
Abstract
Introduction
E
To date, various products and techniques have been recommended for removing the CH from root canals. The most commonly described technique is the shaping of the root canal using a master apical file and copious irrigation at working length. 7 Several studies 2,7 –10 have examined different intracanal irrigants such as saline, sodium hypochlorite (NaOCl), ethylenediaminetetraacetic acid (EDTA), and citric acid, along with combinations for removing CH. According to the results, EDTA and other acid solutions have been found more effective than NaOCl and saline. 8,9 However, none of them removed the CH from the dentin walls completely. These results showed that it is difficult to completely remove the CH using the irrigants alone. Therefore, various irrigation agitation techniques, including mechanical instrumentation with rotary and patency files or sonic or ultrasonic devices, and laser irradiation have been improved. However, there is still no general consensus on the most effective technique.
The use of laser technology has been shown to be relatively safe, and has been proposed for various dental treatments such as reducing tooth sensitivity, removing caries, cavity or root canal preparation, disinfecting dental tissues, and bleaching. Some effects of using lasers, including vaporization of soft tissue, removal of the smear layer or intracanal medicament, and melting of dentin surfaces, have gained popularity in endodontic treatment. 11,12 In previous studies, 13 –15 near-infrared lasers [diode and neodymium:yttrium-aluminium-garnet (Nd:YAG)], medium-infrared erbium-family lasers [erbium:yttrium-aluminium-garnet (Er:YAG) and erbium, chromium: yttrium-scandium-gallium garnet (Er,Cr:YSGG)], or far-infrared carbon dioxide (CO2) lasers were used, and the effectiveness of these lasers in root canal disinfection when used in conjunction with root canal irrigants such as NaOCl or EDTA has been confirmed. The mechanism for the laser activation of irrigating solutions originates from the absorption of laser energy, the formation of vapor bubbles, the collapse of the bubbles, acoustic streaming, and, finally, cavitation. 16,17 Irrigants are also used during lasing to reduce thermal stress to the radicular dentine and periodontium. 18
QMix 2in1 (Dentsply Tulsa Dental, Tulsa, OK) is a novel irrigating solution for smear layer removal and disinfection with added antibacterial agents; it contains EDTA, chlorhexidine, a detergent, and water. 19 Normally, the combination of EDTA and chlorhexidine (CHX) produces the formation of precipitate, but in QMix 2in1 this is avoided because of its formulation. 20 It is a clear solution, ready to use, with no chairside mixing required. Previous studies 19 –21 showed that QMix 2in1 removed the smear layer effectively.
Peracetic acid (PAA) is one of the strongest oxidizing agents, with antibacterial, sporicidal, antifungal, and antiviral effects. 22 For this reason, it has been used as a disinfectant for dissolving biofilms in different areas. The acetic acid content is suggested to be responsible for the inorganic material dissolution. Acetic acid also bonds to calcium to form complexes that are easily soluble in water. 23 In endodontics, the use of low concentrations of PAA are recommended as a final irrigant to remove the smear layer or CH and to disinfect the root canals. 23 –25
The aim of this study was to compare the efficacy of the Er,Cr:YSGG laser at low-energy laser settings with different irrigation solutions (NaOCl, EDTA, QMix 2in1, and PAA) in removing CH from artificial grooves created in mandibular premolar root canals. The null hypothesis was that irrigation solutions and application techniques did not differ in the removal of CH.
Materials and Methods
A total of 160 freshly extracted mandibular single-rooted premolars were selected in this study. Soft tissues and calculus deposits were mechanically removed from the root surfaces with a periodontal scaler. The exclusion criteria were a tooth having more than a single root canal and apical foramen, root canal treatment, internal/external resorption, immature root apices, caries/cracks/fractures on the root surface, and/or root canal curvature >10 degrees. Both buccolingual and mesiodistal preoperative digital radiographs were taken for each tooth to confirm the canal anatomy. The teeth were then stored in distilled water at room temperature until use.
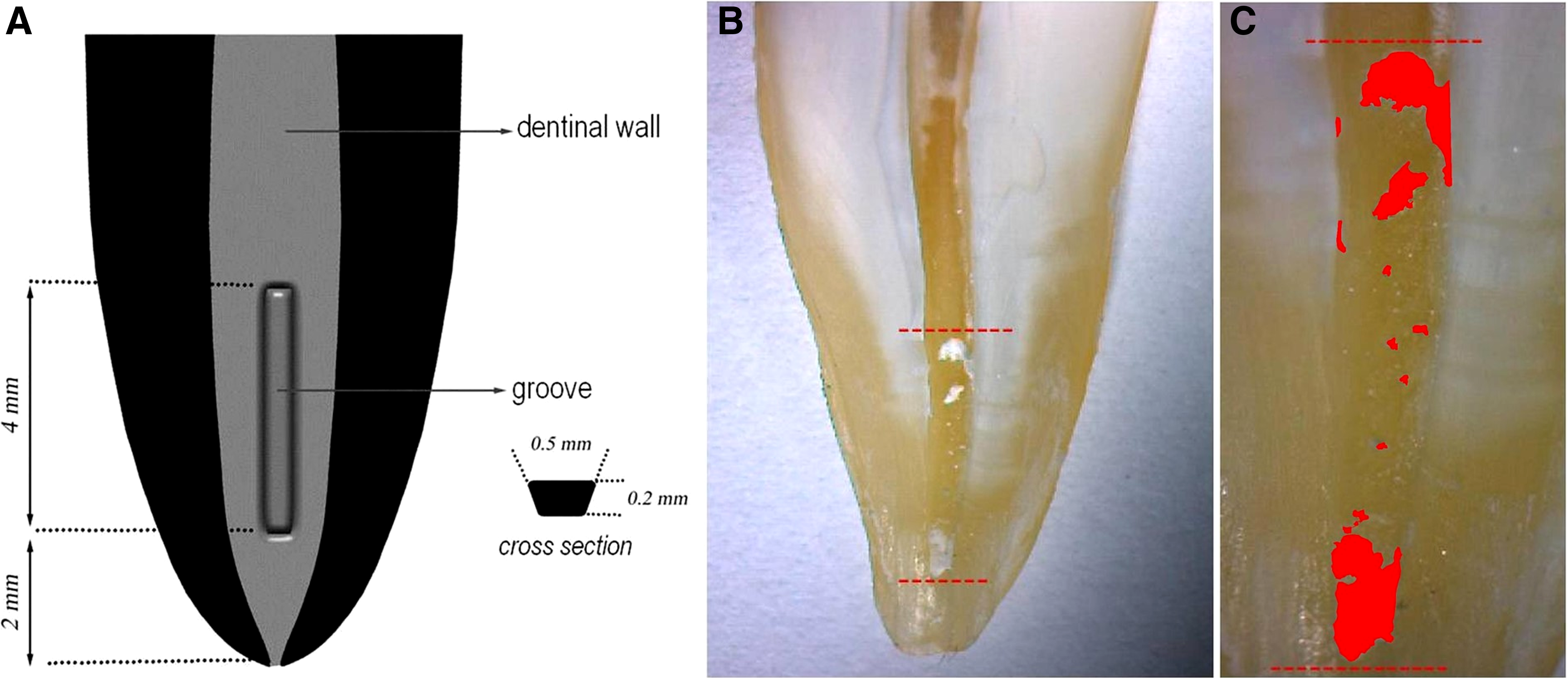
To ensure standardization, the crowns of the teeth were partially removed with a diamond disc under water coolant to achieve a final 15 mm root length for each tooth. A size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) was then placed in the canal until it was visible at the apical foramen. Working length (WL) was determined by subtracting 1 mm from this measurement. Root canals were shaped with ProTaper Universal rotary files (Dentsply Maillefer) up to size F4 as the master apical file. During the preparation, root canals were irrigated with 1.5 mL of 2.5% NaOCl via a size 27-gauge open-ended standard tip needle (Ultradent, South Jordan, UT) between each file change. After completion of the instrumentation, a final flush was applied using 5 mL of 17% EDTA for 1 min and 5 mL of 2.5% NaOCl for 1 min. The canals were then dried with paper points. The specimens were fixed in Eppendorf vials with silicone (Optosil; Heraeus Kulzer, Hanau, Germany). After removal from the impression material, all the roots were grooved longitudinally on the buccal and lingual surfaces with a diamond disc under copious water irrigation, avoiding penetration into the root canal. The roots were then split into two halves with a small chisel. A longitudinal groove, ∼4 mm long, 0.5 mm wide, and 0.2 mm deep, was then cut in the root canal wall of one half of each tooth at a distance of 2–6 mm from the apex with a scaler adapted to an ultrasonic device to simulate an uninstrumented canal extension in the apical region (Fig. 1A). A toothbrush was used to remove debris from the root halves and grooves, and the canals were then irrigated with 5 mL of 17% EDTA for 1 min and 5 mL of 2.5% NaOCl for 1 min. The canals were finally rinsed with 5 mL of distilled water and then dried with paper points.
After that, powder of CH (Kalsin; Spot Diş Deposu, Izmir, Turkey) was mixed with distilled water, and the grooves were filled with CH. The root halves were reassembled, and the specimens remounted in the Eppendorf vials. The coronal accesses were sealed with a temporary filling (Cavit; 3M ESPE, Seefeld, Germany). The teeth were then stored at 37°C at 100% humidity for 1 week. After this period, the coronal accesses were opened, and the removal of CH from the experimental groups was applied by different techniques.
The teeth were randomly coded and blindly allocated by two independent examiners into two main groups (n = 80) according to the selected irrigation techniques (needle and laser activation). Each main group was then divided into four subgroups according to the final irrigation protocols (NaOCl, EDTA, QMix 2in1, and PAA) for CH removal.
Experimental groups and protocols, Group A: Needle irrigation (NI) group
Subgroup A1 (NI + NaOCl group)
The removal of CH was performed with a conventional irrigation via a size 27-gauge needle. The canals were irrigated with 6.5 mL of 2.5% NaOCl for 120 sec. The needle was placed at a distance of 1 mm from WL and moved up and down.
Subgroup A2 (NI + EDTA group)
Subgroup A2 was the same as Subgroup A1 with the exception that 6.5 mL 17% EDTA (Werax) was used as the irrigant.
Subgroup A3 (NI + QMix 2in1 group)
Subgroup A3 was the same as Subgroup A1 with the exception that QMix 2in1 was used as the irrigant.
Subgroup A4 (NI + PAA group)
This group was the same as Subgroup A1 with the exception that 1% PAA (Merck, Darmstadt, Germany) was used as the irrigant.
Experimental groups and protocols, Group B. Laser-activated irrigation (LAI) group
Subgroup B1 (LAI + NaOCl group)
The Er,Cr:YSGG laser (Biolase; San Clemente, CA) was focused through a 320 μm radial firing tip (RFT3 Endolase, calibration factor of 0.85, Biolase) with panel settings of 0.50 W, 20 Hz, 25 mJ, and 140 μs pulse. The fiber tip was fixed in the hand piece of the Er,Cr:YSGG laser, and the coaxial water spray and air were switched off. Then, 0.5 mL of 2.5% NaOCl was placed into the root canal and the optical fiber was placed ∼1 mm below the root canal orifice. During the laser irradiation, the root canals were continuously irrigated to maintain hydration and levels using a hand syringe with a 27-gauge needle positioned above the laser tip in the coronal aspect of the access opening. The total activation time was 120 sec, and the total volume of 2.5% NaOCl was 6.5 mL.
Subgroup B2 (LAI + EDTA group)
This group was the same as Subgroup B1 with the exception that 17% EDTA was used as the irrigant.
Subgroup B3 (LAI + QMix 2in1 group)
This group was the same as Subgroup B1 with the exception that QMix 2in1 was used as the irrigant.
Subgroup B4 (LAI + PAA group)
This group was the same as Subgroup B1 with the exception that 1% PAA was used as the irrigant.
Finally, the specimens were irrigated with 5 mL of distilled water to prevent further irrigant action.
Image evaluation
After irrigation, the root halves were separated to evaluate the removal of the CH. Digital images at x6 magnifications were captured using a stereomicroscope (Olympus BX43; Olympus Co., Tokyo, Japan) attached to a digital camera, and these were transferred to the computer. The digital images were coded to avoid identifying the specimens. The amount of residual CH in the grooves was measured in mm2 using an image analysis software (ImageJ, US National Institutes of Health, Bethesda, MD) (Fig. 1B, C).
Statistical analysis
Kolmogorov–Smirnov test showed that the data were normally distributed; therefore, one way analysis of variance and Tukey's honest significant difference tests were used to compare the groups at a 95% confidence level (p < 0.05). All statistical analyses were performed using SPSS 20.0 software (SPSS Inc., Chicago, IL).
Results
General results
Table 1 shows mean and SD values of CH residues for each group. The study results showed that LAI was superior in removing CH compared with NI, and statistically significant differences were found among the NI and LAI subgroups (p < 0.05).
Mean with same letter is not significantly different at p = 0.05 level.
CH, calcium hydroxide; NaOCl, sodium hypochlorite; EDTA, ethylenediaminetetraacetic acid.
NI groups
NaOCl left significantly more CH than the other groups (p < 0.05). However, there was no significant difference among the EDTA, QMix 2in1, and PAA groups. The mean percentage values of the remaining CH was 61%, 41%, 38%, and 46% for the NaOCl, EDTA, QMix 2in1, and PAA groups, respectively.
LAI groups
NaOCl left significantly more CH than the other groups (p < 0.05). However, there was no significant difference among the EDTA, QMix 2in1, and PAA groups. The mean percentage values of the remaining CH was 20%, 8%, 6%, and 9% for the NaOCl, EDTA, QMix 2in1, and PAA groups, respectively.
Discussion
Optimizing root canal disinfection and preventing reinfection are essential for the success of endodontic treatment. Complete disinfection is impossible because of the complex root canal anatomy, which includes the lateral and accessory canals, isthmuses, and deltas. Regardless of the instrumentation technique used, large areas of the root canal walls can remain untouched. 26 Therefore, it is also necessary to disinfect root canals via chemical means using different intracanal medicaments and irrigating solutions. CH medicament has been established as the most frequently used intracanal medicament because of its antimicrobial efficacy and biocompatibility. 2 Any CH residue on the canal walls negatively affects the quality of the root filling. 4 However, it is difficult to remove CH completely using conventional methods.
To date, various irrigating solutions have been used to remove CH. 7 –10 However, there is limited data about which irrigating solution can be used safely to remove CH from root canals. Therefore, in the present study, NaOCl, as a control, and various other solutions (EDTA, QMix 2in1, and PAA) were chosen to compare their effectiveness in removing CH. QMix 2in1 is composed of 17% EDTA, 2% CHX, and a surfactant. The addition of a surfactant to the chelating agent reduces surface tension and hence increases the ability of the chelator to penetrate the dentine. 27 Previous studies 19,20 have shown that QMix 2in1 is as effective as 17% EDTA for the removal of the smear layer. However, in contrast to these findings, Elnaghy 28 and Eliot et al. 21 reported that QMix 2in1 removed the smear layer more efficiently than EDTA based on the number of fully opened dentinal tubules and the efficacy of debris removal along the dentinal wall. To date, there has been no study on the CH removal effect of QMix 2in1 in the literature. Besides, only one study 24 has examined the same effect of PAA. Sagsen et al. 24 recommended the 1% PAA solution for the removal of CH from root canals. The findings of the present study showed that the use of 2.5% NaOCl as an irrigating solution was not found to be significantly more effective than 17% EDTA, QMix 2in1, or 1% PAA. However, there was no significant difference among EDTA, QMix 2in1, and PAA irrigants.
In the present study, Er,Cr:YSGG laser activation with different irrigating solutions (NaOCl, EDTA, QMix 2in1, and PAA) was used to remove CH from an artificial groove created in straight root canals, and this was compared to NI with the same irrigating solutions. The findings of the current study show that the complete removal of CH from the grooves was not obtained. However, activation of the irrigant with the laser was shown to be more effective than NI in removing CH from the root canal walls. Therefore, the null hypothesis that there is no difference among various irrigation techniques and solutions is rejected.
NI is the standard procedure for root canal irrigation, but unfortunately, this technique is not efficient in the apical part of the root canal. 29,30 It is particularly difficult to completely remove the residual smear layer, debris, or CH in that region because the apical part's dimensions and complex anatomy impede the circulation and action of the irrigating solutions. 31 For this reason, acoustic and hydrodynamic activations of the irrigant have been developed, 32 and these techniques have been shown to increase the efficiency of cleaning. One of these techniques, the use of laser agitation with different wavelengths, has been proposed as an adjunct to conventional endodontic cleaning procedures. 10,17,29,30,33,34 A new laser agitation technique, photon-initiated photoacoustic streaming (PIPS), has also been proposed. This technique differs from other agitation techniques as only the tip of the device is placed into the orifice instead of placing the tip within the canal. 10 The technique is based on photoacoustic and photomechanical phenomena, which make it different from other agitation techniques. 17 PIPS technique uses low energy levels and short microsecond pulse rates to generate peak power spikes. Each impulse interacts with the water molecules, creating expansion and successive shock waves that lead to the formation of a powerful streaming fluid and facilitate three-dimensional (3D) movement of the irrigant. 17,29,34 Generally, erbium lasers (Er:YAG or Er,Cr:YSGG) are used with different fiber tips (radial/stripped or radial) at subablative power settings in this technique. In the present study, we used Er,Cr:YSGG laser with a 320 μm radial/plain endodontic fiber tip (RFT3). Previous studies 34 –36 showed that the LAI using PIPS tips has been shown to be significantly more effective at cleaning the dentinal walls compared with conventional, sonic, or ultrasonic irrigation techniques.
The use of lasers can cause some side effects in the root canal, such as carbonization and cracks, collateral damage, apical extrusion of the solution, and temperature increases. 37,38 In our study, to avoid some of the side effects associated with the use of the Er,Cr:YSGG laser, the fiber tip was placed into the coronal reservoir of the root canal. During laser irradiation, the root canal was irrigated continuously to maintain the hydration level.
Previous studies 14,30 have used an artificial standardized groove model in evaluations of CH removal. This groove model makes it possible to standardize the size and location of the grooves and the amount of medicament used before irrigation protocols. 30 However, a drawback of this model is that it does not simulate the complexity of a natural root canal anatomy. 9 In addition, this experimental model does not show evidence of medicament penetrating into dentinal tubules. In the present study, the artificial standardized groove model was created in the apical part of the root canal to simulate canal irregularities. Studies 5,7 have reported that the removal of CH from the apical part of the root canal wall is very difficult and, accordingly, more CH residues remain in this part.
The amount of residual CH in the canal walls was calculated by measuring the surface area of residues in terms of mm2, 39 by using a scoring method. 9,14 This was performed using either scanning electron microscopy 40 or a volumetric analysis by computed tomography. 8,41 In the present study, a surface area measurement method was used. The surface area count (mm2) of residual CH on the groove walls was recorded as a percentage of the overall groove surface using an image analysis program. However, the main limitations of this technique are loss of residual CH during splitting and variation between observers, because of subjective evaluation or underestimation of remnants as a result of two-dimensional imaging. 42
In the present study, the split-tooth model was used for surface area measurement. Although this model provides a number of advantages to laboratory studies, such as reproducible in vitro evaluations, direct comparison of applications, and elimination of tooth morphology variability, it cannot exactly simulate in vivo conditions. 43 Also, the split-tooth model does not recreate a perfectly restricted canal. 44 In some previous studies, the presence of lateral extrusion of heated gutta-percha or irrigating solution was seen between the two halves of the model. 43 –46 In the present study, the tendency for the irrigating solutions to flow into the interface between the two halves during the removal of CH may be a contributing factor in the failure to completely remove CH from the root canals.
Conclusions
Within the limitations of the present study, it was found to be impossible to completely remove CH from the root canal with tested techniques. However, LAI was significantly more effective than NI. This technique could be beneficial in endodontics for activating irrigation solutions. NaOCl left significantly more CH than the other irrigants used. However, EDTA, QMix 2in1, and PAA showed similar effects. The techniques were compared in straight root canals, and further studies should be conducted to evaluate the effectiveness of the techniques in curved root canals.
Footnotes
Author Disclosure Statement
No competing financial interests exist.