
Abstract
Introduction
D
The complex anatomy of the root canal system enables bacteria to survive harsh conditions. Enterococcus faecalis, a gram-positive non-spore-forming bacterium belonging to the phylum Firmicutes with streptococci as the nearest neighbor, especially has the ability to form intra- and extraradicular biofilms that partially protect these bacteria from the immune defense, endodontic procedures, and medicaments. 7,8 This fact highlights that this species is the stubborn invader of root canal dentin 9 and that it is – together with Candida albicans – frequently found in secondary root canal infections and recrudescence. 10 All these points together could be responsible for the 14–16% failure rate for initial root canal treatment as reported by Torabinejad et al. and Ng et al. 11,12
Depending on the wavelength, lasers showed better access to formerly unreachable parts of the tubular system. 13 –15 Several studies by Gutknecht et al. 16 Moritz et al., 17 and Schoop et al. 18 have proved the high bactericidal effect of the Nd:YAG laser. Diode laser of 980 nm possesses the ability to penetrate deep inside dentinal tubules. 19 In addition, a limited form of cavitation can be generated in aqueous fluids around the top of the fiber. 20 Castelo-Baz et al. postulated that a synergistic bactericidal effect was observed by combining NaOCl with a 940 nm diode laser against mature biofilm of E. faecalis. The prepared samples were irradiated with 3.5 W, 0.05 ms pulse duration, and 0.25 ms pulse period for 60 sec. 21
Gutknecht et al. showed that within a dentin thickness of 500 μm, the 980 nm diode laser, adjusted to 2.8 W in continuous wave (CW) mode for 32 sec with a fiber diameter of 200 μm, was able to eliminate 86% of the inoculated E. faecalis bacteria. 22 In a comparative study conducted by Franzen et al. 3 the average bacterial reduction was 58% with a dentin slice thickness of 500 μm with Er,Cr:YSGG with a distal output of 0.25 W and a frequency of 20 Hz, whereas Beer et al. 23 reported a reduction of 98.66% with the 940 nm diode laser when irradiating a prepared root sample with 1.5 W, 0.05 ms pulse duration, and 0.15 ms pulse period.
Regarding the improvement of the established delivery systems, radial firing tips (RFT) have been developed that allow a more homogeneous irradiation of the root canal walls. The ends of these RFT show a conical outline with a cone angle of 60 degrees. The laser light, hence, is expanded to a broad cone, facilitating an even coverage of the whole root canal wall that can improve debris removal and the bactericidal efficiency of the laser along root canal system. 24
The objective of this in vitro study was to investigate the depth of antibacterial effect of the dual wavelength (2780 and 940 nm) laser in elimination of E. faecalis by indirect irradiation of dentin slices of different thicknesses in comparison to Er,Cr:YSGG laser alone.
Materials and Methods
Sample preparation
Twenty caries-free bovine teeth were cleaned with a curette to remove tissue remnants. With the aid of a diamond band saw (Exact GmbH, Hamburg, Germany), the teeth were sectioned at the cementoenamel junction. The prepared roots were then embedded in resin material (Technovit® 4071, Heraeus Kulzer GmbH, Germany) and longitudinal sections from bovine teeth were produced with the aid of a saw microtome (Leitz Wetzlar GmbH, Wetzlar, Germany) in slices of three different thicknesses (300, 500, and 1000 μm). All dentin slices were sectioned parallel to the root canal lumen. The thickness of the dentin slices was checked by a vernier and slices below tolerance of ±5 μm were excluded from the study. The resulting total number of 75 precise slices with dimension of 15 × 15 mm (each n = 25 with 300, 500, and 1000 μm) were immersed in an ultrasonic bath with 17% of ethylenediaminetetraacetic acid (EDTA) for 4 min to remove the smear layer, and then thoroughly washed in saline solution. The samples were preserved individually in saline solution at a temperature of 4°C until further use.
Bacterial inoculation
The instruments and the dentin slices in saline solution were sterilized in an autoclave (Napid 30, SMS GmbH, Emmingam-Liptingen, Germany) at a temperature of 121°C for 20 min to remove all contaminants. A region of 10 × 10 mm was marked on the uninoculated side of the slice to specify the area for laser irradiation. According to the methodology of Gutknecht et al. 22 and Franzen et al., 3 the 25 slices of each thickness were inoculated with 1 μL suspension of Enterococcus faecalis (strain ATCC 29212), exactly in the middle opposite to the irradiation area, applying a calibrated micropipette. The bacterial cell concentration was 1.67 × 1010 CFU/mL Luria broth (LB)-medium, such that the 1 μL inoculum contained 1.67 × 107 CFU. In LB-medium E. faecalis forms short chains of 2–8 cells per CFU.
Laser irradiation
Laser irradiation was performed on dentin slices of bovine teeth. The applied dual wavelength laser emits two wavelengths (2780 nm Er,Cr:YSGG laser and 940 nm diode laser) simultaneously (Biolase, San Clemente, CA). The delivery system was via a 415 μm diameter and 21.17 mm length RFT fiber that allowed laser light to be emitted laterally.
The power settings of Er,Cr:YSGG laser were 1.5 W average power, 50 Hz, and 50 μs pulse duration, with 60% water level and 30% air pressure, whereas for diode laser the average power was 2 W. The output power emitted from the distal end of the Mazda 6 (MZ6) laser tip that has a calibration factor of 1 was measured by powermeter (FieldMaxII-Top, Coherent Inc., CA) to ensure a stabile power output. The display settings of 1.5 and 2 W corresponded to an actual power of 1.06 and 0.51 W for Er,Cr:YSGG laser and diode laser, respectively. This difference was the result of the calibration factor of the RFT laser tip (0.85). Also, additional losses were detected as a result of optics coupling in the diode laser.
Dentin slices of every thickness (n = 25) were divided randomly into three groups. Group A: 10 samples were irradiated with 1.06 W Er,Cr:YSGG laser, 50 Hz, 50 μs pulse duration, 60% water and 30% air pressure according to the methodology of Ramalho et al. and Esteves-Oliveira et al. 25,26 Laser irradiation implemented as one cycle comprised three irradiations of 10 sec – separated by 5 sec break in between – resulting in a total irradiation time of 30 sec. Group B: 10 samples were irradiated in three cycles comprising nine irradiations of 10 sec according to the methodology of Al-Karadaghi et al. 27 In cycle no.1, the specimens were irradiated with Er,Cr:YSGG laser with the same power settings as in group A. For cycle nos. 2 and 3, the irradiation was composed of cycle 1 settings simultaneously with a 940 nm diode laser Pave = 0.51 W in pulsed mode. Pulse widths of 4 and 10 ms, which are equivalent to duty cycles of 20% and 50% were used for the second and third cycles respectively. The total irradiation time was 90 sec for group B (Table 1). Control group (Co): the remaining five samples of each thickness were treated in the same way as in groups A and B, except for the laser irradiation, and served as a positive control (no treatment).
The slices were irradiated from the opposite to the bacterial inoculation side. This indirect irradiation protocol was preferred to investigate the influence of dentin thickness on bactericidal efficiency of the dual wavelength laser. In order to simulate the irradiation inside the root canal, the slices were irradiated in close contact with a scanning pattern of 1 mm/sec, and a 5 degree incident angulation was maintained between the fiber tip and the dentin slice.
Bacteriological analysis
The inoculated dentin slices, from both the irradiated and control groups, were placed individually into a sterile plastic PCR tube (Eppendorf Vertrieb Deutschland GmbH, Wesseling-Berzdorf, Germany) containing 1 mL of a physiological salt solution (0.9% NaCl). In general, the duration between inoculation with bacteria and resuspension to grow survivors was <2 h, and all samples were kept on ice to avoid unintended growth or death of the test strain. In order to separate the surviving bacteria from dentin slices, the tubes were vortexed for 1 min. Afterward, the bacterial suspension was serially diluted (log 10 steps). Only the last three suspensions where growth could be detected were used for calculation of surviving bacteria or as control. Of these three suspensions, 20 μL were plated onto Columbia-Agar plates. The plates were then incubated overnight at 37°C in an atmosphere of 10% CO2. After this incubation period, E. faecalis CFU were counted and analyzed. Because the data were not normally distributed, comparisons of CFU values among groups were analyzed by nonparametric Kruskal–Wallis and post-hoc Dunnett tests. p Values of <0.05 were considered as statistically significant. Statistical analysis was performed by SPSS Statistics 20 (IBM Corp., Armonk, NY).
Results
The results of E. faecalis reduction in CFU/mL and log kills are presented in Table 2. For the fidelity of the experiment, the log kill values of control group (because of the natural dying of bacteria) were further subtracted from the corresponding log kill of both laser treatment groups to present the effective log kill.
Indicates significant difference form control group.
Indicates significant difference in laser groups.
CFU, colony-forming units.
The number of bacteria recovered after laser irradiation reduced to almost comparable values for the Er,Cr:YSGG laser group and the dual wavelength laser group in 500 μm thick dentin slices (Fig. 1). As the dentin slice thickness was increased to 1000 μm, one could see a decrease in the bacterial log kill of the Er,Cr:YSGG laser group to an average number of log-steps of 2.1, leaving ∼2.7 × 104 CFU/mL resuspension solution (0.9% NaCl) of survivors. However, when the same slice thicknesses were irradiated with the dual wavelength laser, the decrease in the bacterial load was as high as 3.2 log-steps, reducing the number of survivors to 0.47 × 104 CFU/mL. Thus, a reasonable high bacterial reduction could be observed in all three dentin thicknesses (including 1000 μm) in the dual wavelength laser treatment group.
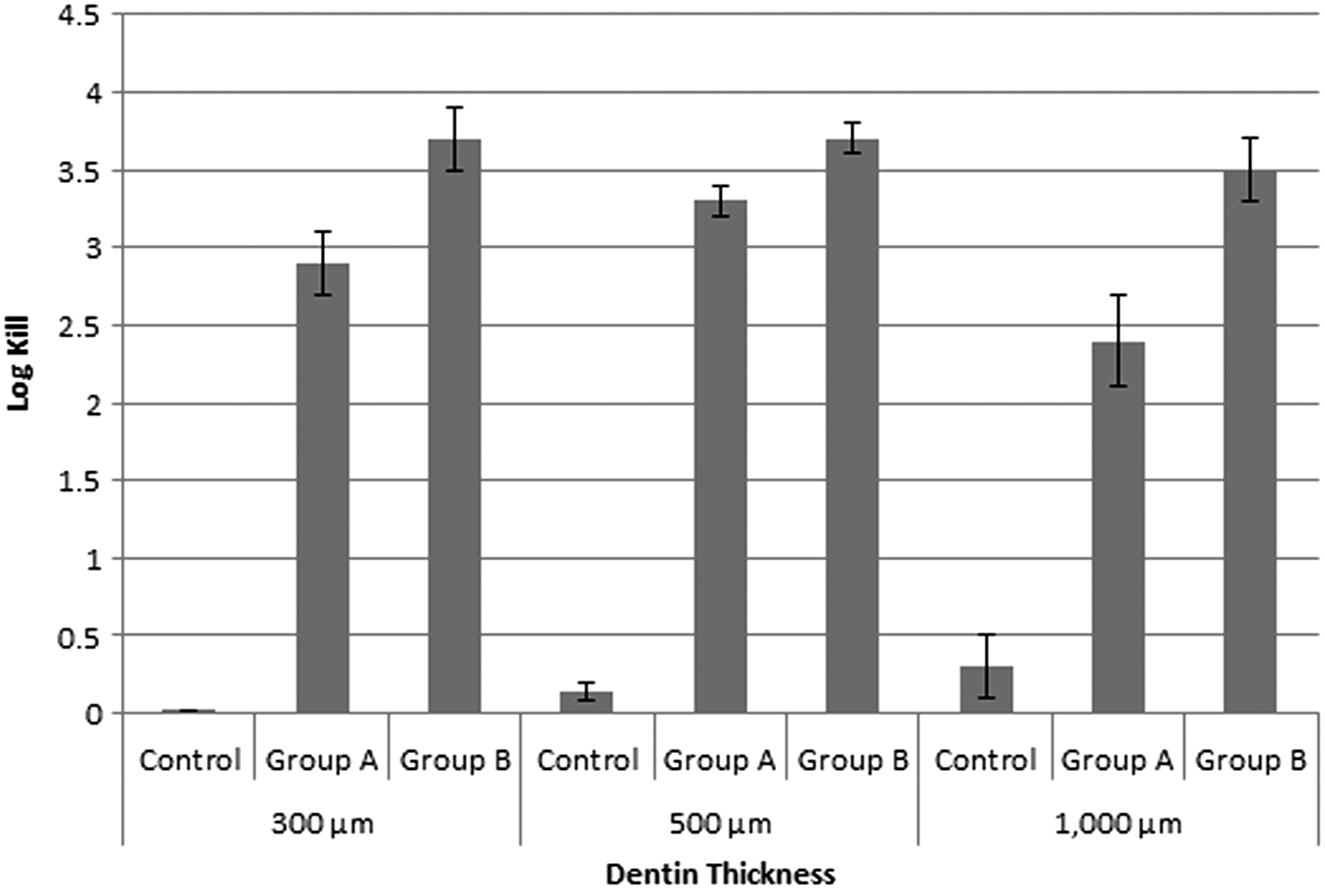
The average log kill and standard deviation of the 300, 500, and 1000 μm dentin slices. In group A, samples were irradiated with 1.06 W of Er,Cr:YSGG laser. In group B, samples were irradiated with 1.06 W of Er,Cr:YSGG laser and 0.51 W of diode laser simultaneously.
There were statistical differences between group A and group B compared with the control group over all dentin thicknesses, with p < 0.001. The results showed that significantly more viable bacteria (less reduction) were found in group A than in group B in 300 and 1000 μm dentin slices, with p < 0.01. However, a statistical difference was not found between group A and group B in 500 μm dentin slices. There were no statistical differences in group B bacterial counts over the three selected dentin thicknesses (p = 0.467), whereas the bacterial counts in group A were significantly higher in 1000 μm thick dentin slices than in 300 and 500 μm thick dentin slices (p < 0.01).
Discussion
A root canal system infection is a mixed infection of gram-negative and gram-positive bacteria. 28 The three-dimensional tubular network is usually permeated by these bacteria, forming a focus for the potential reinfection of endodontically treated teeth. 29
The results of this study showed that the dual wavelength laser has a greater bacterial reduction potential for all of the tested dentin slice thicknesses than the Er,Cr:YSGG laser alone. This reduction was significant in the 1000 μm dentin slices.
E. faecalis, which is a facultative anaerobic, gram-positive bacterium, was chosen in this study because of the reported tolerance to high temperature, physical stress, and chemobiomechanical preparation of the root canal system. 30 The presence of E. faecalis has been related to failure of endodontic treatment that has been reported in 20–23% of patients 1 year after treatment. 7,31
The major factor responsible for the long-term failure and therapy resistance in endodontics is the discrepancy in the penetration depth of microorganisms and chemical solutions. 31 Because of surface tension, the bactericidal irrigants possess an approximately one order lower penetration ability than microorganisms. 32
In many previous studies, the bacterial suspension was inoculated directly inside the root canal, and the irradiation by the laser fiber tip was in direct contact with the contaminated dentin. Our present study was designed to investigate the penetration depth ability of the dual wavelength laser by subjecting dentin slices of 300, 500, and 1000 μm thickness, and by irradiation of the opposite area of bacterial inoculation, thus at a distance of 300, 500, and 1000 μm from the bacteria. This method was applied in the same way in studies conducted by Klinke et al., 13 Gutknecht et al., 33 and Franzen et al. 3
Kakoli et al. 34 concluded that the depth of bacterial invasion was strongly dependent upon the patient age. Bacterial spread inside dentinal tubules increases from 360 μm in an older patient group to 420 μm in patients 18–25 years old. This could explain the differences in bacterial penetration depth. Hence the relative size between the bacteria and dentin tubules governs the depth of bacterial invasion. To exclude such variations, freshly extracted bovine teeth were used in our study. These teeth came from bovine of the same age and were, therefore, evenly developed according to age. Also, they showed a similar morphological composition to human teeth. 35
Gutknecht et al. reported a bacterial reduction of 86% when dentin slices of 500 μm thickness were irradiated with 980 nm at an output power of 2.8 W in CW mode. The delivery was via a 200 μm quartz fiber. This wavelength shows higher absorption coefficient in water than 940 and 1046 nm, yielding a lower penetration depth. 22 A bacterial reduction to an average of 99.91% was achieved by direct irradiation of extracted human teeth with 1.5 W and 15 Hz of Nd:YAG laser, 16 whereas a comparable result of 99.96% (3.2 effective log kill) was achieved in our study by indirect laser irradiation, which was given by the specific thickness of the dentin slices, to 1 mm dentin slices by the dual wavelength laser. 16
Franzen et al. 3 evaluated the decontamination effect of Er,Cr:YSGG laser with an average power of 0.25 W and 20 Hz delivered through 200 μm fibre on E. faecalis. After 40 sec irradiation time, a bacterial reduction of 59% was achieved. A significant difference between the Er,Cr:YSGG laser group and the control group in 1 mm thick dentin was not observed. In the same way, Schoop et al. 18 reported a bacterial reduction of approximately two log-steps compared with the control group using an Er,Cr:YSGG laser and a diode laser adjusted to 1.5 W and 20 Hz and 15 Hz for the two wavelengths, respectively, without water spray.
On the other hand, Castelo-Baz et al. used a 940 nm diode laser with power settings of 3.5 W and 50 ms pulse duration against mature biofilms of E. faecalis. The prepared root samples were irradiated for 60 sec. These authors postulated a superior bactericidal effect during combination of an irrigant solution with laser radiation than for canals disinfected with laser alone. 21 Comparable results were obtained by Preethee et al. 36 The reason behind these results was mainly the cavitational effect arising from combining an irrigant solution with laser irradiation. The rapid expansion and implosion of water vapor bubbles leads to high velocity water jets. This process results in the formation of pressure waves characterized by rapid change in pressure. Forced collapses of bubbles cause implosions that impact on surfaces, causing shear forces, and remove smear layer and debris. Such an effect could potentially rupture the bacterial cell walls. 20,37
Additionally, the high water content inside the bacteria 38 favors the absorption of Er,Cr:YSGG laser resulting from the high absorption coefficient, which is in the order of 5000 cm−1. The laser destroys E. faecalis when energy is absorbed into the volume of the bacterium. That could explain the high bacterial reduction observed in both laser groups over 300 and 500 μm thick dentin slices.
In our study, the combination of both Er,Cr:YSGG laser and 940 nm diode laser in the dual wavelength laser group showed a superior bactericidal action. In a recent study published by Al-Karadaghi et al., 27 a distinctive removal of smear layer was observed in root canals irradiated with the same power settings of the dual wavelength laser. This would explain the high bacterial reduction in the dual wavelength laser group. In addition, removal of the smear layer by laser irradiation will enhance the adaptation of root canal sealers. 39 Moreover, increasing the irradiation time from 30 sec in group A to 90 sec in group B allowed greater energy deposition and light transmission through dentinal tubules, which aggravated its bactericidal action. This is in agreement with Gordon et al., 40 who reported a decrease in the bacterial load when laser irradiation duration or power increased.
An RFT delivers laser energy in a unique pattern that could ensure a more homogeneous removal of smear layer compared with bare end fibers. Schoop et al. 24 reported a decisive disinfectant effect of Er,Cr:YSGG laser at a power setting 0.9 W and a repetition rate of 20 Hz delivered through RFT laser tips. However, EDTA was not used to remove the smear layer formed during the biomechanical preparation of roots to size ISO 70#. The bacterial permeation inside dentinal tubules could be negatively influenced. In addition, a direct irradiation was performed, resulting in direct contact of the laser fiber with the bacteria. Contrary to this, in the present study, a high percentage of bacterial reduction was obtained, although bacterial irradiation was performed indirectly and the smear layer was removed by EDTA.
Conclusions
According to the results of the present in vitro study, simultaneous irradiation with the 1.06 and 0.5 W output powers of Er,Cr:YSGG and 940 nm diode lasers, respectively, in the dual wavelength laser system obtained a significantly higher bactericidal effect on E. faecalis than did Er,Cr:YSGG laser alone. This reduction reached 1000 μm depth of dentin. Clinical studies are necessary to confirm the results and to investigate the efficiency of these wavelengths combination under in vivo conditions.
Footnotes
Acknowledgments
The authors thank Beate Melzer-Krick and Patricia Buttler-Bucher from the Department of Conservative Dentistry, RWTH University Hospital Aachen, for technical support.
Author Disclosure Statement
No competing financial interests exist.