
Abstract
Introduction
M
Until ∼10 years ago, laser therapy was commonly associated with postoperative complications, including bruising, decreased hematocrit resulting from significant blood loss, mild burns, changes in skin texture, and skin waviness. 1 –3 These were challenges to plastic surgeons and served as a stimulus for the development of devices that allowed partial or even total correction of skin deformities. At present, the 975 nm diode laser may be used in the photothermal treatment of skin laxity.
The photothermal effect of laser irradiation on the hypodermis causes retraction of superficial and deep skin layers by the heating of fibrous septa. 4 –6 It also results in the thinning of the reticular dermis, leading to improved aesthetic results 1 and decreased bleeding at the treatment site. 7,8 The use of laser may also reduce or eliminate bruising in the immediate post-treatment period by the cauterization of small vessels. 8 –10 These effects have served as motivation for the development of laser devices operating at different wavelengths in the range of the absorption spectra of fat, water, and other chromophore association for the treatment of skin laxity. 11 –14
The dual-wavelength diode laser is among the devices available for this purpose. It operates at 975 nm, which is a wavelength that acts on collagen and elastin fibers in the deep dermis. This system preserves the epidermis, therefore eliminating most risks associated with its use. 4
The use of laser devices for the photothermal treatment of skin laxity requires attention during the procedure regarding the total energy transmitted by the laser to each region of the body (cumulative energy) to achieve the best aesthetic result by the remodeling of fibrous conjunctive tissue. 6 The control of the cumulative energy is essential to reduce risk of complications, such as necrosis, prolonged erythema, hyperchromic skin patches, secondary bacterial infection, and dyschromia. 2 This topic has been studied to determine the safety parameters to prevent treatment complications, especially at the 975 nm wavelength. 9,15
The purpose of this study was to evaluate skin tightening of the face and neck using a 975 nm diode laser.
Materials and Methods
This retrospective, cross-sectional study included the medical records of 17 patients who had undergone photothermal laser therapy to correct skin laxity in the cervicofacial region at the Plastic Surgery Outpatient Clinic of the Federal University of Pernambuco (UFPE), in Recife, Brazil, between June 2013 and February 2015. The study was approved by the Research Ethics Committee of the Federal University of São Paulo (UNIFESP approval number 436.441) and performed in accordance with the Brazilian Ethical Review System on research involving human beings. Patient anonymity was maintained.
Inclusion criteria were skin laxity in the mid and lower face and submental and anterior cervical areas, being 40–65 years of age, and body mass index (BMI) within normal range (18.5–24.9 kg/m2). Patients could be of either gender.
Exclusion criteria were laxity after bariatric surgery, pregnancy, diagnosis of autoimmune diseases or cancer, infection in general, allergies, collagen disease, and use of isotretinoin in the past 12 months.
Power and sample size calculations estimated a purposeful convenience sample of 20 patients, assuming that 1200 patients are seen per month (which is the monthly number of outpatient visits in the study setting), with 80% power at 5% significance level. Therefore, the medical records of 20 patients who had undergone photothermal therapy with a 975 nm diode laser were retrieved; however, three of the patients were lost to the 3-month follow-up, and their records were excluded from the sample. The three patients did not come to the 3-month follow-up either because they were satisfied with the results or because they lived in cities far from the clinic.
Photothermal laser therapy
Four cervicofacial lines (L1, L2, L3, and L4) were defined at both sides of the face. Line L1 was located at the mid-third of the face and extended from the corner of the mouth (cheilion) to the lateral palpebral commissure (exocanthion) of the same side of the face; line L2 was positioned at the lower third of the face and constructed from the central part of the chin region (mental protuberance) to the inferior insertion of the earlobe (otobasion inferius); line L3 was placed in the anterior cervical region and connected the hyoid bone to the mental protuberance; and line L4 was located in the lateral cervical region and drawn from the hyoid bone to the otobasion inferius (Fig. 1).
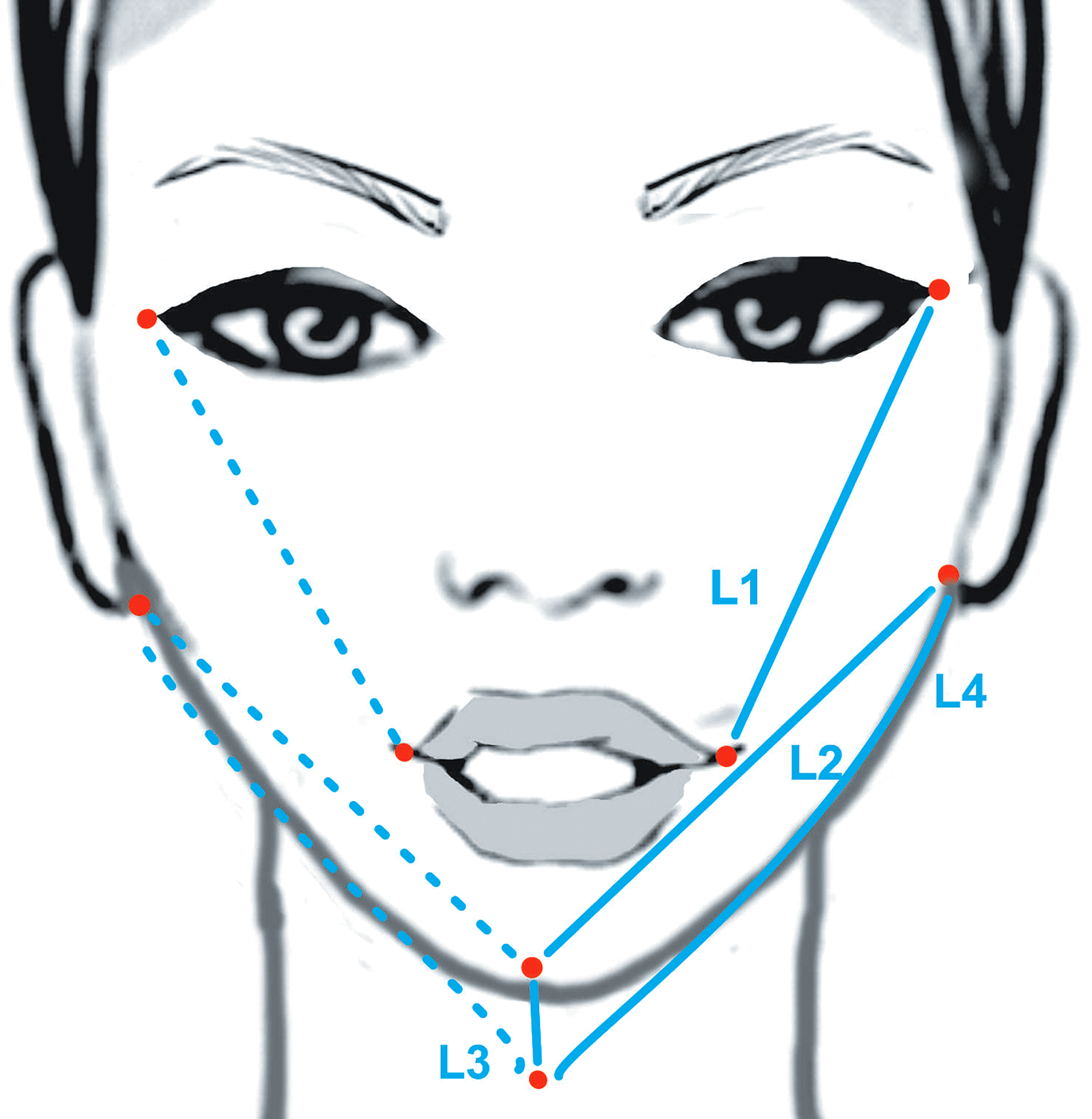
Diagram showing the position of the lines used in measurements of the face and neck performed before treatment, immediately post-treatment and 3 months later. Line L1 extended from the cheilion to the exocanthion of the same side of the face; line L2 was constructed from the mental protuberance to the otobasion inferius; line L3 connected the hyoid bone to the mental protuberance; and line L4 was drawn from the hyoid bone to the otobasion inferius.
Three measurements of every line segment from each side of the face were carefully made at the three time points (before the photothermal laser therapy, immediately after the procedure, and 3 months post-treatment) using a caliper, and the average of the three measurements was then calculated. The measurements were recorded in a standardized form prepared for this purpose, which was attached to the medical records. The length of the line segments presented in this article represents the average of line measurements from the right and left sides of the face at the three time points. Only the length of line L3, which is common to both sides of the face, was not calculated as the average of the two sides.
Photodocumentation with standardized views was performed for all patients at the same distance, with the same camera (Sony Lens/Optical zoom 3X, 5.0 megapixels, Sony Cyber-shot DSC-P10, Sony Corporation, NY), at the three time points. In order to avoid distortions in the line measurements, the photographs were taken at the same angles with the patient staying still in the sitting position. The head and neck of the patient needed to be motionless; facing forward; without flexion, extension, or rotation, and the patient could not be smiling or swallowing at the time the photograph was taken (Fig. 2).
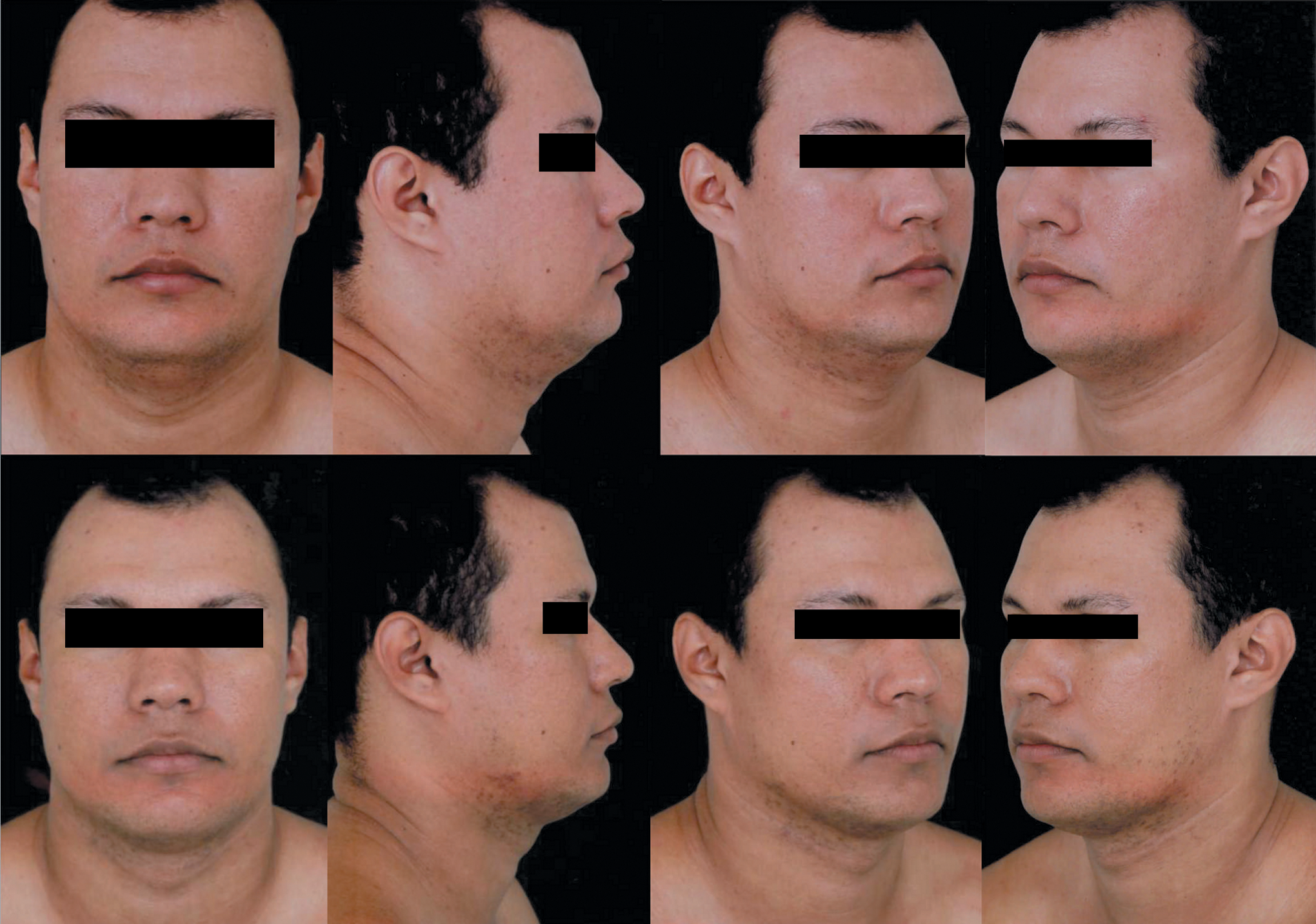
Anterior, lateral, and oblique views taken before the photothermal laser therapy (top) and 3 months after the treatment (bottom), showing the cervicofacial region of a 49-year-old patient treated with a 975 nm diode laser. The patient gave permission to use these photographs.
The treatment was performed in one session using a pulsed diode laser [SlimLipo, Palomar Medical Technologies, Burlington, MA; licensed by the United States Food and Drug Administration (FDA) and by the Brazilian Health Surveillance Agency (ANVISA)] operating at 975 nm, with a frequency of 100 Hz and a pulse duration of 100 μs, and independently controlled for different output powers (3–8 W). The plastic surgeon could apply the laser in the different treatment areas for different periods of time, as necessary, while always respecting the safety parameters.
The photothermal effect of laser irradiation on the hypodermis is used for heating fat cells, leading to membrane rupture with consequent release of intracellular lipase and fat liquefaction, which facilitates liposuction (Fig. 3). In addition, the heating of fibrous septa and reticular dermis causes tissue thinning, leading to an improved aesthetic result. 1 The photothermal properties of the laser light may also be applied for cauterizing small blood vessels, decreasing bleeding at the surgical site. 6
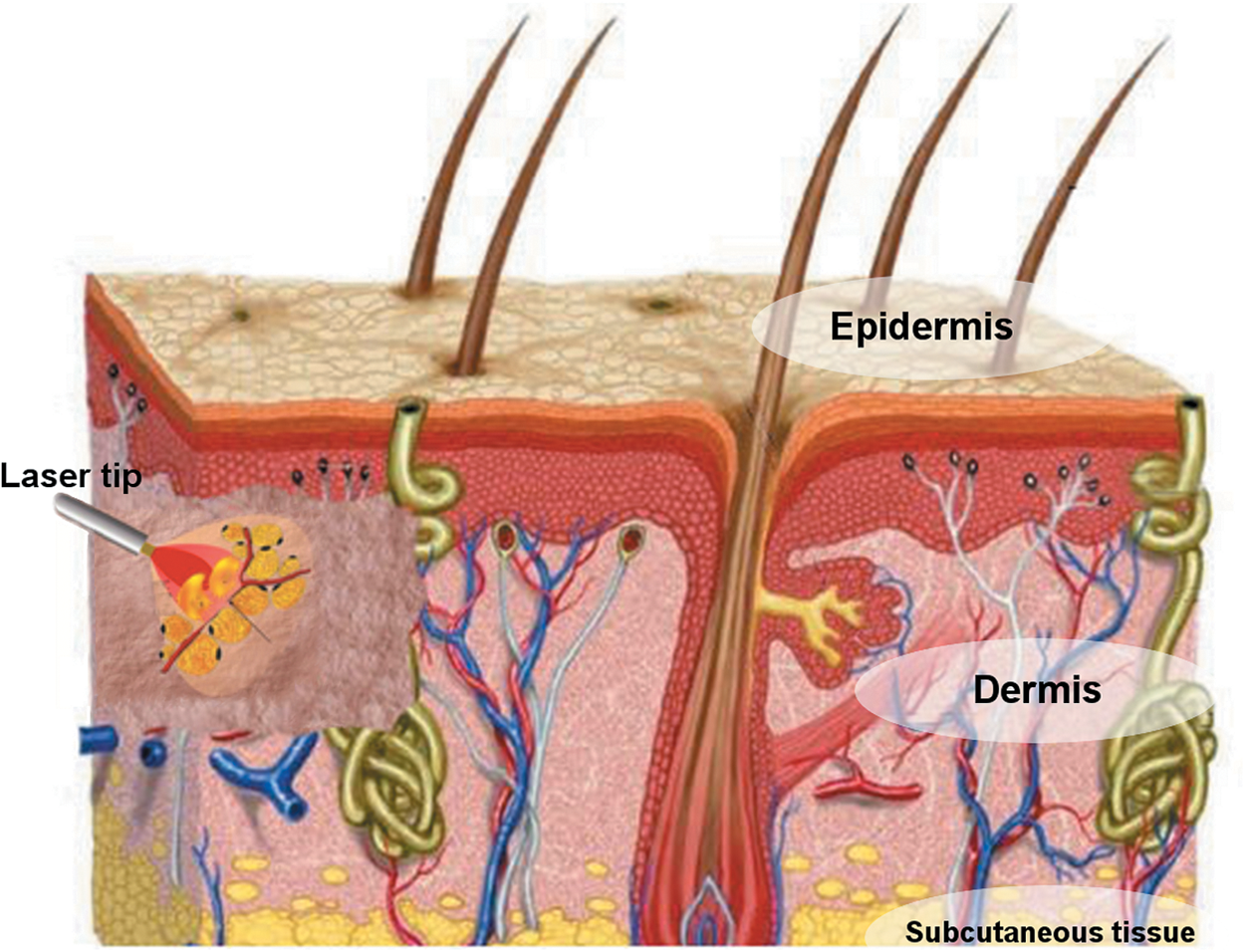
Diagram showing the interaction of the laser irradiation with the dermal tissue.
The laser power detection system is calibrated regularly, according to the manufacturer's specification, by a specialized service center. Displayed power is checked against a power meter. If necessary, recalibration is performed to bring the system to within specification.
After antisepsis with chlorhexidine, areas of 10 and 50 cm2, for a total area of 60 cm2, were marked on the skin on each side of the face with a bright marker (Fig. 4). The procedure was performed in a surgical setting, with the patient under sedation, with intravenous midazolam (15 mg/3 mL; Dormonid; Produtos Roche Químicos e Farmacêuticos SA, Rio de Janeiro, Brazil). Once the patient was sedated, each side of the face was infiltrated with 100 mL of local anesthesia, containing 90 mL of 0.9% saline and 10 mL of 1% xylocaine, at 4°C, always in the presence of an anesthesiologist.

Pretreatment photograph showing the face of a 60-year-old patient marked with areas of 10 cm2 (cumulative energy, 0.3 kJ) and 50 cm2 (cumulative energy, 1.5 kJ) for laser application. The patient gave permission to use this photograph.
First, an 18-G hypodermic needle (1.20 × 40 mm) was used to puncture the skin. The laser tip was inserted through the skin needle puncture at an angle of 15 degrees to the surface of the skin, 5–10 mm into the subcutaneous tissue (depending upon the specific patient), without a skin incision, and leaving no marks. The insertion points (marked in red in Fig. 5) were located at the right and left lateral palpebral commissures (exocanthion), right and left insertions of the earlobes (otobasion inferious), and mental protuberance for the treatment of area A, areas B and D, and area C, respectively. A 1.5 mm diameter cannula and two laser tips with different lengths (80 and 180 mm) were used, allowing treatment of small areas of the face and medium areas of the neck, using the laser on the Aspire platform, which operates with output power up to 24 W. For each of the four cervicofacial regions, the optimal cumulative energy to promote skin tightening was estimated based on the number of 100 cm2 skin areas within the treatment site. A maximum energy dose of 3 kJ (3000 J) per 100 cm2 of skin area and maximum output power of 8 W were used on as safety parameters. To prevent burning injuries, the temperatures of the skin and subcutaneous tissue should never exceed 32°C. 16 –19 Skin and subcutaneous temperatures were measured with an infrared thermometer (Extech Instruments Corp., Waltham, MA). The four regions for laser application are represented by shaded areas (A–D) in Fig. 4. The cumulative energy values for these areas are as follows: area A (10 cm2) = 0.3 kJ; area B = 0.4 kJ at an output power of 2 W; area C = 0.6 kJ; and area D = 0.5 kJ; or areas B+C+D (50 cm2) = 1.5 kJ.
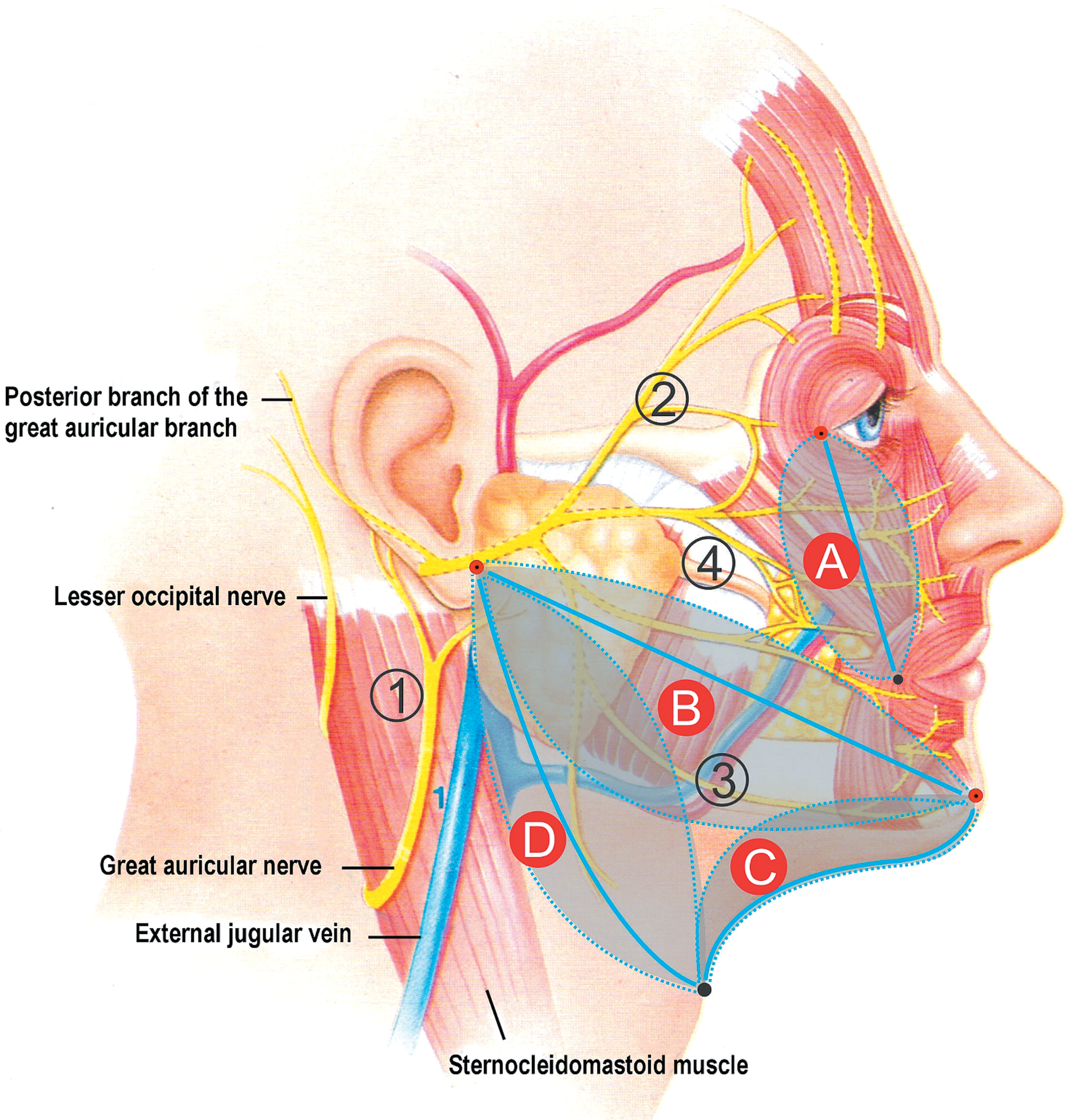
The shaded areas A–D correspond to the four regions for laser application. Numbers show the regions at risk of injury to the (1) auricular, (2) temporal, (3) marginal mandibular and (4) zygomatic branches of the facial nerve. The red dots mark the insertion points for the cannula and laser tips.
There are four regions at risk of injury to the branches of the facial nerve (Fig. 5). 20 The laser tip should not be used near the auricular, temporal, or zygomatic branches of the facial nerve. Close to the marginal mandibular branch (treatment area B, region of risk 3), a cumulative energy of 1 kJ per 100 cm2, output power of 2 W, and skin and subcutaneous temperatures of 31°C should not be exceeded.
Laser exposure time varied according to the treatment area and cumulative energy. The greater the cumulative energy required, the longer the exposure of the treatment area to laser irradiation, always respecting the safety parameters.
Immediately after the procedure and at the 3 month follow-up, the patients were evaluated for possible complications, such as bruising, prolonged erythema, bleeding, and necrosis, and the information was recorded.
Statistical analysis
Statistical analysis was conducted using the Statistical Package for the Social Sciences (SPSS) version 20.0 (SPSS Inc., Chicago, IL). Descriptive analysis was conducted to determine means, standard deviations, and confidence intervals (CI). Non-normally distributed values were expressed as medians and the semi-interquartile range was corrected by Tukey's method. Paired Student's t test and the Wilcoxon test were performed for comparisons of skin tightening of predefined areas among the three time points. All statistical tests were performed at a significance level of 0.05 (p < 0.05).
Results
Seventeen patients [16 (94.1%) women and 1 (5.9%) man] were treated with photothermal laser therapy. The diode laser operating at 924 and 975 nm was used in only one patient; the other 16 patients were treated with the laser operating at 975 nm. The mean age of the participants was 47.6 ± 1.3 years (range, 40–63 years; 95% CI, 47.6–52.8 years).
Parameters, such as cumulative energy, output power, and sequence of wavelengths used during the photothermal laser therapy in the different regions of the face and neck are listed in Table 1.
Measurements of the cervicofacial lines defined on the treated areas taken before the procedure, immediately after the procedure, and 3 months post-treatment are given in Table 2. There was a progressive tightening of the skin over time at all treatment sites.
SEM, standard error of the mean; SIQR, semi-interquartile range (Tukey's method); IAT, immediately after treatment; 3-month f/u, 3-month follow-up.
Comparisons among measurements taken at baseline, immediately after the procedure, and 3 months after treatment are depicted in Table 3. There were significant differences in length of the cervicofacial lines from baseline to both the immediate and 3-month post-treatment assessments; however, no significant difference was found between the immediate and 3-month post-treatment results (Table 3).
Numbers in bold indicate statistical significance, paired Student's t test (p < 0.05).
SEM, standard error of the mean; IAT, immediately after treatment; 3-month f/u, 3-month follow-up.
Relative changes in the length of the four cervicofacial lines between time points are shown in Table 4. There was a significant reduction in the length of the four cervicofacial lines in most patients in the immediate post-treatment assessment. The tightening of the skin was maintained in most patients from the immediate post-treatment period to the 3-month follow-up; however, some patients experienced some increase in the length of the cervicofacial lines, especially in the mid (n = 5; 29.4%) and lower thirds (n = 4; 23.5%) of the face, but with no significant difference between the two time points.
Numbers in bold indicate statistical significance, Wilcoxon test (p < 0.05).
IAT, immediately after treatment; 3-month f/u, 3-month follow-up.
The skin and subcutaneous temperatures did not exceed 32°C during any of the procedures. Temperatures of the skin and subcutaneous tissue before and after infiltration with saline combined with xylocaine at 4°C and after laser application are shown in Table 5. No cases of bruising, secondary anemia caused by bleeding during the treatment procedure, or tissue necrosis occurred; two patients had prolonged edema and erythema for up to 6 months.
Infiltration of 0.9% saline and 1% xylocaine at 4°C.
Photographic examples of the results obtained with photothermal laser treatment of face and neck deformities are shown in Figs. 6 and 7.

Anterior views taken before treatment (left) and 3 months post-treatment (right) showing improvement in the anterior cervical region of a 63-year-old patient. The patient gave permission to use these photographs.

Photographs in anterior views taken before treatment (left) and 3 months post-treatment (right) showing improvement in the cervical region of a 58-year-old patient. The patient gave permission to use these photographs.
Discussion
Skin laxity is one of the most common complaints of patients who seek cosmetic treatments. Cosmetic surgery offers a variety of treatments for reduction of deformities associated with skin laxity. Among the several invasive and noninvasive techniques, we may cite facelift, acid-based treatments, and photothermal laser therapy.
Ten years ago, laser irradiation was proposed as an alternative for the treatment of skin laxity and fat accumulation on the face and neck 15,21,22 and, recently, studies on laser therapy and liposuction have been published based on evidence. 17 Today, new minimally invasive or noninvasive techniques are available to treat skin laxity and aesthetic contour deformities. 18 In 2006, a project was developed at Harvard University, resulting in a method to simultaneously treat adiposity and skin laxity using a dual-wavelength diode laser operating at 924 and 975 nm; however, the 975 nm wavelength was used alone in areas with skin laxity but without adiposity. 22 The diode laser operating at 924 and 975 nm was used in only 1 of the 17 patients participating in this study; the other 16 patients were treated with the laser operating at 975 nm. In a previous study, 41 patients treated with a dual-wavelength diode laser had a marked reduction of skin laxity. 19 Photothermal laser therapy has shown to be an effective, safe, and reproducible procedure if safety parameters (i.e., cumulative energy of 3 kJ per 100 cm2 for the face or up to 5 kJ for other parts of the body, and skin and subcutaneous temperatures ≤32°C) are followed. 19
This article focuses on the treatment of the sagging face, and is based on our extensive experience in the use of photothermal laser therapy to reduce skin laxity in different areas of the body. In this study, a 975 nm diode laser was used in the photothermal treatment of skin laxity of the face and neck based on reported skin-tightening effects. 22 Skin tightening was observed in the four treated cervicofacial regions immediately after the procedure, and the results were maintained over the 3-month follow-up.
This is a mildly aggressive procedure with minimal complications; no cases of bruising, secondary anemia caused by bleeding during the treatment procedure, or tissue necrosis occurred. Two patients had prolonged edema and erythema for up to 6 months, which have also been reported by other authors. 1 –3,21
The diode laser used in the present study differs from other systems in that it operates at 975 nm, which is a wavelength that especially acts in the photothermal treatment of skin laxity. This system also allows the simultaneous use of two wavelengths (blend system), which stimulates tissue contraction, reducing both skin laxity and adiposity, thus facilitating skin contouring without excision or bruising. 7,15,22 Moreover, the device provides control of the output power from low power to a maximum of 24 W. This feature has a direct impact on the aesthetic outcome, because the laser power delivered to the tissue is associated with the cumulative energy and temperature rise at the treatment site. Mordon et al. 6 developed a mathematical model to explain the relationship among output power, temperature, and cumulative energy, and emphasized the need to determine the optimal cumulative energy as a function of the volume of tissue to be treated by laser.
The laser power and cumulative energy per treated area used in this study were determined based on experiments conducted by the authors, whose results were presented at the I Advanced Fractional and Body Sculpting Symposium in New York, NY, in 2009. 10 According to our experience, a maximum cumulative energy of 3 kJ per 100 cm2 skin area of the face should be used for obtaining the best aesthetic outcome tailored to the patient. 9
The use of the optimal cumulative energy results in a moderate rise of temperature in the skin, which leads to connective tissue remodeling and cauterization of small blood vessels. 6 The present study showed that a cumulative energy of 3 kJ per 100 cm2 skin area may be considered as an optimal energy because it led to a progressive tightening of the skin over time, without causing bruising, prolonged erythema, excessive bleeding, or skin necrosis. The laser treatment resulted in a progressive tightening of the skin over time, as indicated by significant differences in the measurements of the neck and mid and lower thirds of the face from baseline to the immediate post-treatment assessment, which persisted after 3 months of the procedure. This suggests that photothermal laser therapy resulted in tissue remodeling, according to the physiology of each patient.
Photothermal laser therapy was performed with a 1.5 mm diameter cannula and an 80 mm long laser tip. In most cases, the insertion of the laser tip allowed a more comprehensive dermal treatment, contributing to reduced temperature rises in the epidermis and preventing a superficial inflammatory process and formation of skin dimples. 3
The use of this laser system has several advantages for both the patient and surgeons (including reduction of operating time), which have also been reported by Parlette and Kaminer. 1
The procedure is performed with the patient under local anesthesia without the need for general anesthesia in the majority of cases, leading to a rapid recovery (∼24–48 h), with preservation of the epidermis, and without post-treatment complications that are usually associated with other techniques. The obtained results may be attributed to both the treatment procedure used in this study and characteristics of the laser system.
Photothermal laser therapy with a 975 nm diode laser has a short learning curve for plastic surgeons already experienced in other laser systems. It is a cosmetic procedure that is gaining worldwide acceptance and that has the potential to radically change the paradigm of the treatment of skin laxity. The widespread dissemination of the results obtained with this procedure is essential to demonstrate its efficacy and safety, when safety parameters are observed.
The design is a limitation of this study. Further studies using a control group receiving sham laser therapy are necessary to compare the obtained results. Studies with a split-face design are also needed to document changes measurable immediately after the procedure.
Conclusions
In 94% of cases, photothermal therapy with a 975 nm diode laser efficiently reduced cervicofacial laxity by promoting satisfactory skin tightening, without need for hospitalization. The diode laser operating at 924 and 975 nm was used in one case (6%) in the treatment of adiposity and skin laxity, and also produced satisfactory results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.