
Abstract
Introduction
T
Various lasers (i.e., CO2, ND:YAG, diode, and also Er:YAG) have been introduced for the treatment of oral mucosal diseases, and their applications in dental clinics have become a topic of much interest. Among them, the Er:YAG laser system possesses suitable characteristics for hard and oral soft tissue ablation; because of its elevated absorption in water, an effective ablation with a very thin surface interaction occurs on the irradiated tissues without any major thermal damage to the irradiated and surrounding tissues. 2 Specifically, its use in performing oral biopsies has been described. 3 It has also previously reported that Er:YAG laser minimizes postoperative pain and accelerates healing in oral surgery. 4 –6 Moreover, even if principally designed for hard tissues, Er:YAG could be able to provide respectable cutting and coagulation effects also on soft tissues; definite parameters have to be outlined in order to achieve the chosen effect. Reduced or absent water spray, defocused light beam, local anesthesia, and the most effective use of long pulses are approaches to attain finest coagulation and bleeding control. 7
The aim of this randomized controlled study was to evaluate possible differences between the use of Er:YAG laser and traditional scalpel in patients undergoing conventional removal of nondysplastic white oral lesions. The null hypothesis was that there would be no difference between the Er:YAG laser and the traditional scalpel only in the immediate postoperative period.
The present trial is reported according to the Consolidated Standards of Reporting Trials (CONSORT) statement for improving the quality of reports of randomized controlled trials (
Materials and Methods
Study population
Consecutive Caucasian patients, attending the Oral Medicine Section of the Department of Surgical Sciences, Turin Hospital, Italy, from September 2008 and June 2010, were selected for the present study. Patients were referred for histological determination of oral white patches.
Patients were clinically evaluated by a trained group of oral healthcare providers (P.G.A., R.B.), who recorded the clinical aspect of the lesions, size, and sites of oral involvement. The size of the lesions was divided into three categories: <0.5 cm, between 0.5 and 1 cm, and >1 cm in diameter. Considering the site of oral involvement, five zones have been listed: gingiva, tongue, buccal mucosa, palate, and floor of the mouth.
A detailed medical history was taken that included pregnancy, breastfeeding, smoking habits, systemic diseases, systemic symptoms of malignancy, medications used, and level of education [primary (5 years of school), upper secondary (13 years of school), or university].
A preoperative biopsy was performed first. After this, the inclusion and exclusion criteria were evaluated as follows. Inclusion criteria were: (1) age >18 years; (2) American Society of Anesthesiology physical status classification class I (normally healthy patient) 8 ; and (3) oral mucosal lesion to be completely removed. Exclusion criteria were: (1) presence of histological signs of dysplasia; (2) inability to understand oral and written instructions; (3) pregnant or breast-feeding women; or (4) previous diagnosis or oral squamous cell carcinoma.
All patients were informed about the surgical procedures, postoperative follow-ups, and potential complications, and informed consent was obtained before surgery. The study was conducted in line with the principles of the Helsinki Declaration of 1975, as revised in 2000, and accepted by the Main Board of the CIR-Dental School, University of Turin.
Two months after histological diagnosis, each patient underwent the surgical removal of the biopsied lesion with standardized techniques. An experienced oral surgeon (R.B.) performed all procedures.
Surgical procedures
Patients were randomly divided into two groups. Allocation to treatment arms was performed using sequentially numbered randomization table. RANCODE (version 3.6) was used to generate the randomization sequence. The first group of patients underwent surgical excision of the lesion with traditional scalpel, (GROUP A_TS) whereas the second group of patients received an ablative session with Er:YAG laser (GROUP B_L).
Local anaesthesia was achieved by infiltration around the lesions using a solution of 4% articaine hydrochloride and epinephrine 1:100.000.
In those cases in which resection was performed with the scalpel, a number 15 blade, mounted in a number 3 handle, was used. An elliptic incision was made to fully enucleate the lesion along with the overlying mucosa. The wound was sutured with interrupted sutures using silk 4.0 (Perma-Hand®, Ethicon, NJ).
In the laser group, a Fidelis plus3™ Er:YAG laser (λ = 2.940 nm), with a R02-C handpiece, was used (Fotona™, Ljubliana, Slovenja). The device was used according to the manufacturer's instructions using an ablative modality: 1.5 W power, 150 mJ pulse energy, 10 Hz frequency, 500 μs pulse duration, and 0.9 mm spot size. In each session, the laser used was not in contact with the tissues, with a probe distance of ∼2 mm from the oral mucosa. Using the laser there was no need of suturing.
Postoperative assessment
The surgical time was recorded, as data relating to surgery session's difficulty.
After surgical procedures, patients were given standard postoperative instructions and standard anti-inflammatory therapy (nimesulide 100 mg tablet) to be taken if required. A cold semiliquid diet for the 1st day was suggested, and normal oral hygiene procedures were re-established after 3 days; moreover, three times daily for 1 week, patients, to clean the postoperative wound, had to use 0.20% chlorhexidine mouth rinse for 1 min.
Patients were asked to complete three different forms after surgery. The first one, to be completed at day 6, was the Italian version of the oral health related quality of life questionnaire that was measured by the Oral Health Impact Profile-14 (OHIP-14). 9 It consisted of 14 items and assessed the frequency of problems with pain, eating, speaking, self-esteem, functional status, and psychological well-being. The response set was a five-point scale from “Very often” (score of 4) to “Never” (score of 0). A second test [Quality of Life (QOL)], to be completed at day 6, was also used to assess the quality of life after surgery. This test aimed to measure, through five items (work efficiency, social activities, appetite, depression, and anxiety), how the surgical treatment might have influenced the daily activities of the patients; the response set was a five-point scale from 0 to 4.7. Finally, patients were asked to detail the pain suffered; the symptom score was obtained using a visual analogue scale (VAS). The VAS consisted of a 10 cm horizontal line marked 0 ( = no pain) to 10 ( = most severe pain ever experienced). Patients were requested to mark the scale, late in the evening, at day 3 after surgery. Moreover, they had to record the number of analgesics taken during the 1st week postsurgery (e.g., one analgesic consisted of an oral dose of 100 mg of nimesulide).
These forms were collected on the 7th day after surgery (when the sutures were removed) by the same independent examiner, unrelated to the study.
Statistical analysis
Sample size was challenging to estimate, based on the lack of any previously reported changes in patients treated with this protocol; the power of the study was then calculated for a range of values at 0.95 confidence, for a 170 × 2 sample size (with software PASS13). Each group had to be composed of at least 170 lesions.
The primary outcomes of the study were reported quality of life and postoperative pain. Secondary outcome was the duration of surgery. Describing general information, data were reported as means and standard deviation (SD). Descriptive analyses were performed using the t test or the Mann–Whitney test for continuous variables and the χ2 test or Fischer exact test for categorical variables when indicated. Analysis was stratified by gender, age, smoking habits, size of lesions, and duration of surgery. Statistical significance level was set at 0.05. SPSS (SPSS for Windows, version 19, SPSS Inc, Chicago, IL) statistical software was utilized.
Results
Initially, 371 patients were screened; 22 of these were not included because presenting exclusion criteria (15 had a dysplastic lesion, 3 had a neoplastic lesion, and 2 were found to be pregnant after first biopsy). Five patients refused to be part of this study. Figure 1 shows the flow diagram for patients' enrolment and selection. No deviation from the operative protocol occurred.

The Consolidated Standards of Reporting Trials (CONSORT) explanatory flow chart.
A total of 344 patients took part in the study of which 198 were women (57.5%); 394 lesions were treated. For female subjects, the mean age at presentation was 61.7 years (±12.8), for male subjects it was 58.2 years (±12.8).
Two hundred and twenty-one lesions (56.1%) underwent surgery with traditional scalpel (Fig. 2), whereas 173 (43.9%) underwent laser surgery (Fig. 3). No statistical differences were found between the two groups regarding gender, age, and smoking habits (Table 1) and degree of education. Differences in outcome measures between the two groups are reported in Table 1: significant differences were found if considering the surgical time, VAS, and QOL and OHIP-14 questionnaires. Regarding those data, the Er:YAG laser appeared to be faster and less painful than traditional scalpel (p < 0.05).
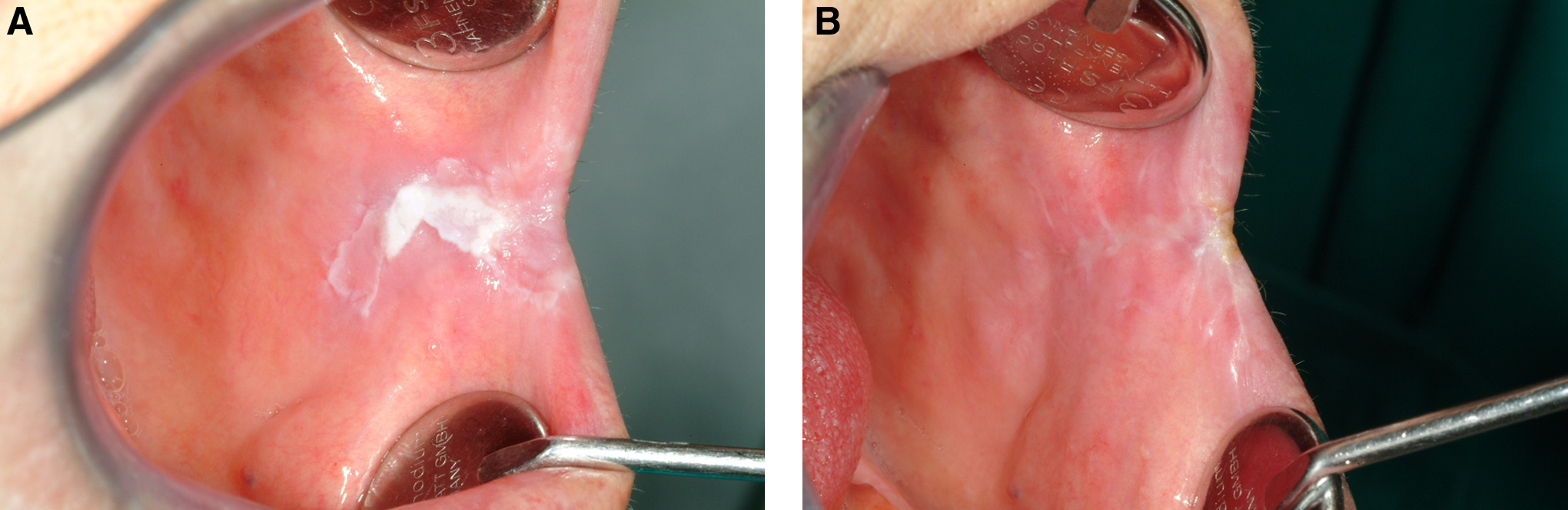
A white lesion of the left buccal mucosa.
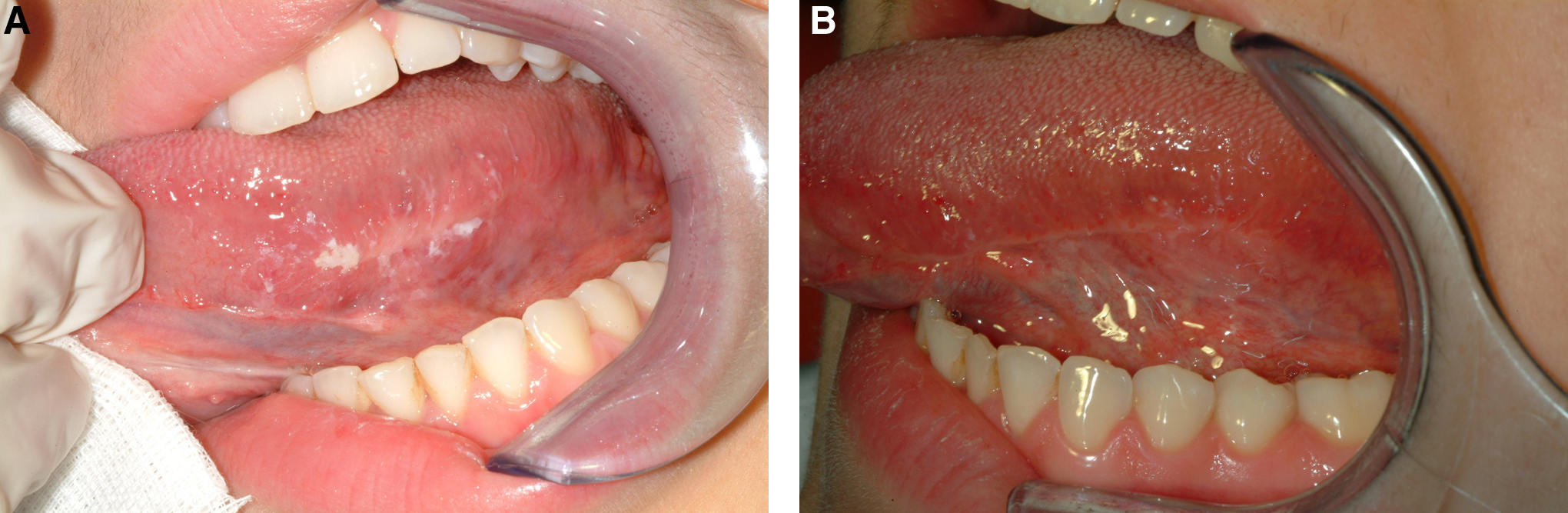
A white lesion of the left lateral border of the tongue.
t test.
VAS, visual analogue scale; OHIP-14, Oral Health Impact Profile-14.
If considering the smallest lesions (93 were <0.5 cm), no statistical differences were noticed in any of the outcome measures detailed (data not shown). For bigger lesions (211 were between 0.5 and 1 cm, and 90 were >1 cm), all the reported outcomes differed in the two groups (Tables 2 and 3), the laser technique being the most favorable for the treated patients; also, the mean painkiller consumption was statistically different.
t test.
VAS, visual analogue scale; OHIP-14, Oral Health Impact Profile-14.
t test.
VAS, visual analogue scale; OHIP-14, Oral Health Impact Profile-14.
The correlation between the analgesic consumption and VAS score was found to be statistically correlated (Pearson correlation = 0.508; p < 0.05).
Specific results, considering the sites of oral involvement, are reported in Table 4. The Er:YAG laser appeared to be less painful and was well accepted by patients when treated for gingival and palatal lesions (p < 0.05).
t test.
VAS, visual analogue scale; OHIP-14, Oral Health Impact Profile-14.
Discussion
Significant advances in laser technology have been made since the advent of laser treatment of oral diseases, and today a great variety of different systems can be used in this field. 10 Laser surgery has been shown to exhibit several advantages over scalpel for many oral procedures, including hemostasis, decreased scarring, and the ability to perform certain procedures without anesthesia.
The present report identifies significant difference in the immediate postoperative surgical period between the two treatments, meaning that the Er:YAG laser seemed to be less painful than traditional scalpel; patients also seemed to prefer laser, especially if considering bigger lesions occurring in the gingiva or in the palate. Usually, keratinized areas, if compared with other oral sites, are less painful in terms of postoperative recovery after surgery. 11 It has been suggested that the mechanical pain thresholds in orofacial areas might be influenced by the density of free nerve endings, the degree of keratinization, and tissue thickness. The palatal zone is typically less sensitive than the tongue or floor of the mouth, but cold knife excision provided worse healing than laser in keratinized tissues; for this reason, it appear reasonable to use laser in such zones.
In oral surgery, a laser system with lesser application to soft tissues is the Er:YAG laser, which produces prompt healing as a result of the restricted thermal effect generated. An inconvenience, however, is that the surgical field is not free of blood (unlike with the CO2 laser); consequently, upon concluding surgery, compression of the treatment zone is required to ensure adequate hemostasis. 12 However, in our experience, it is sufficient to wait for several minutes, and a partial clotting will be obtained; for this reason, sometimes sutures could be avoided, leading to a decreased surgical time.
Many studies have analyzed the possible surgical properties of Er:YAG lasers in dentistry. It has been recently reported that Er:YAG could provide good cutting and coagulation effects, specifically on oral soft tissues; however, specific parameters have to be defined in order to obtain the optimal desired effects (e.g., water spray, defocused light beam, and the use of long pulses). 13 Moreover, Er:YAG laser may be routinely used in oral surgery, because of its minimal damage to the epithelial tissue, its low inflammatory reaction, its quicker healing process, and its lower risk of scarring. 14,15
The CO2 laser is the most studied device for the surgical treatment of leukoplakia, whereas few authors had used the erbium. Although the erbium laser is the treatment of choice for hard tissues, its water absorption makes it effective also in the treatment of soft tissue, especially based on the ability to remove thin layers of tissue and the poor thermal damage in the surrounding tissues, 10 which also allows the treatment of lesions located in delicate areas such as, for example, the floor of the mouth and the lingual pelvis.
To date, not many data are available about the quality of life reported by patients treated with this erbium laser. Usually, after any surgical procedure, quality of life can be modified. Oral health-related quality of life characterizes a person's perception of how oral health influences an individual's quality of life and overall well-being. Although the type of surgery reported in this article is not life threatening, it can affect not only the capacity to eat and communicate but also interpersonal relationships, daily activities, and, therefore, “quality of life.” 16 The results of our study indicated that the Er:YAG laser could be a well-accepted modality of treatment for oral lesions.
Other types of laser have been previously studied for the same purpose, with dissimilar results. Very recently, it has been reported that CO2 laser supersedes conventional scalpel in terms of better intraoperative and reduced scarring; however, postoperative pain and swelling after laser excision did not show any significant difference from those after the use of scalpel. 17 On the other hand, it has been also reported that the CO2 laser could cause only minimal pain and swelling, therefore suggesting that it may be an alternative method to scalpel in treating oral leukoplakia. 18
Acute postoperative pain following oral mucosal surgery is primarily a consequence of inflammation caused by tissue injury; pain is usually greater 48–72 h after surgery, 16 and in our sample, laser seemed to reduce the reported discomfort 3 days after intervention.
This report has, however, three main limitations. The main limitation is the lack of independent and blinded evaluation of the outcome measures. Moreover, patients were also not blinded; however, this is because we did not use a placebo. Finally, considering the simple size without the dropouts, the number of patients at the end of the study was less than those needed.
Conclusions
In conclusion, these results, although not categorical, are a step forward for enhanced management of the treatment of nondysplastic oral lesions; however, it would be interesting to know if this would be true with a greater number of patients or in a different clinical setting.
Footnotes
Author Disclosure Statement
No competing financial interests exist.