
Abstract
Introduction
S
Healing is a highly dynamic process. The immediate goal in repair is to achieve tissue integrity and homeostasis. The process involves three phases that overlap in time and space: inflammation, tissue formation, and tissue remodeling. 4,5
Several studies have demonstrated a significant clinical value for the use of low-level laser therapy (LLLT) to accelerate the healing of superficial wounds. 6 –8 LLLT has been used in different areas such as wound healing, 9 –11 pain relief, 12 blood microcirculation, 7 orthodontic movement, 13 and anti-inflammatory effect. 14
Many benefits, including stimulation/inhibition of physiological, biochemical, or proliferative activities, are associated with LLLT. 15
Immediately after injury (e.g., mini-implant insertion), the traumatized area, including soft and hard tissues, may suffer ischemic damage, due to a lack of nutrients and oxygen supply. During this initial phase, an immediate inflammatory response starts and may evolve to an apoptosis process in the injured cells. 16 The use of LLLT could reduce or even avoid these injures to the tissue, facilitating the healing process. 11
Cytokines, such as interleukins 6 and 8, are involved in inflammatory responses in peri-implant tissues. 17,18 They are key mediators of tissue damage, tooth movement, and bone turnover. Cytokines are classified as pro- and anti-inflammatory, including tumor necrosis factor and interleukin (IL): IL-1, IL-2, IL-6, and IL-8. These are “alarms” cytokines that induce a series of vascular and cellular reaction, resulting in an inflammatory process and tissue remodeling. 19
IL-8 and IL-6 play a fundamental role in recruiting and activating neutrophils and other cells during inflammation and healing around oral implants. 18 They are secreted mainly by monocytes and are important for regulating alveolar bone resorption during tooth movement by acting at an early stage in the inflammatory response; also, these cytokines are responsible for extracellular matrix degradation and released at higher levels in inflamed gingiva. Yet, IL-6 and IL-8 are commonly released in tissue after injury or trauma and may represent response to both soft and hard tissue to surgical trauma. 17,20
Duarte et al. 21 reviewing the literature about the immunological response following implant insertion in patients found a good correlation between the volume of Crevicular Fluid and the amount of cytokines with mucosal inflammation.
Our aim in this study was, therefore, to evaluate the effects of LLLT on immediate inflammatory response, through the peri-implant crevicular levels of interleukin-6 and interleukin-8 in the initial 3 days after mini-implant insertion, and compare this level with a health tooth.
Materials and Methods
Subjects
The protocol of this study was reviewed and approved by the Institutional Review Board of the São Leopoldo Mandic Dental Research Center, and all trial procedures were conducted according to the principles of the Declaration of Helsinki. Written informed consent was obtained from each subject.
Ten volunteers (six men and four women) with good systemic health condition, checked by individual anamnesis interview and clinical examination, and no use of any kind of anti-inflammatory medication in the 6-month before the experiment and between the ages of 25 and 38 years were selected for this study.
The volunteers were selected from the patients, treated during 2013 in the Orthodontic department at São Leopoldo Mandic Dental Research Center—Campinas, SP, Brazil (Southeast region of Brazil). They all had indication of use of bilateral mini-implants, but during the experimental period, the miniscrews were not activated or loaded with orthodontic force. After the end of the experiment, all received orthodontic treatment according to orthodontic indication and treatment planning.
All the subjects were in good health, no smokers, and they did not present at the moment of the study any circulatory or healing disorder, local inflammation, or sight of recent trauma, such as diabetes, osteoporosis disease, or local gingival inflammation.
Exclusion criteria were pregnancy, lactation, current smoking, and smoking within the past 5 years, use of mouthrinses containing antimicrobials in the preceding 2 months, and long-term administration of anti-inflammatory immunosuppressive medications and hormone replacement therapy.
After radiographic and clinical examination, a bilateral site between the central incisor/lateral incisor or lateral incisor/first premolar was selected to insert the mini-implant, avoiding any risk of damage in the root area.
Mini-implants
Twenty mini-implants (1.6 mm × 7 mm), self-drilling, self-tapping (Neodent, Curitiba, Brazil), were inserted according to the manufacturer's instructions, two mini-implant per volunteer, bilaterally and without any load.
Groups
The mini-implants were divided into two groups: Group 1–10 mini-implants [at the right side] were inserted and received lasertherapy (LLLT) immediately, 24 and 48 h after placement. A diode laser (TwinLaser MMOptics, São Carlos, Brazil) emitting at 660 nm, with 40 mW for 60 sec (total energy of 2.4 J), was used to irradiate directly over the mini-implant (Table 1). The laser beam (area = 0.04 cm2) was positioned over the mini-screw head (around 5 mm height, covering an area of ∼0.6 cm2), creating a light intensity of 0.07 W/cm2 on the gingival surface and an energy density of 4 J/cm2 per irradiation (12 J/cm2 total treatment). Group 2: the other mini-implants, in the opposite side of the same volunteer, were used as a nonirradiated control group (n = 10); the laser beam was covered with an aluminum foil to avoid light emission, but allowing the “bip” sound of the laser equipment; in this way, the volunteers did not know which side was the nonirradiated group.
A third group—Group 3, served as a negative control. Gingival crevicular fluid (GCF) was collected from the same volunteers, using the upper first premolar to compare the normal levels of cytokines during the same period of the study. This tooth did not receive any orthodontic treatment or any load during the experiment.
The peri-implant crevicular fluid (PGF) around the mini-implant, as well as the GCF around the upper first premolar, was collected using two sterile paper points #25 (Dentsply Latin America, Rio de Janeiro, Brazil). The first paper point was inserted into the base of the interface mini-implant/tissue or at the gingival sulcus for 1 min, and after the 1-min interval, a second paper point was inserted for another 1 min. 22 The samples were collected from both sides and from first premolar after 24 (T1), 48 (T2), and 72 h (T3), always during the afternoon. For the sampling, plaque was removed without touching the gingiva, using a water spray, to minimize contamination of the paper point. The site was carefully isolated with cotton rolls (to eliminate contamination from saliva) and gently dried with an air syringe. After sampling, the papers points were stored in sterile Eppendorf tubes and conserved at −20°C. An immunoassay kit for the ELISA test was used to measure IL-6 and IL-8 concentrations.
ELISA
The PGF and GCF were collected by inserting standard paper strips into the sulcus for 30 sec. The samples were immediately placed in tubes containing 250 μL phosphate-buffered saline and protease inhibitor cocktail (Sigma-Aldrich, Saint Louis, MO) and were stored at −70°C for subsequent assays.
Aliquots of each sample were assayed by enzymatic immunosorbent assay (ELISA) to determine the levels of IL-6 and IL-8 according to the manufacturer's recommendation (eBioscience, San Diego, CA). Briefly, 100 μL of detection antibody was added to all wells, except blank, mixed gently, and incubated overnight (16–24 h) at 4°C. Plates were washed three times, and standards and supernatants were added in the respective wells in duplicate. After the incubation time, the plates were washed again and incubated with 200 μL of conjugate for 60 min at room temperature. Plates were washed three times again, and 200 μL of substrate was added and incubated for 15 min at room temperature in the dark. The reaction was stopped by the addition of 50 μL stop solution, and color was measured in an automated microplate spectrophotometer (Epoch; Biotek, Winooski, VT). The total amounts of cytokines were determined as picograms (pg/mL). Results were calculated using the standard curves created in each assay. The ELISA assays were carried out in a blind manner in triplicate.
Statistical analysis
Values are given as means, and error bars are standard deviations. Statistical comparisons between means were performed with ANOVA followed by the Tukey test, using the Software SPSS 20 (SPSS, Inc., Chicago, IL). p < 0.05 was considered as statistically significant.
Results
An increase in interleukin levels was observed for both groups, along the time, when compared to the levels seen on upper first premolar, for all the volunteers. However, the effects of LLLT on inflammatory modulation were significant for the group that received laser irradiation, when compared to the nonirradiated mini-implants on the other side, used as a control.
On the upper first premolar, used as a negative control group, the levels of IL-6 and IL-8 were maintained stable during the initial 3 days and were significantly different (p < 0.05) from the levels observed on the PCF around all the mini-implants for both interleukins at T2 and T3.
The initial values of IL-8 were similar for irradiated and negative control groups in the initial 24 h, but the IL-8 levels for nonirradiated group were significantly higher. However, along the time, they were statistically different among nonirradiated and laser group (p < 0.05). PGF around nonirradiated mini-implants showed higher levels of IL-8, while the irradiated group showed intermediary values and the upper premolar the lowest levels (Fig. 1).

Levels of IL-8 at T0 (0 h), T1 (24 h), T2 (48 h), and T3 (72 h). Note that IL-8 levels of an untreated tooth were stable during the time.
Analyzing the levels of IL-6 at T1, the nonirradiated group presented similar levels than the upper premolar (negative control); however, the group that received irradiation presented higher levels of IL-6 when compared to the other groups. At T2 and T3, the IL-6 levels were similar to both groups, but statistically different from upper premolar (Fig. 2).
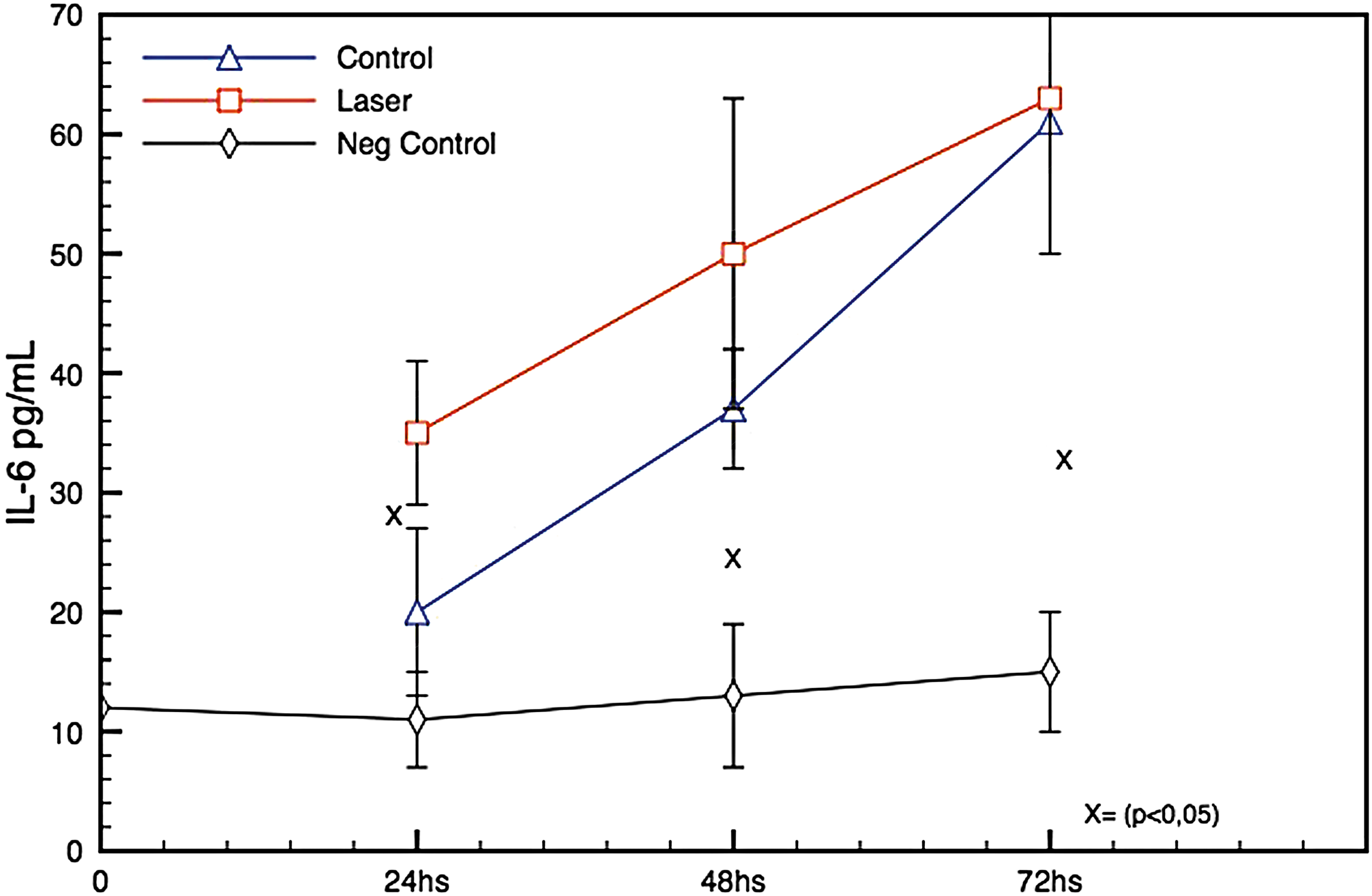
Levels of IL-6 at T0 (0 h), T1 (24 h), T2 (48 h), and T3 (72 h).
LLLT promoted a significant modulation of the IL-8 levels, and the data show a difference when compared to the nonirradiated group. After 24 h of mini-implant insertion, IL-8 levels were similar to upper premolar. For IL-6 levels, there is a significant difference, along the time, for the nonirradiated group during this study, indicating an increase of this cytokine, but for irradiated and nonirradiated groups, the IL-6 levels are higher to upper premolar at T2 and T3.
Discussion
One of the first prerequisites for the success of mini-implants is minimal damage to the host tissues on the insertion site during the surgical process. 22 Despite researchers' and clinicians' efforts, no orthodontic mini-implant system has provided a 100% success rate. Since peri-implantitis turned out to be the main cause of mini-implant loosening, 3,23 –25 assessment of factors involved in such type of inflammation has become crucial to increase mini-implant stability and success rate in orthodontics. 26 Peri-implant inflammation can be responsible for about 30% of miniscrew failures according to Miyawaki et al. 27 Peri-implantitis is a progressive disease, characterized for peri-implant bone loss in conjunction with soft tissue, around implant inflammation. Initially, a mucositis or more precisely a peri-implant mucositis (soft tissue reversible inflammation of the mini-implant surrounding gingiva) appears, which may progress to peri-implantitis if not treated. 28
The sampling of PGF and/or GCF is a useful method for examining cellular dynamics. It is noninvasive, nondestructive, easily applied, and there are some advantages especially for human in vivo studies. 29
The amount of cytokines (IL-6 and IL-8) on GCF collected in gingival sulcus of upper first premolar (that was left untreated and did not receive any load) was as expected, relatively stable during the study. However, the levels of interleukin IL-6 as IL-8 increased after mini-implant insertion, when compared to the tooth in the first 72 h for both groups, indicating the beginning of inflammatory response. The presence of inflammation, on PCF, is possibly due to the trauma caused by ischemic compression over hard and soft tissue, bone deformation, and microfractures. 30
The mini-implants were inserted using the manufacturer's hand driver; thus, variations among the force to insert the mini-implant certainly occur. However, every effort was made to insert the mini-implant with uniform pressure. Yet, the use of a hand driver is more consistent with a clinical setting. Summed with individual anatomy, volume of PGF around mini-implant and distinct biological response could explain the variations on interleukin's levels found in this study among the volunteers.
IL-6 is a multifunctional proinflammatory cytokine, and increased levels are involved in osteoclast recruitment and bone resorption. In studies performed during orthodontic treatment, 31 and in a dental implant study, 32 IL-6 levels increased from the first hour and decreased on succeeding days.
The results showed that the level of IL-6 was higher for the laser group at T1. At T2 and T3, this group presented a slightly increased (not significant), but showed similar levels, than the nonirradiated group at these times, probably achieving values closer to IL-6 peak for both groups, since their levels were significantly higher (sixfold) to the upper premolar. Bellido et al. 33 demonstrated that IL-6 is produced by stromal/osteoblastic cells and is capable of stimulating the development of osteoclasts from their hematopoietic precursors; also, Lópes Carriches et al. 34 stated that this cytokine is one of the most important involved in the physiological response to trauma and furthermore; IL-6 regulates immune responses at inflammatory sites and has autocrine/paracrine activities that stimulate the osteoclast formation and bone resorbing activity of preformed osteoclasts. 17 Moreover, some authors 34 –36 did not observe direct relation between high levels of IL-6 and peri-implantitis, showing that this cytokine is present in bone turnover but does not seem to be involved in bone disease.
Based on the results, it is possible to hypothesize that the initial trauma (first 24 h) stimulated the production of IL-6 to enhance the osteoclast differentiation to reabsorb the traumatized bone accelerating the bone turnover. However, IL-6 level was significantly higher for the irradiated group when compared to the other two groups at T1. In addition, IL-6 did vary along time for the nonirradiated group, showing an increase of its level, but this did not happen for the laser group. On irradiated peri-implant tissues, IL-6 levels were not significantly different along time, possibly suggesting a modulatory effect of LLLT over initial inflammation.
With regard to IL-8, the data showed that both groups had increased levels of this cytokine during the experiment compared to the upper first premolar, confirming the data found by Hamamci et al. 17 In the meantime, for the laser group, the levels of IL-8 were lower compared to the nonirradiated group; yet, at T1, when compared to upper first premolar, the group irradiated presented similar levels. The activity of IL-8 plays a major role in producing inflammatory responses 37 and can be found in the pathogenesis of periodontal disease. 38 On the contrary, orthodontic forces evoke changes in IL-8 levels 29 and significant increases in IL-8 levels can be found, for example, during premolar distalization, and could indicate bone and soft tissue remodeling.
Studies on implants have demonstrated that a rise in proinflammatory cytokine levels, such as IL-8 in crevicular fluid, may indicate the presence of peri-implantitis. 39,40 Nowzari et al. 41 found that IL-6 and IL-8 levels were significantly higher in patients with failing implants than in those with healthy implants. Clinically, all the mini-implants were considered healthy in our study; the levels of IL-8 could indicate that the healing process was modulated by LLLT, since the levels of this cytokine were closer to the levels of upper first premolar, especially at T1.
Our results suggest that LLLT seems to act modulating the inflammatory response increasing IL-6 to reabsorb the traumatized bone area, improving the bone metabolism and turnover, particularly at the first 24 h, a result compatible with the findings of Shaama 32 that found, in cell culture, IL-6 levels increased from the first hour after contact with Titanium material and decreased after 7 and 10 days. In the current research, the levels of IL-6 were higher during experimental time, but were not significantly different to the nonirradiated control group after 48 h of mini-implant insertion. Moreover, LLLT decreased the IL-8, presenting similar levels than normal tissues (T1), which could, in high levels, exacerbate the inflammatory response producing discomfort and increasing the risk of inflammation around mini-implant, fact observed by Hamamci et al. 17
This study used the parameters suggested by Khadra 42 that showed to modulate the activity of cells interacting with an implant, thereby enhancing tissue healing and ultimate implant success. Besides the dose, other parameters must be taken into account, such as wavelength, irradiance, contact or noncontact application, exposure time, type of tissue, physiological conditions, as well as optical properties of the tissue. 7 The irradiation was made with a near infrared laser, allowing a good penetration on gingiva and bone tissue. In addition, we irradiated the lesions in a noncontact uniform way. The laser beam was positioned over the mini-screw head and created a homogeneous light intensity on the gingival surface. Despite that literature suggests the use of direct contact to reduce the energy loss due to reflection, noncontact treatment has the advantage of producing a more homogeneous irradiation in extended surfaces and, in our case, is difficult to promote a uniform irradiation around mini-implant using punctual irradiation, since the metal surface of the mini-implant difficult the light distribution. 43
The use of the same volunteer to compare the effects of LLLT on control, experimental group, and negative control group is a very polemic subject on literature. The risk of bias due to laser irradiation systemic effect cannot be discharged. Rodrigo et al. 10 and Rochkind et al. 44 indicated strong evidences of systemic effect of LLLT on wound healing, nervous system, cutaneous wounds, and burns. However, other authors 45,46 used the same animal as a control and did not establish this effect; in these cited experiments, the laser group/groups showed a significant difference compared to the untreated control group. In our study, there was a significant difference between tissue inflammations on both groups, and, when compared to normal tissue, suggesting that even if the systemic effect was present, this effect was not enough to promote a significant influence on the counter-part miniscrew used as a control or at the periodontal ligament at an untreated tooth, as previously reported in an animal model study from our group. 43
Literature shows that in periodontal and peri-mini-implants tissues, cytokines may have essential roles in modulating inflammatory response. 47 –49 Several biochemical markers have been associated with inflammation and tissue remodeling, especially on osseointegrated dental implants, but only few studies were found in the literature in which biochemical assessments were used to investigate the stability of orthodontic mini-implants. 47 These biochemical characteristics are elsewhere out the scope of this study, since it focused on changes in IL-6 and IL-8 levels during the immediate response to mini-implant insertion. In our study, PGF was collected during 72 h after mini-implant placement and compared to a normal tissue. We believe that more frequent sample collection could have been done during the next weeks, and results of this study could be further confirmed with a larger sample size and evaluation of different cytokines. Supplementary, in this experiment, mini-implants were not immediately loaded and this should be tested in a future study. In addition, the effects of LLLT on alveolar bone remodeling biomarkers are suggested to be monitored during further investigations.
Mini-implant insertion causes an inflammatory reaction on gingival and bone tissues, which, in turn, may trigger the biological processes associated with bone remodeling and soft tissue healing. Furthermore, low-level laser therapy may be useful in reducing inflammation and modulating bone remodeling, decreasing the period of discomfort for the patients and the risk of mini-implant failure.
Conclusions
LLLT modulates the initial inflammation after the insertion of orthodontic mini-implant, keeping IL-8 levels lower when compared to a nonirradiated area, but increasing IL-6 levels, especially in the first day after installation.
Footnotes
Author Disclosure Statement
The authors affirm that they have no financial affiliation (e.g., direct payment, consultantships, honoraria, and so on) or involvement with any commercial organization with direct financial interest in the subject discussed in this article. Any other potential conflict of interest is disclosed.