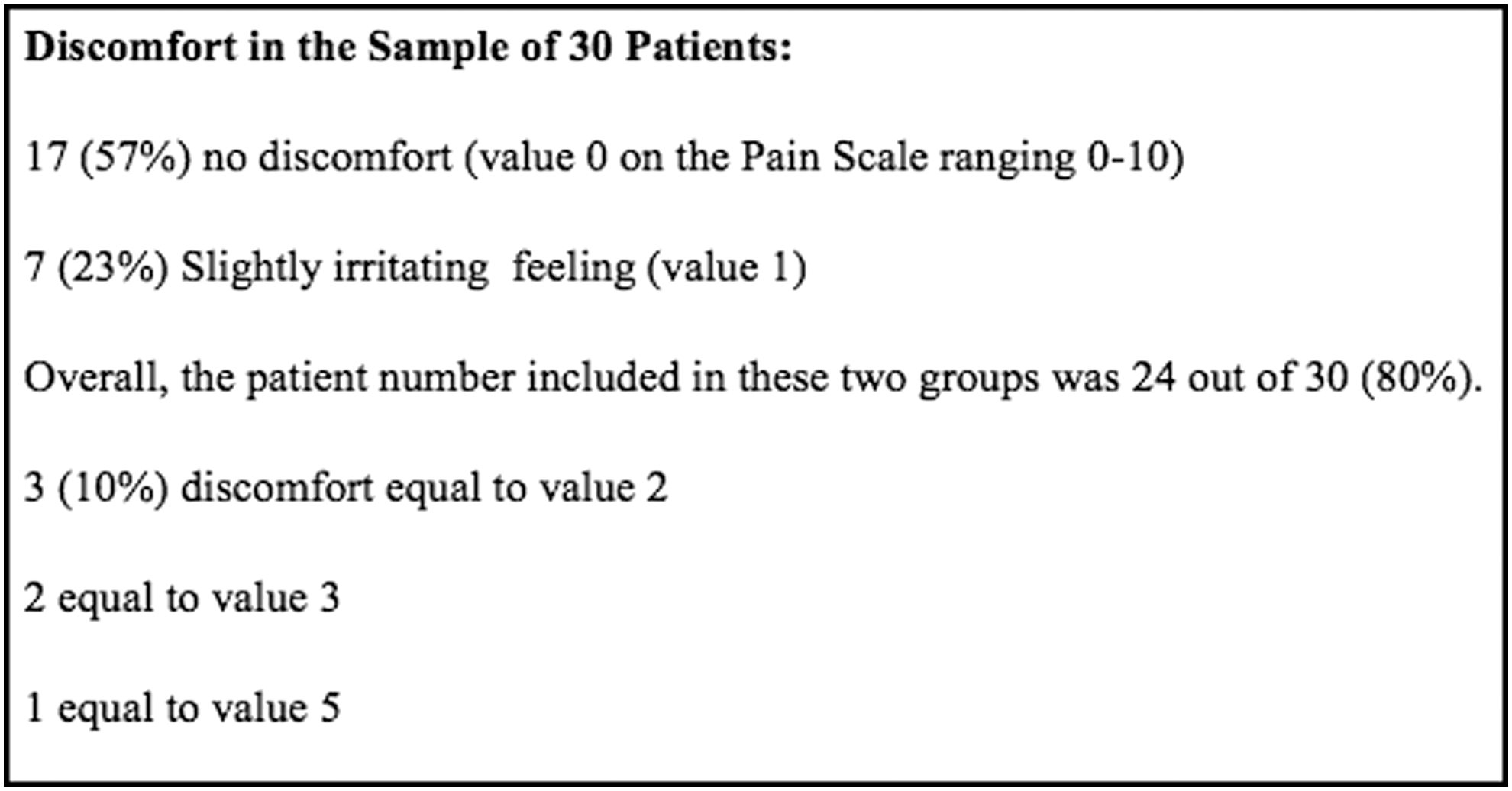
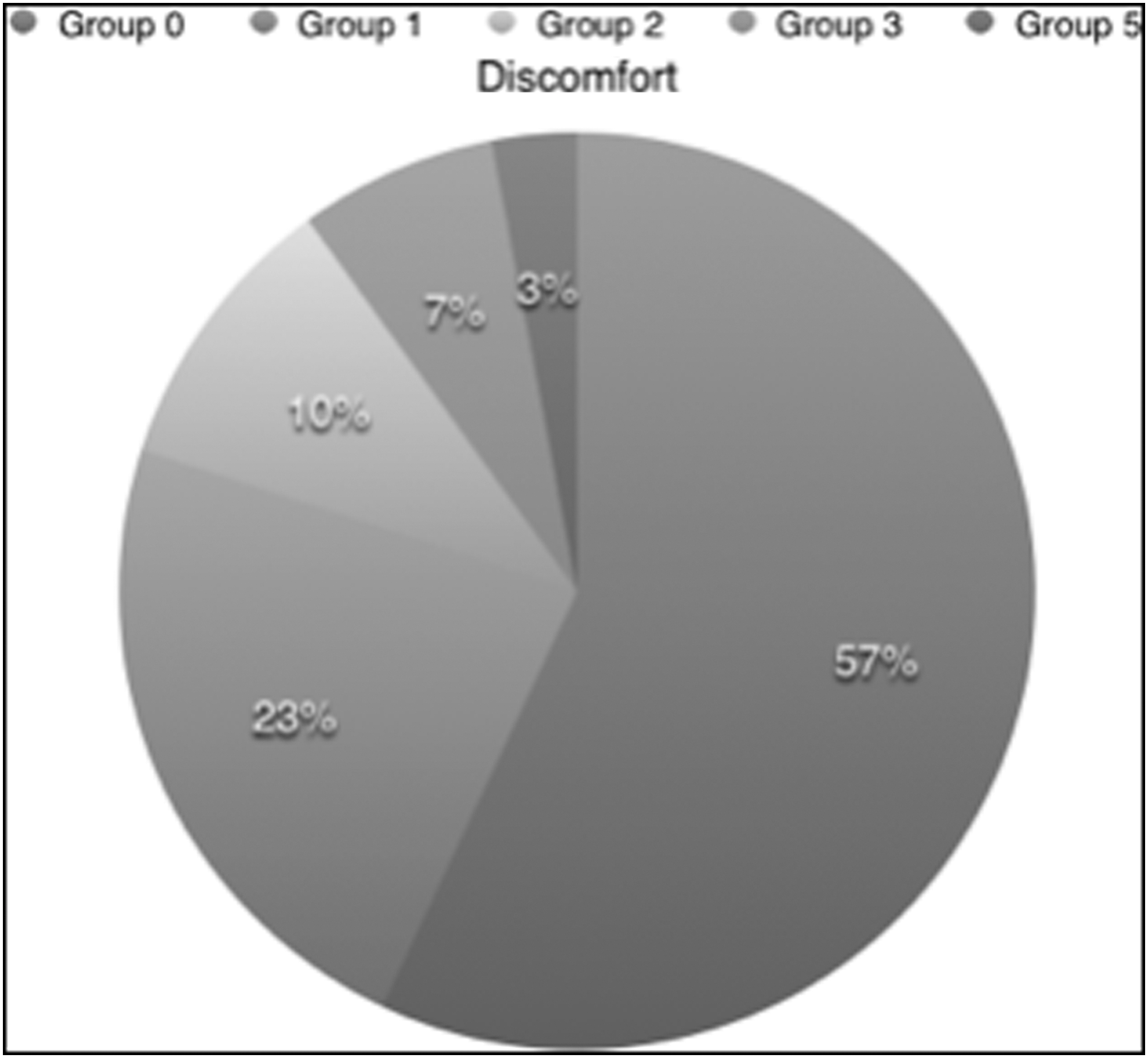
Discomfort felt during the restorative treatment.
Seventeen out of 30 (57%) patients did not feel any discomfort (value 0 on the pain scale ranging from 0 to 10).
Seven out of 30 (23%) felt a slightly irritating feeling (value 1).
The number included in those two groups was 24 out of 30 (80%).
Three patients felt an estimated discomfort equal to value 2 (10% of the total sample), two felt a discomfort equal to value 3, and only one felt a discomfort equal to value 5 (Fig. 10 shows the distribution of discomfort groups).
Even though local anesthesia was offered, none of the patients requested it.
The adults (26 subjects), considering possible levels of anxiety included in a range of 0–10, on average scored 3.9 points.
Within a range of discomfort, category 0 had on average 3 points. Those at discomfort level 1 had on average 4.3 points. Category 2 had an average value of of 5.5 points. Category 3 had 6.25 points. The patient in category 5 reached 5 points
The four pediatric patients who filled in the CFSS-DS questionnaire (and did the same again 1 week later in order to evaluate the change of anxiety level) had the following final scores: Patient A=45 points (discomfort level 0), reduced to 39 Patient B=57 points (level 1), reduced to 48 Patient C=34 points (level 1), reduced to 33 Patient D=51 points (level 0), reduced to 45
The paired t test was used to verify the statistical significance of the EPT values variation.
The statistical analysis performed indicated no significant differences among the values measured by the means of the EPT (p always>0.05).
The alternate comparison in couples, between two consecutive measurements, highlighted that there were no significant variations in the values observed in the same tooth.
In order to further evaluate the relationship among the different factors and parameters, further analysis was applied (univariate, multivariate, and ordinal logistic regressions).
Discussion
Many factors influence pain perception. 8,23
There is uncertainty as to which patients require preliminarily anesthesia, for which restorative therapies it is always advisable, and which would be the ideal therapeutic approach for every subject. 24
Different possible explanations have been suggested for low-level laser (photobiomodulation) action surrounding pain control, 25 and several wavelengths have been considered. 7 . The commonest are Neodymium-doped Yttrium Aluminium Garnet (Nd:YAG) (1064 nm), diodes (810–980 nm), and Erbium (Erbium Yttrium Aluminium Garnet [Er:YAG] 2940 nm, Er,Cr:YSGG 2780 nm).
Many studies agree that to obtain pulpal analgesia, it is necessary to take advantage of low energy and power densities. 1,8,18, 24,26
Furthermore, in those laser machines, low-level air/water spray delivery should be adopted to avoid dental sensitivity phenomena. 7,27
At present, there is no consensus regarding a complete and detailed treatment protocol with reliable laser parameter settings, 27 –33 and some research lacks necessary parameter detail such that it is almost always neither repeatable nor reproducible. 34
It has been scientifically demonstrated that permanent teeth are more sensitive to pain than deciduous teeth, and that laser analgesia is easier to obtain when dealing with the latter. 24
In this investigation, the cases in which the subjects felt a greater discomfort (categories 2–3 and 5) were completed with lower levels of energy and power and in a shorter time. Even though the parameters of the Er,Cr:YSGG laser were lower, the discomfort for these patients was greater. It was, therefore, necessary to consider additional factors in order to explain this significant difference. Factors considered and analyzed were patient gender and age, anxiety felt during the therapy, tooth position, depth of cavity, overall time for cavity preparation, and times of use of the different laser energy levels.
It was found that one of the most important factors that influenced pain perception was patient age, with all the patients who felt greater discomfort being in age groups 20–29, 30–39, and 40–49 years.
It is suggested that with younger patients, pulpal analgesia could be obtained more easily and quickly because the dental hard tissues contain more water and dentinal tubules that are wider in diameter; this could facilitate ablation and progression of laser beam effect on pulpal nociceptors.
Older patients could be less sensitive to irradiation for the opposite reason; more sclerotic and calcified dental tissues with narrow dentinal tubules, even if more difficult to ablate, can render the pulp more insulated to incident photonic energy.
Further to the responses given by the adult patients when filling in the autoevaluation questionnaire regarding the sensations felt and the anxiety perceived, it was evident that there was an increasing and directly proportional trend of both values as the discomfort felt by the subjects increased.
The average level of anxiety for the 26 adult patients was 3.9 points out of 10, but the subjects of group 0 had a mean value of 3 points; in category 1 it was 4.3, in category 2 it was 5.5, in category 3 it was 6.25, and in category 5 it was 5. (Fig. 9 shows levels of anxiety perceived by patients before the treatment.)
Therefore, for patients having higher levels of anxiety connected to dental care a trend can emerge toward feeling more discomfort during therapy.
With regard to the four pediatric patients, it is possible to underline that according to their CFSS-DS answers, three of them could be considered potentially anxious and one borderline. All four felt a very low discomfort or nothing at all (categories 0 and 1).
It is suggested that the patient groups reporting higher levels of anxiety preceding the dental appointment were the same who felt a greater discomfort during the therapy. In consequence, it is probable that the anxiety factor contributed to a higher subjective evaluation of discomfort.
The only way to obtain an evaluation of clinical analgesia adequacy may be to directly verify if the restorative treatment could be performed after laser analgesia without inducing any pain. Obviously, this exposes the operator to the risk of causing annoying or painful sensations to the patient.
It is not clear as to why it is possible to perform cavity preparation without any patient discomfort after inducing laser analgesia, even if during this procedure the EPT pulse can be easily perceived by the patient.
It can be also hypothesized that laser analgesia does not cause changes in the pulp electric state, or that its nerve fiber conductivity can be altered in a substantially different mode to that obtained with anesthetic drugs; only by clarifying the phenomenon concerning laser-induced analgesia would it be possible to understand which is the best instrument able to measure it.
It is possible that the EPT values that remained constant (or lowered) could be a sign of a higher tendency to dental discomfort or pain.
The levels in the post-ablation phase frequently remained stable or reduced. This seemed to be caused by the interruption of photonic laser irradiation. In the previous phases, 18 patients demonstrated constant or reduced sensibility EPT levels.
Among them, 14 patients were part of discomfort categories 0 and 1 (9 and 5, respectively). Only two felt a discomfort at level 2, and two felt discomfort at level 3.
It may therefore be stated that EPT readings at a lower or constant level were not a sign of absent analgesia and did not show a greater risk of potential pain for the patient.
The factors that seemed to have a higher tendency to promote the shift to greater discomfort categories were: posterior teeth, greater caries depth, higher power levels, and ablation time.
In Figs. 11 –14, a clinical case example of the technique applied in this study is shown. It is our opinion that the depth of the carious cavity is an important factor that influences sensibility, but the time taken in cavity preparation is a greater determinant.

Carious cavity in tooth #2 I class.

With the spacer in position, the analgesia phase is achieved.

Ablation of carious tissue.
Composite filling.
This may be caused by the effect of the Er,Cr:YSGG laser on dentin; the more extensive the laser use, the more the tubules will be opened and the greater the perception of discomfort. Additionally, if the dental hard tissues are not easily ablated (for example. if composed of a lower water percentage) and it is necessary to extend use of the laser for more time or to increase the energy levels, then the risk of pain further increases.
One more element to consider is the fact that laser analgesia is not completely effective in obtaining periodontal tissue analgesia.
During this research, it was frequently noticed that even if the tooth was completely insensitive to carious ablation, the patient could feel the discomfort provoked by the positioning of rubber dam clamp, matrix band, or wedge.
The use of EPT was the factor causing greater disturbance, because the patient always felt the impulse of the electric current even if no pain was otherwise perceived during the ablation.
Conclusions
With this research, a protocol is proposed for painless restorative therapy using the Er,Cr:YSGG laser. The efficacy was proven in a consistent number of cases (80%).
In relevant literature, the comparison between the traditional handpiece with bur and Erbium showed that with the former, painless treatment was obtained in only 20–50 % of the patients.
In using this laser, it was possible to avoid local anesthesia with a needle and the use of bur. Therefore, anxiety was reduced when associated with restorative treatment.
Footnotes
Author Disclosure Statement
No competing financial interests exist.