
Abstract
Introduction
T
Laser techniques have been used for many years in the gynecological setting for the treatment of cervical, vaginal, and vulval intraepithelial neoplasias (CIN, VAIN, VIN) and also for the treatment of condylomas. 2 –6 The most commonly used laser to date is the CO2 laser, which vaporizes the pathological changes. The reason for choosing the CO2 laser is the good controllability of the penetration depth. The thulium laser Vela (StarmedTec, Starnberg), with its wavelength of 1.9 μm, has a performance range of 5–50 W, and beam transmission is via a fiber system. Its depth of penetration is also controllable as a result of its good absorption in water, and it therefore offers a possible alternative to the CO2 laser. It can be used not only for vaporization and deep destruction, but also as a laser scalpel. 7,8
The aim of the present study was to investigate the safety, the feasibility, and the possibilities of the thulium laser, Vela, for vaporization in specific clinical conditions in gynecology.
Methods
After patients presented to the Dysplasia Clinic at the Tuebingen University Hospital for Women, the indication was made for laser treatment of the cervical portio, vagina, and/or vulva.
Before inclusion, the following examinations were performed: • Detailed history and physical examination • Colposcopy of portio, vagina, and vulva • Cytological smear of the portio or the vaginal stump and the vulva, if applicable, and possible sample removal to confirm dysplasia
Patients between 18 and 100 years of age who had a clear indication for laser treatment of the portio, vagina, and/or vulva were included in the study.
Indications for laser treatment were: • CIN I-II, • VAIN I-III, • VIN I-II • Cervical ectopy • Cervical, vaginal, and/or vulval condylomas
The following conditions were excluded from the study: • Contraindications for laser vaporization: conformed CIN III or VIN III; endocervical CIN I, II • Evidence of invasive disease • Lack of patient compliance to be expected • Pregnancy • Patient unable to give consent
The interdisciplinary S2k guidline for prevention, diagnosis, and therapy of human papilloma virus (HPV) infection and preinvasive lesions of the lower genital tract, and the recommendation of the German working group of cervical pathology and colposcopy (Arbeitsgemeinschaft Zervixpathologie und Kolposkopie e.V.) states that for therapy of high grade lesions of the cervix (CIN III) and the the vulva (VIN III) and endocervical CIN I and II, it is necessary to choose an excisional procedure for histological reworking of the tissue. 9,10 The standard excisional procedure in our Dysplasia Clinic is done by loop electrosurgical excisional procedure (LEEP), and not by laser conization. Therefore, all patients needing an excisional procedure were excluded from the study.
After providing written informed consent, the patients were treated using the thulium laser, Vela. The treatment was mostly performed using general anesthesia, rarely using local anesthesia. The laser power chosen was between 6 and 21 W–a mean power of 18 W (range, 11–21 W) was chosen for laser treatment of the portio; however, a mean of 8 W (range, 6–15 W) was chosen for laser treatment of the vulva. The laser power was chosen according to the best visual vaporization result. Laser use was always contactless. A LightTrail Bare Fibre (low-OH all-silica fiber) with a core diameter of 365 μm was used for treatment. The laser was used in continuous wave (CW) mode. Several treatments with the thulium laser were planned for very extensive cases. Analgesia was given after treatment (Voltaren® 100 mg suppository) and silver sulfadiazine cream (Flammazine Cream®) was applied to the vaporized area. Any relapses were treated with the CO2 laser. Follow-up examination usually took place after 1–2 weeks, 3 months, and 6 months in the dysplasia clinic, where colposcopy and, when necessary, a cytological smear, were performed. A biopsy was also performed if the colposcopy result was suspicious.
Any possible side effects that occurred, as well as the response to treatment, were recorded.
The response was assessed as follows.
1. Complete remission: lesion can no longer be optically/cytologically detected (for dysplasia). Histological screening was performed for uncertain findings.
2. Improvement: regression of the lesion size/condyloma infection by ≥50% or downstaging of the dysplasia (CIN II → I; VIN II → I; VAIN III→II/I; cytologically and/or histologically) disputable
3. Persistence: regression of the lesion size/condyloma infection by <50%
4. Relapse: after remission/improvement there was recurrence/enlargement of the finding.
The patients also completed a questionnaire about pain and side effects during and after the treatment.
Results
During the period from January 2012 through January 2014, 18 patients were treated using the thulium laser, Vela. Three patients had a CIN I, 12 had condylomas, two had CIN I and condylomas, and one had CIN II and condylomas. In two patients with extensive condylomas, two treatment sessions were performed. The mean age of the patients was 29.5 years (range, 19–47 years). The mean duration of treatment with the thulium laser was 15 min (range, 5–40 min).
All patients attended the colposcopy clinic 1–2 weeks postoperatively for follow-up. The wound was found to be healing in 72% (n = 13), the wound had healed in 17% (n = 3), and wound healing was delayed in 11% (n = 2). A total of 89% (n = 16) of the patients were in complete remission, 1 patient (5.5%) showed improvement, and 1 patient (5.5%) showed disease persistence.
Sixteen patients attended the second follow-up appointment 3 months postoperatively. Condylomas were still present in two patients after the first follow-up appointment. They underwent planned repeat laser treatment at the second session. Two patients, who were previously in remission, did not attend the second appointment. The wound was found to have healed in 87.5% (n = 14) and was found to be still healing in 12.5% (n = 2). Further, 62.5% (n = 10) of the patients were in complete remission, 6.25% (n = 1) showed improvement, and relapse of condylomas had occurred in 31.5% (n = 5).
The third follow-up appointment after 6 months was attended by 13 patients. The wounds were found to have healed in all patients (100%): 69% (n = 9) of the patients were in complete remission and 15% (n = 2) showed improvement. Relapse of condylomas occurred in 15% (n = 2). From these 13 patients, 3 who were found to have a relapse after the second follow-up were treated with the CO2 laser. One of these had a new relapse, the other was in complete remission, and one showed improvement.
During the 6 months of follow-up, 6 patients had a relapse of condylomas after treatment with the thulium laser; a total of 15 patients with condylomas were treated with the laser. In this study, the relapse rate of condylomas treated with the thulium laser was 40% (n = 6) during the 6-month follow-up. No relapse of CIN I, II occurred.
Figure 1 shows the postoperative assessment of wound healing after treatment with the thulium laser, Vela, and Fig. 2 shows the postoperative assessment of the findings. The results of the questionnaire are shown in Table 1. Pain could be expressed on a scale of 0–10, with 0 representing no pain and 10 representing maximum pain. Burning, itching, pain, bleeding, discharge, and skin irritation were stated as side effects, which are shown in Fig. 3. Figure 4 shows the location of condylomas treated with the thulium laser.
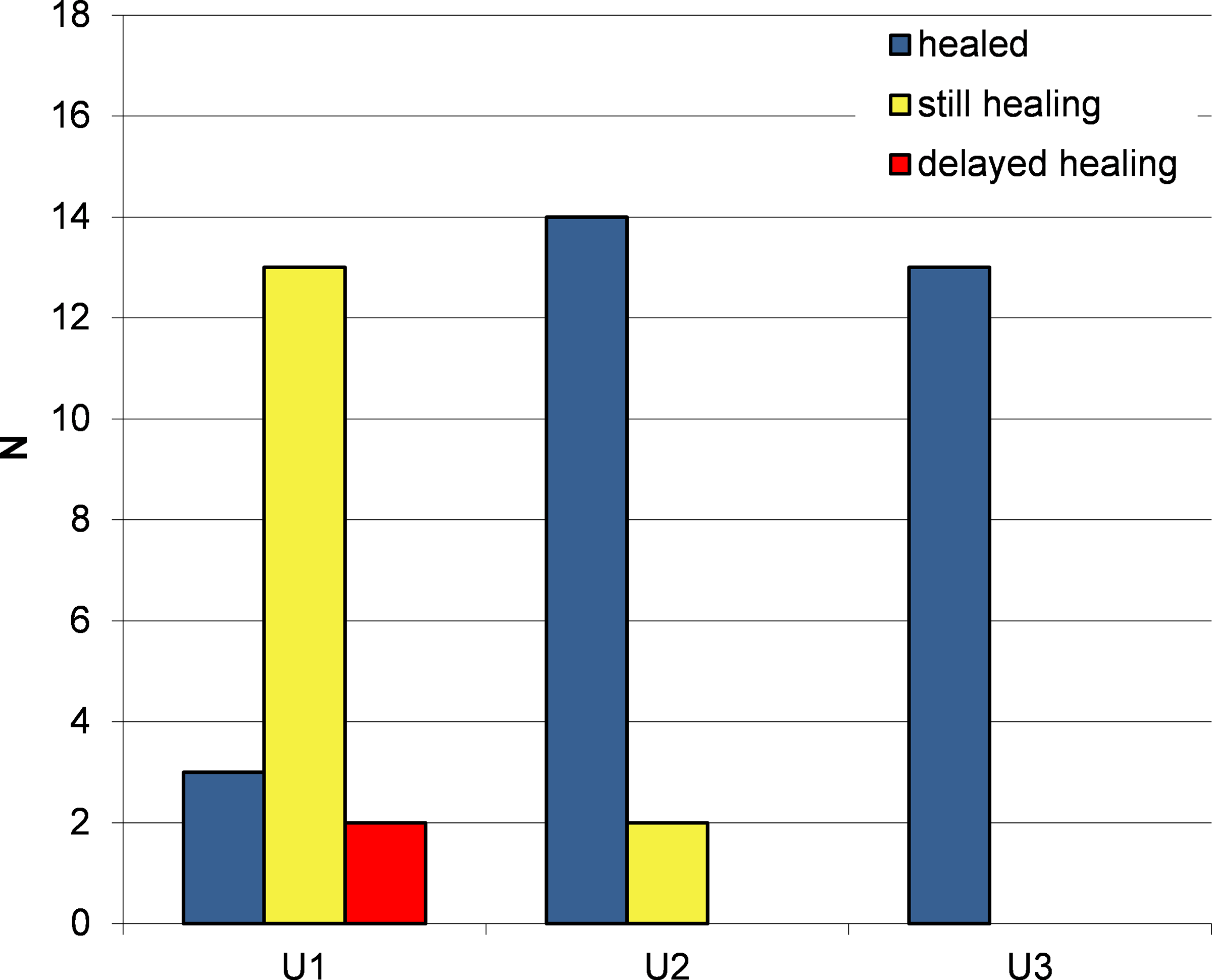
Postoperative evaluation of the wound healing after treatment with the thulium laser Vela® (StarmedTec, Starnberg) during the follow-up appointments after 1–2 weeks (U1), after 3 months (U2), and after 6 months (U3).

Postoperative evaluation of the finding after treatment with the thulium laser Vela® (StarmedTec, Starnberg) within the follow-up appointments after 1–2 weeks (U1), after 3 months (U2), and after 6 months (U3). CR, complete remission; PR, partial remission.
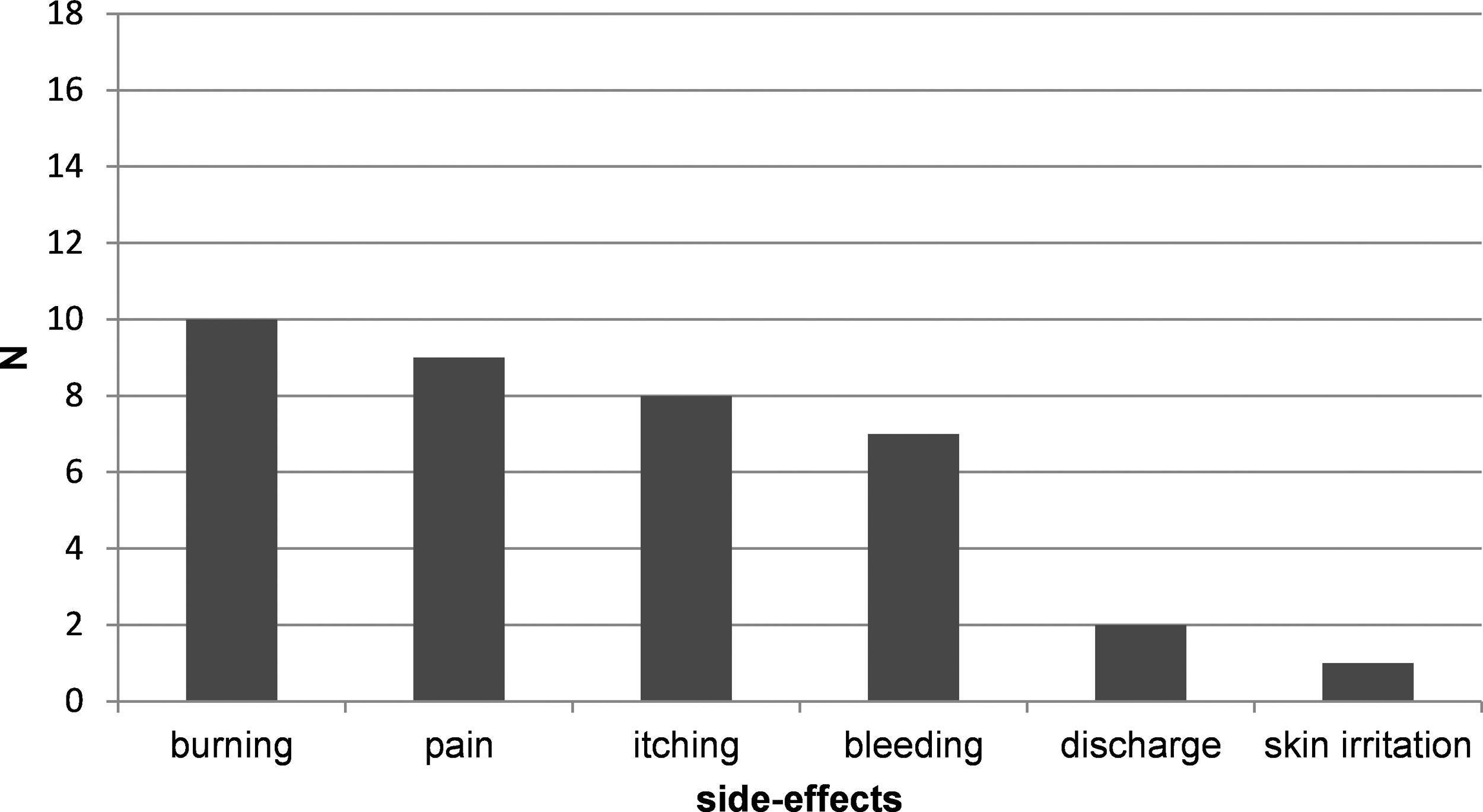
Stated side effects after treatment with the thulium laser Vela® (StarmedTec, Starnberg).
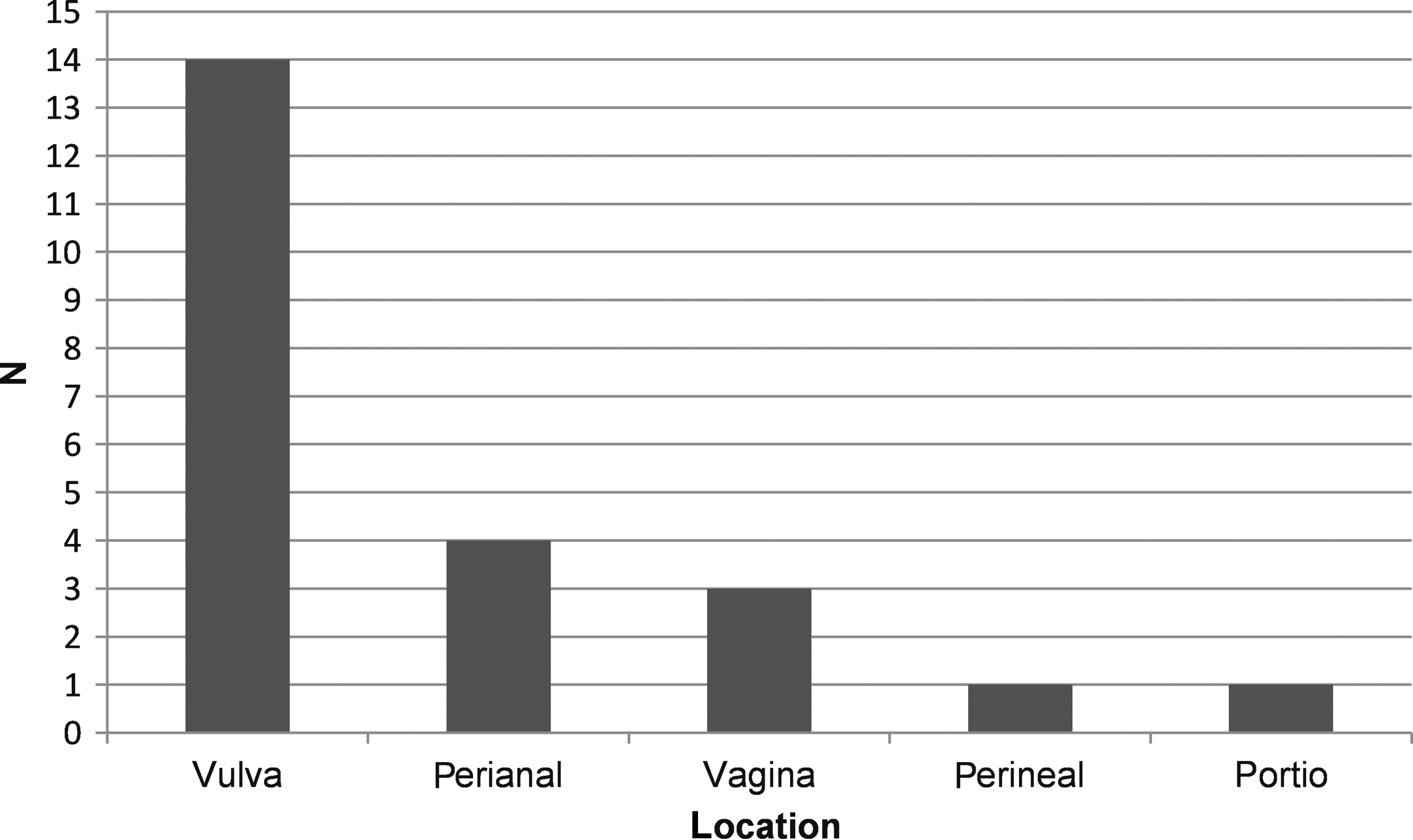
Location of condylomas treated with the thulium laser Vela® (StarmedTec, Starnberg).
Discussion
The treatment of condylomas and cervical, vaginal, and vulval intraepithelial neoplasias using CO2 laser (10.6 μm) is still a tried and tested good standard technique. 2 The wavelengths of both the CO2 laser and the thulium laser exhibit good absorption in water and are, therefore, suitable for the ablation of tissue. However, as a result of its higher wavelength, the CO2 laser can only be guided using mirror joints. In contrast, the thulium laser can be guided via a fiber and, therefore, offers the greatest flexibility. Application of the thulium laser is shown in Fig. 5.
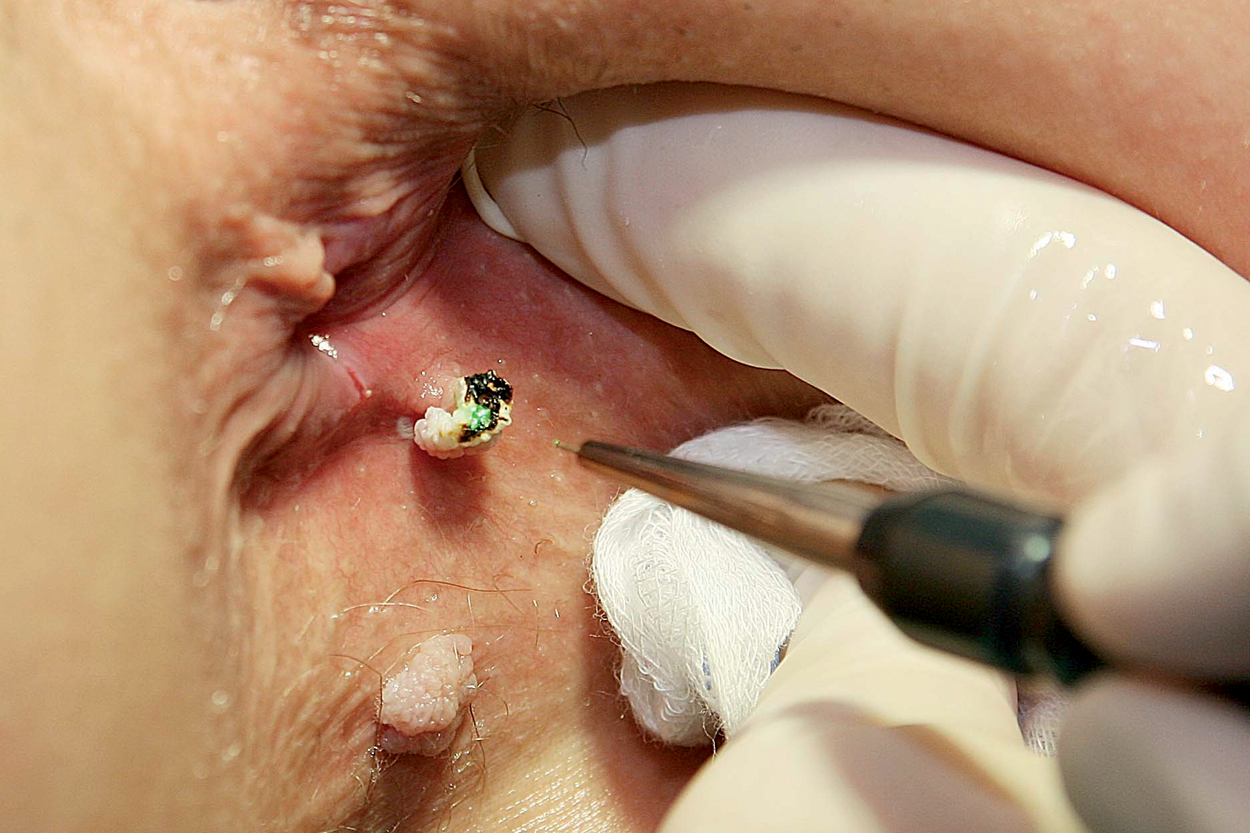
Application of the thulium laser. Vaporization of perianal condylomas with the thulium laser Vela® (StarmedTec, Starnberg).
The thulium laser, Vela, with a wavelength of 1.9 μm, power range of 5–50 W, and laser beam delivery via a fiber system, can be used for vaporization, deep destruction, and hemostasis, and also can be used as a laser scalpel. We investigated a further application for this laser, which is already commonly used in other disciplines. 7,8 Laser vaporization of the vagina, vulva, and cervical portio could be performed without difficulty. Minimal bleeding occurred during treatment, and the vaporized area was usually completely dry after the end of the procedure. With regard to tolerability, it can be said that no side effects occurred during the treatment of cervical changes, and few occurred during treatment of vaginal and vulval changes. Side effects were surveyed using the questionnaire and the history taken at the follow-up appointments. Itching, burning, pain, bleeding, discharge, and skin irritation were listed as side effects.
As CO2 laser conization is possible, a further study to evaluate the possibility of thulium laser conization to make a comparison between these two lasers would be interesting.
In comparison to the commonly used CO2 laser, use of the thulium laser gave the impression of a slight deterioration in the vaporization of the tissue to be removed. This can be explained by the lower absorption of the thulium laser in water compared with the CO2 laser. The handling of the thulium laser was very comfortable because of the laser beams being delivered via a fiber system.
In the case of HPV-induced condylomas, the probability of relapse is up to 75% with surgical treatment. 11 Relapse rates of 60–77% occur after treatment with a CO2 laser. 12 In this study, the relapse rate with the thulium laser of condylomas was 40% (n = 6) during the 6-month follow-up. No relapse of CIN I, II occurred. However, the relapse rate cannot be judged on the choice of laser alone. Additional factors such as occult, not-yet-visible areas infected with the HPV virus, immune status, and, also, nicotine use have to considered. The achieved relapse rate of 40% is less than the relapse rates of up to 75% with surgery. Further investigations with a higher number of treated cases with CIN and/or condylomas are needed for more exact comparison of the relapse rates.
In addition to surgical procedures, local drug treatments of condylomas are also available. For example, imiquimod 5% cream can be used to treat condylomas. Recurrence rates of <20% can be achieved. A disadvantage of local drug treatment is the long duration of the treatment, and irritation and swelling in the genital area. 11
None of the available treatment methods, surgical and conservative, can definitely remove genital warts permanently.
Conclusions
This feasibility study shows that the use of the thulium laser for the vaporization of cervical neoplasias and condylomas offers a good alternative to the standard treatment using a CO2 laser.
Footnotes
Author Disclosure Statement
No competing financial interests exist.