
Abstract
Introduction
O
A considerable body of evidence has been building to support the use of low-level laser therapy (LLLT) for reducing the severity of oral mucositis in HSCT patients. A recent update of the Mucositis Guidelines of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) recommended the use of LLLT (applied to the oral mucosa) for the prevention of oral mucositis in adult patients receiving HSCT conditioned with high-dose chemotherapy. 7,8 However, no guideline was developed for the pediatric population, because of insufficient evidence. Further, most protocols to date have evaluated only a direct intraoral use of the laser. Experts have suggested that extraoral application of the laser can also have beneficial effects on oral mucositis. 9 However, we could find no published studies on extraoral laser application for oral mucositis. Because difficulty swallowing (resulting from oropharyngeal mucositis) is a common complaint in HSCT patients, this study examined the use of an extraoral laser targeted to the oropharyngeal area, combined with an intraoral laser targeted to the more accessible intraoral areas. Therefore, the goal of this study was to evaluate a protocol combining intraoral and extraoral laser application for the prevention of oral mucositis in a pediatric HSCT population.
Methods
Twenty-four children receiving a HSCT at the Pediatric Oncology Institute—Support Group for Child and Adolescent with Cancer (Grupo de Apoio a Criança e Adolescente com Cancer–GRAACC), Federal University of São Paulo (Universidade Federal de São Paulo (UNIFESP), São Paulo, Brazil, were included in this study. All patients or their parents signed institutional review board (IRB)-approved informed consent forms. Twelve patients who received HSCT between January 2010 and June 2010 were included in the laser therapy group. Twelve other patients who received HSCT between August 2000 and January 2006, and had not received laser therapy, formed the retrospective control group.
Prior to chemotherapy administration, all patients had a comprehensive oral examination to identify and treat potential sources of oral infection that could compromise the HSCT. The oral evaluation included panoramic radiographs for all patients. During the study period, oral hygiene practices were standardized for all subjects. The basic oral hygiene was performed with soft brushes after every meal. 2,8 All subjects also used a mineral water mouthwash every 2 h following the administration of chemotherapy. All subjects, in addition to the conditioning chemotherapy regimen, received prophylaxis with acyclovir and fluconazole per institutional protocol. In addition, the subjects who had allogeneic transplants were administered cyclosporine or tacrolimus with or without mycophenolate mofetil or methotrexate, to prevent graft versus host disease (GVHD). The preceding protocol is standard of care at the study site, and was received by patients in both the test group and the retrospective control group. 10 No specific intervention for oral mucositis was administered, other than the LLLT in the test group.
LLLT
Laser therapy began on the 1st day of the conditioning chemotherapy regimen and ended on the day of healing of the ulcers or the day of engraftment (defined as the 3rd day of 3 consecutive days with absolute neutrophil count ≤0.5 × 109/L, following the nadir of the chemotherapy-induced neutropenia). The laser therapy was performed four times a week (Monday, Tuesday, Thursday, and Friday). Prior to applications, the equipment was cleaned with alcohol and the tip was covered with a plastic wrap to avoid direct contact with the subjects' mucosa. During the application, the examiner and all subjects used safety glasses.
For intraoral laser therapy, we used an InGaAIP Diode Laser (Therapy XT, DMC Equipment Ltd, São Carlos, Brazil), emitting red light with wavelength (λ) = 685 nm in continuous mode with a spot size of 600 μm. The parameters applied in the protocol were: power, P = 35 mW; exposure time, t = 10 sec per point; distributed energy per point = 0.35 J, for a total of 19 points, with a total energy of 6.65 J per day. For this, we used the equation: E = P x t. The laser was calibrated prior to each application using a Laser Check® power meter (Coherent, Santa Clara, CA).
The intraoral application of laser therapy was performed at the anatomical regions most prone to oral mucositis, such as the labial and buccal mucosa, the ventral surface of the tongue, and the floor of the mouth. A total of 19 points were treated as shown in Fig. 1.
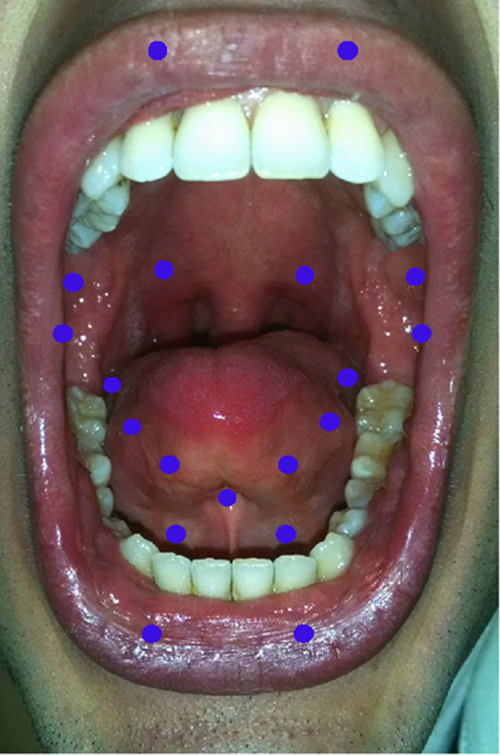
Intraoral points treated with low-level laser therapy. Each treated point is marked by a circle.
In addition, extraoral laser therapy was administered using a GaAIAs laser. (Therapy XT, DMC Equipment Ltd, São Carlos, Brazil) The parameters applied in the extraoral protocol were: wavelength of 830 nm, power 80 mW, exposure time of 30 sec per point, the area of optical fiber 600 μm, distributed energy per point 2.4 J, total of 14.4 J per application. The six points treated extraorally are depicted in Fig. 2.
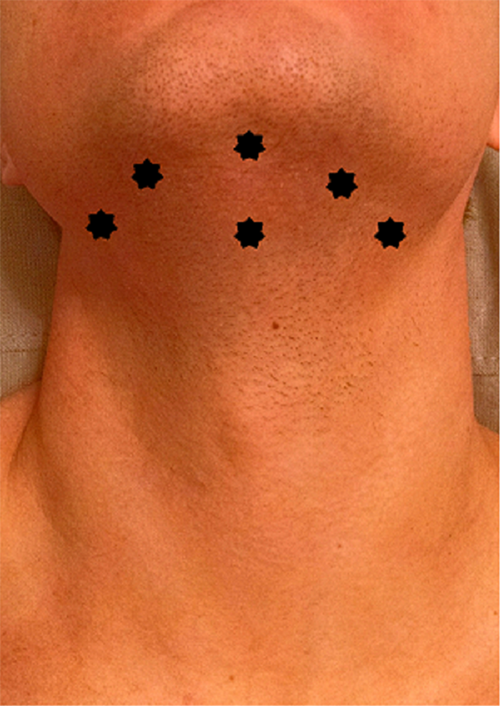
Extraoral points treated with low-level laser therapy. Each treated point is marked by a star.
Assessment of oral mucositis
In the prospective laser group, scoring of oral mucositis was performed four times a week (Monday, Tuesday, Thursday, and Friday) by two independent examiners. In the retrospective control group, scoring of oral mucositis was performed as part of routine patient care. All scoring of oral mucositis was done using the clinical and functional oral mucositis scales of the National Cancer Institute (NCI) Common Terminology Criteria for Advance Events (CTCAE) version 3.0. 11
Statistical analysis
Clinical and functional mucositis scores were compared between the laser and control groups using an ANOVA test. To specifically examine the effect of LLLT on the incidence of ulcerative oral mucositis, clinical NCI grades II, III, and IV were grouped as “ulcerative oral mucositis,” whereas clinical NCI grade I (erythema only) or no mucositis (grade 0) were grouped as “no ulcerative oral mucositis.” To specifically examine the effect of LLLT on the loss of function associated with oral mucositis, we grouped functional NCI grades I and II as “adequate oral alimentation possible” and grades III and IV as “adequate oral alimentation not possible.” To compare these groups, we applied Fisher's exact test. A p value <0.05 was considered significant for all tests.
Results
Patient characteristics are listed in Table 1. The laser and control groups were similar with respect to age, gender, cancer diagnosis, chemotherapy regimen, and type of transplant.
ALL, acute lymphoblastic leukemia; AML, acute myelogenous leukemia; CTX, cyclophosphamide; HL, Hodgkin's lynphoma; NHL, non-Hodgkin's lymphoma; TBI, total body irradiation.
Effect of LLLT on clinical severity of oral mucositis
The distribution of clinical mucositis scores in the laser and control groups is shown in Fig. 3. Patients receiving LLLT experienced less severe oral mucositis than the control group. In the laser group, three patients had no oral mucositis (grade 0), four had erythema only (grade I), four had grade II, only one had grade III, and no patient had grade IV mucositis. In contrast, in the control group, no subjects escaped oral mucositis, with only one patient having grade I, six having grade II, four having grade III, and one having very severe grade IV mucositis. This difference in the distribution of clinical mucositis scores between the two groups was highly significant (p = 0.004). Because LLLT was used to prevent ulcerative oral mucositis, we also compared the incidence of ulcerative oral mucositis (grades II, III, and IV combined) between the two groups. Five of 12 patients (41.7%) in the laser group experienced ulcerative oral mucositis as compared with 11 of 12 (91.7%) in the control group. This difference was also statistically significant (p = 0.027).
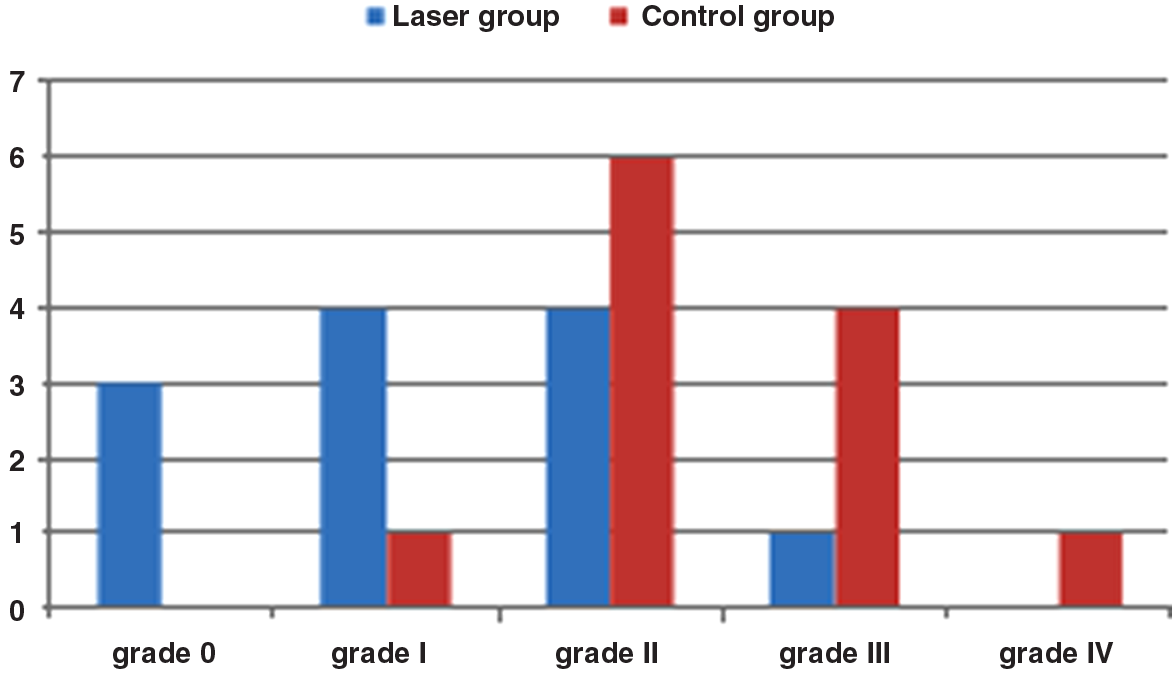
Distribution of clinical mucositis scores in the laser and control groups. Each bar represents the number of patients who experienced that grade of clinical oral mucositis in the laser or control groups.
Effect of LLLT on functional limitations associated with oral mucositis
The distribution of functional mucositis scores in the laser and control groups is shown in Fig. 4. Patients who received LLLT experienced less severe dietary/swallowing limitations associated with oral mucositis than the control group. In the laser group, seven subjects could continue a normal diet (grade I), three subjects could swallow a modified diet (grade II), and two were unable to adequately eat or drink orally (grade III). In contrast, in the control group, only four subjects could continue a normal diet (grade I), two could swallow a modified diet (grade II), and six were unable to adequately eat or drink orally (grade III). No subjects developed grade IV (life-threatening) functional symptoms in either group. This difference in the distribution of functional mucositis scores between the two groups was not statistically significant (p = 0.114).
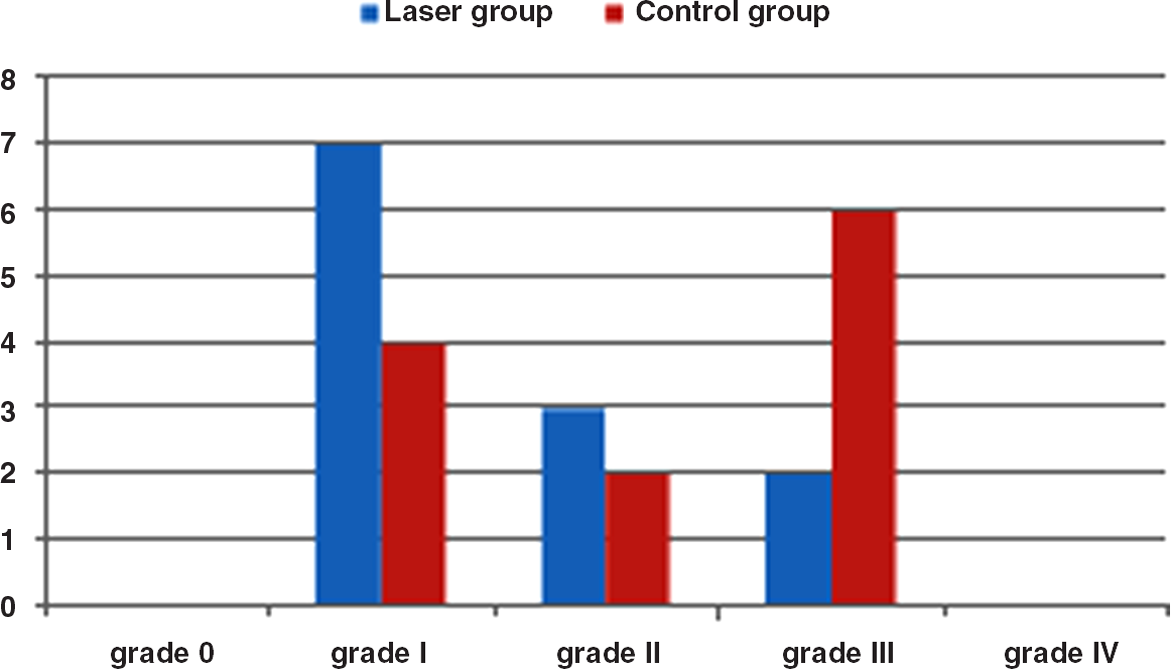
Distribution of functional mucositis scores in the laser and control groups. Each bar represents the number of patients who experienced that grade of functional oral mucositis in the laser or control groups.
Because an inability to adequately eat or drink is associated with the need for supportive care, including total parenteral nutrition, we also compared the incidence of grade III functional limitation between the two groups. Two of 12 patients (16.7%) in the laser group experienced this severe degree of functional limitation as compared with 6 of 12 (50%) in the control group. This difference was not statistically significant (p = 0.193).
Distribution of mucositis based on transplant type
The severity of oral mucositis in different types of transplant is presented in Fig. 5 (laser group) and Fig. 6 (control group). No significant difference was seen in clinical or functional oral mucositis scores between patients receiving autologous and those receiving allogeneic transplants.
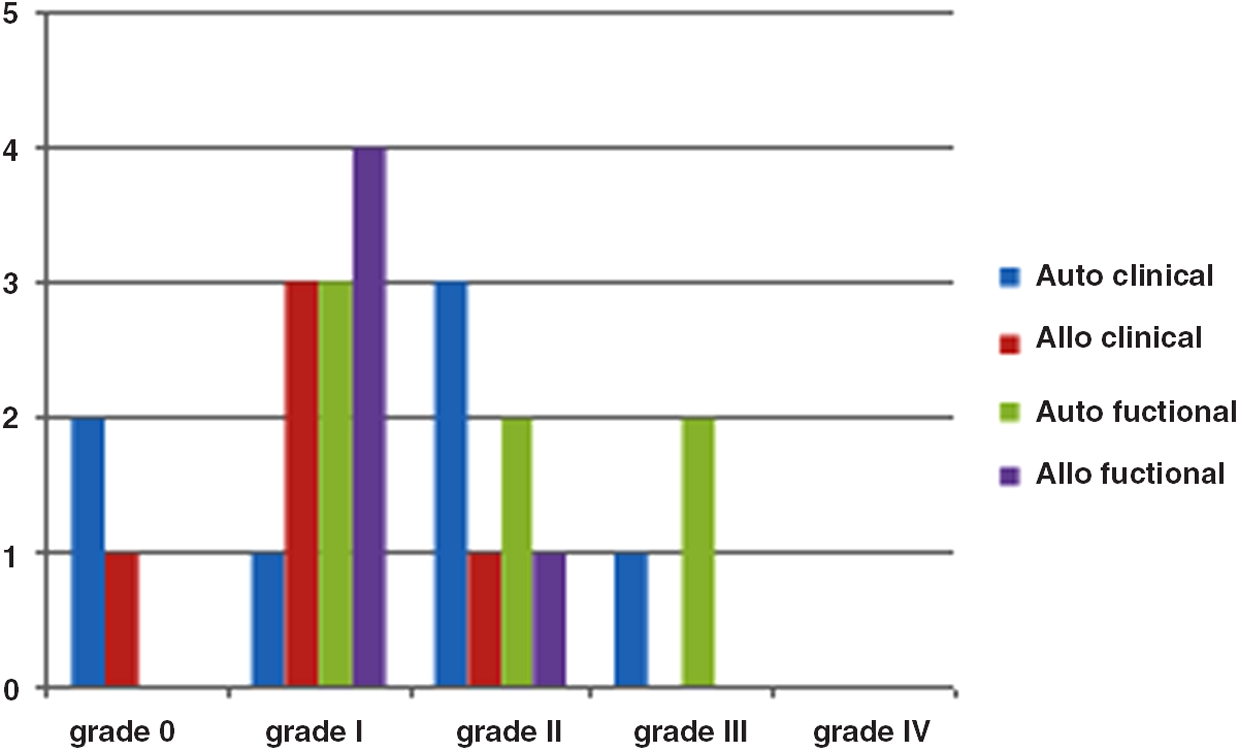
Distribution of clinical and functional oral mucositis scores by transplant type, in the laser group. Each bar represents the number of patients who experienced that grade of clinical or functional oral mucositis.
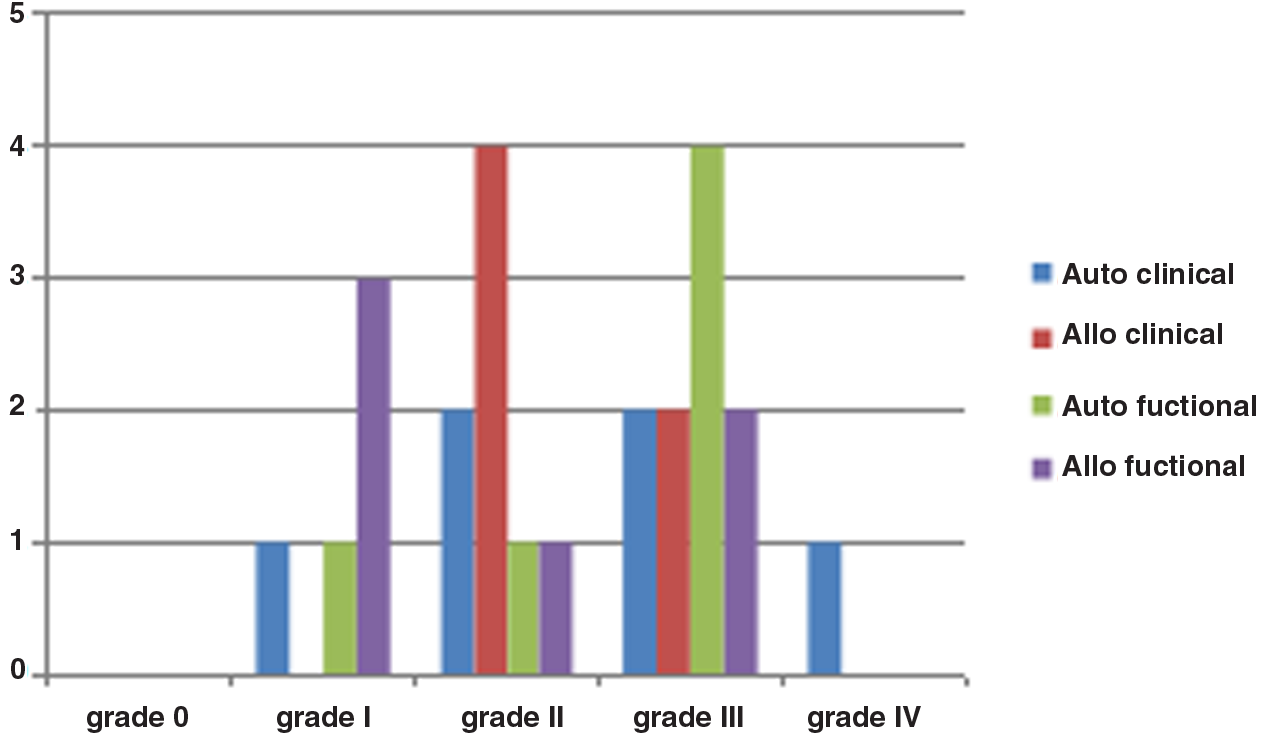
Distribution of clinical and functional oral mucositis scores by transplant type, in the control group. Each bar represents the number of patients who experienced that grade of clinical or functional oral mucositis.
Discussion
The mechanism by which LLLT affects cells is not well understood. Laser energy is absorbed by photo acceptors of the mitochondrial respiratory chain, particularly by cytochrome e oxidase in the mitochondrial membrane. The amount of energy absorption is primarily a function of laser wavelength and the rate of energy delivery, which in turn depends upon the power of the laser. 12 Research has revealed that specific wavelengths of light in the visible and near visible spectrum (at the correct dose, intensity, and pulse frequency) can induce a variety of cellular effects. 13 These include enhancing adenosine triphosphate (ATP), cyclic adenosine monophosphate (cAMP), increasing protein synthesis, and stimulating angiogenesis. 14 Wavelengths between 632.8 and 685 nm 15 have been demonstrated to have a reparative effect by stimulating fibroblast, endothelial, and epithelial cell proliferation. 16,17 All these effects initiate a complex signaling cascade that is essential for the proliferation, regeneration, and protection of various cells and tissues. 18 –22
Mucositis results from a complex series of reactions occurring in both epithelial and subepithelial layers of the mucosa. 23 –25 Studies in animal models have demonstrated that LLLT can reduce the severity of oral mucositis by promoting wound healing, as evidenced by a greater proportion of mature collagen compared with a control group. 16 Further, LLLT has also been found to have an anti-inflammatory effect, with a reduction in neutrophil infiltrate and decreased expression of cyclooxygenase (COX)-2, which is an important inflammatory mediator. 16,26
A number of clinical studies have indicated a beneficial effect of LLLT on oral mucositis in adults. In a systematic review and meta-analysis of 18 randomized controlled trials, Oberoi et al. 27 concluded that the application of prophylactic LLLT in patients with cancer receiving HSCT reduced severe mucositis and pain. Based on the available evidence, the MASCC/ISOO Mucositis Guidelines now recommend the use of LLLT (applied to the oral mucosa) for the prevention of oral mucositis in adult patients receiving HSCT conditioned with high-dose chemotherapy. 7 However, few studies have examined the use of LLLT in pediatric patients. It has been reported that pediatric patients undergoing HSCT have a threefold higher risk of developing oral mucositis, because of a higher proportion of rapidly proliferating cells. 28 The results of this study indicate that LLLT is able to reduce the severity of oral mucositis in pediatric patients undergoing HSCT. Patients who received LLLT had a significantly lower degree of clinical mucositis severity than matched controls. This finding is supported by the previous studies in pediatric patients, even though the laser parameters used differed among studies. 29 –35
Another unique aspect of this study was the combination of extraoral and intraoral laser therapy used. Almost all mucositis studies to date have evaluated only a direct intraoral use of the laser. The ability of low intensity light to penetrate skin with minimal beam scattering (reflection and refraction) permits the use of therapeutic light to effectively treat subdermal lesions. 36 –38 When comparing two sources of light (red and infrared), infrared light spectrum (with a wavelength of >700 nm) penetrates tissue more deeply (between 3 and 5 cm), than red light (between 600 and 700 nm, penetrating 2–5 mm). For this reason, longer wavelengths are usually recommended for treating deeper lesions. 36 –39 Therefore, we used light with a wavelength of 830 nm for the extraoral protocol, as compared with 685 nm for the intraoral application. The rationale for the extraoral application is to impact oropharyngeal mucosa not accessible for direct treatment via the oral cavity. Studies have indicated that the most troublesome symptoms reported by patients with oral mucositis are related to eating and swallowing. 40 The results of this study indicated that the extraoral laser application to the oropharyngeal area resulted in an improvement in functional outcomes related to diet and swallowing. However, these differences did not achieve statistical significance. This may be because of the small sample size, which limited the power of the study. This result may also indicate that direct laser application to the oral mucosa is more effective in ameliorating mucositis than indirect application to oropharyngeal mucosa through the skin.
An important fact to consider is the period of application of laser therapy. In this study, LLLT was initiated at the beginning of the conditioning regimen and continued until neutrophil recovery. Therefore, LLLT was used for a mean period of 22 days. A study by Antunes et al. 41 also used a similar duration of laser therapy. That study also documented a significant reduction in the severity of oral mucositis. In contrast, other studies have used the same laser parameters, but the laser therapy was applied for only 5 consecutive days. 25 In those studies, 100% of the patients presented with oral mucositis after HSCT. This reinforces the concept that the laser-use parameters are of critical importance. In particular, the total duration of time over which laser treatment is performed could be of importance. 16 Additional important variables include the dose, 40,42 and whether LLLT is started before or with the start of the conditioning regimen, or at the first appearance of ulceration 25,29,30,33,35 The number and specific location of sites treated is also an important factor, which varies widely among published studies. This study had the same number of treatment points (19) as used by Abramoff et al.; 30 other studies have provided the anatomic areas stated without specifying the number of points, 32,37 or have not provided any information. 31 The energy per point also varies between studies. For example, this study used 0.35 J per point, whereas Abramoff et al. 30 used 2 J per point. Therefore, there is a need for standardization of laser protocols to determine the optimal parameters for mucositis.
Limitations of this study include the small sample size, with only 12 subjects in each group, which limits the power of this study. However, it is noteworthy that a statistically significant difference in clinical mucositis severity was seen despite the small sample size. Another limitation is the use of a retrospective control group. A concurrent control group receiving sham laser treatment would have been a stronger control. However, at our center in Brazil, the use of LLLT for oral mucositis is now standard of care and it would have been ethically and practically difficult to enroll subjects to a sham laser control group. The retrospective control group was well matched with the laser group on important variables that can affect mucositis severity, which supports the validity of the comparisons conducted.
There were no adverse events associated with the use of laser therapy in this study. Intraoral LLLT is commonly used; however, extraoral LLLT targeted to the oropharyngeal area is relatively new. Azevedo et al. 43 demonstrated that direct infrared laser therapy to the thyroid gland of male mice resulted in alterations to blood thyroid hormone levels. However, the extraoral laser treatment in this study was targeted to the oropharyngeal areas, and there was no direct treatment to the thyroid gland.
Conclusions
In conclusion, this study indicates that a combined protocol of intraoral and extraoral application of LLLT can reduce the severity of oral mucositis in pediatric patients undergoing HSCT. Randomized double-blind clinical trials with a larger number of subjects must be conducted to further test such combined protocols.
Footnotes
Acknowledgments
We thank all the members of the HSCT unit team (doctors, nurses, caregivers, and patients) for their contributions to this study.
Author Disclosure Statement
No competing financial interests exist.