
Abstract
Introduction
V
Management of vascular malformation may vary, according to their location and clinical picture, and can include treatment with corticosteroids, beta-blockers, cryotherapy, laser, embolization, electrodessication, and surgery. 4,5
The use of lasers in the treatment of skin vascular lesions was introduced in the 1960s by Goldman and colleagues 6 and gained more popularity with the diffusion of the selective photothermolysis theory by Anderson and Parrish in 1985. 7 The latter authors hypothesized that specific molecules present in the tissues called chromophores, such as deoxyhemoglobin, oxyhemoglobin, and melanin, can selectively absorb exact light wavelengths. These molecules transform the light energy into thermal energy after their absorption. Therefore, chromophores can be selectively damaged or destroyed by the specific absorption of an appropriate wavelength. This subsequently led to a more thorough understanding of laser therapy (and its related treatments by non-coherent light sources); therefore, it is now considered the gold standard in the treatment of the majority of vascular lesions.
It has long been established that vascular malformations can be treated effectively with a variety of vascular-selective lasers. Flashlamp-pumped pulsed dye laser (PDL) has been the first laser based on the selective photothermolysis theory, which has been manufactured for the treatment of vascular lesions. However, the short penetration of the laser light (no more than 0.2 mm below the dermo-epidermal junction) required a high fluence to target deeper vascular lesions, producing very high complication rates. 8 The short pulse duration causes vessel disruption, which can result in a cosmetically unpleasant and long-lasting, post-treatment purpura. 9 In addition, many lesions that respond well to an initial treatment with PDL may reach a response plateau, becoming unresponsive to further PDL treatments, a phenomenon known as “treatment resistance.” 10 Second-generation PDL treatments were introduced to decrease the rate of complications, but these devices still remain difficult to maintain and service. 11 The dye and the lamp have to be checked within 1 year and have to be substituted if necessary. The device has to be switched on at least once a day to circulate the dye within the machine for the correct function. Due to these limitations, PDL has now been replaced by safer, more predictable, and more deeply penetrating light sources such as the 1064-nm Nd:YAG laser and the novel intense pulsed light (IPL) devices. 10,12 Although treatment with the long-pulsed Nd:YAG can achieve satisfactory outcomes, it can be, however, complicated by pain, which often requires management with cooling and topical anesthesia. Another common side effect of the 1064-nm Nd:YAG laser is the presence of hyperpigmentation, which can occur even in patients with light phototypes. Hyperpigmentation usually resolves with time, whereas hypopigmentation and scars are uncommon. 10
Novel IPL devices have the advantage of producing variable pulse durations along with multiple split light pulses, releasing the heat to different diameters of vessels. An additional advantage of the IPL is its capacity to emit multiple wavelengths that potentially target the full range of the hemoglobin absorption peaks, leading to destruction of both superficial and deep components of the vascular lesion. 13
Here, we present our experience with an optimized pulsed light source (MaxG™; Palomar Medical Technologies, Inc., Burlington, MA). We describe the technique and evaluate the clinical outcomes in patients treated with this method. To our knowledge, the use of MaxG represents a novel method for the treatment of vascular anomalies.
Methods
We conducted a prospective study to evaluate the outcomes and clinical efficacy of the MaxG optimized pulsed light source. Patients were selected by following clinical evaluation and clinical records that were obtained through the Department of Plastic and Reconstructive Surgery, University of Rome “Tor Vergata.” Candidates who met the inclusion criteria were informed of the purpose of the study, the required procedures and assessments, the duration of the study, and the potential risks and benefits of the proposed treatment method. The local ethics committee approved the proposed protocol of the study, and it has, therefore, been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. All patients read and signed written informed consent forms. The study included 30 patients aged between 18 and 65 years. We recruited patients for the period February 2012 to July 2013, and the study was completed in July 2014. The inclusion criteria for recruitment were skin phototypes of I–III, vascular lesions of the face, including hemangiomas, PWS, ectasias, telangiectasias, and dilated facial veins, and painful, bleeding, disfiguring lesions associated with psychological distress. Patients with unsuccessful previous treatments were also included in the study.
Clinical efficacy was evaluated subjectively by patients (degree of pain and cosmetic improvement) using a questionnaire and objectively (size and discoloration of the malformation) by an independent physician evaluator using a quartile grading scale. The results were graded as excellent when there was 75–100% improvement, good if there was 50–75% improvement, and fair if there was 25–50% improvement. The efficacy was evaluated for different patient groups, depending on the kind of vascular malformation. Any adverse effects from treatment were also recorded.
All data were initially entered into an EXCEL database (Microsoft, Redmond, Washington), and the analysis was performed using the Statistical Package for the Social Sciences Windows, version 15.0 (SPSS, Chicago, IL). Descriptive statistics consisted of the mean ± standard deviation. A comparison of continuous variables was performed using one-way ANOVA with multiple comparisons by Bonferroni test. A p value <0.05 was considered statistically significant.
IPL treatment
The laser used was the StarLux 300 platform with the IPL handpiece MaxG (Palomar Medical Technologies, Inc.). Power settings were set in the range of 36–56 J/cm2, with pulse durations between 10 and 42 msec. The settings for all treatments were defined taking in consideration the authors' experience, suggestions of the manufacturer, and size and depth of the vessels and were adjusted according to the immediate clinical response of the treated area. Treatment parameters were modulated based on the depth and color of each lesion. The pulse width was gradually augmented as the fluence energy increased appropriately.
The target treatment area was defined by a 10 by 15 mm sapphire optical window with uniform output fluence and selectable temperature. For greater safety, the temperature of the contact sapphire window on the handpiece could be adjusted to provide cooling. No topical or local anesthesia was used. Patients received a series from three up to a maximum of six sessions. Treatment was repeated at an interval of a minimum of 4 weeks between sessions, depending on the rate of clearance of their lesions. Patients were informed to expect some degree of erythema, swelling, and rarely minor ulceration or crusting after the procedure. Cooled ice packs were applied immediately after the treatment on the areas concerned. A corticosteroid cream Advantan 0.1% 20 g (Intendis S.p.A., Milan, Italy) was applied topically 1 h after laser therapy, and it was continued for a course of 5 days. A Stearyl glycyrrhetinate soothing cream (Neo-Tec; NeoEurope S.r.l., Rome, Italy) was used to improve skin regeneration, and a hyaluronic acid moisturizing gel (Neo-Tec; NeoEurope S.r.l.) was prescribed for daily application. In the event of postoperative crust, we recommended application of Iruxol ointment (Smith & Nephew Ltd., Hull, UK) on a twice-daily basis for 5 days. Patients were monitored daily during the first week and until healing was complete. They were seen again during follow-up 1–6 weeks postoperatively.
Results
A total of 30 patients (21 men and 9 women) with vascular lesions that presented on the face, cheek, scalp, orbital area, frontal area, lip, and nose were treated in this study. The mean age of patients was 46.3 years (range, 36–64 years). The average follow-up period was 10 months (range, 6–14 months). On a total of 30 patients, 12 patients were affected by PWS, 5 with rosacea, 4 by teleangegtasia, 3 with hemangioma, 2 with ectasia, 2 with venous lake, 1 with spider angioma, and 1 with cherry hemangioma. The location of the vascular malformations was as follows: face (12); cheek (20); frontal area (2 of 30); scalp (2 of 30); lip (2 of 30); orbital area (1 of 30); and nose (1 of 30). The range power used for PWS was 38–42 msec, 52–56 J/cm2 (average 39.8 msec, 53.6 J/cm2); for rosacea, 20–22 msec, 38–40 J/cm2 (average 20.4 msec, 38.4 J/cm2); for telangiectasia, 10–12 msec, 36–38 J/cm2 (average 10.5 msec, 37 J/cm2); for ectasias, 18–20 msec, 36–38 J/cm2 (average 19 msec, 37 J/cm2); for venous lake, 38–40 msec, 42–44 J/cm2 (average 39 msec, 43J/cm2); for spider angioma, 20 msec, 38 J/cm2; and for cherry angioma, 40 msec, 44 J/cm2.
The average number of treatments was 4.2 (range between 3 and 6). Clinical pictures of the patients are shown in Figs. 1 –4. Patients' data and treatment parameters are summarized in Table 1.

A 50-year-old man with hemangioma of the right cheek
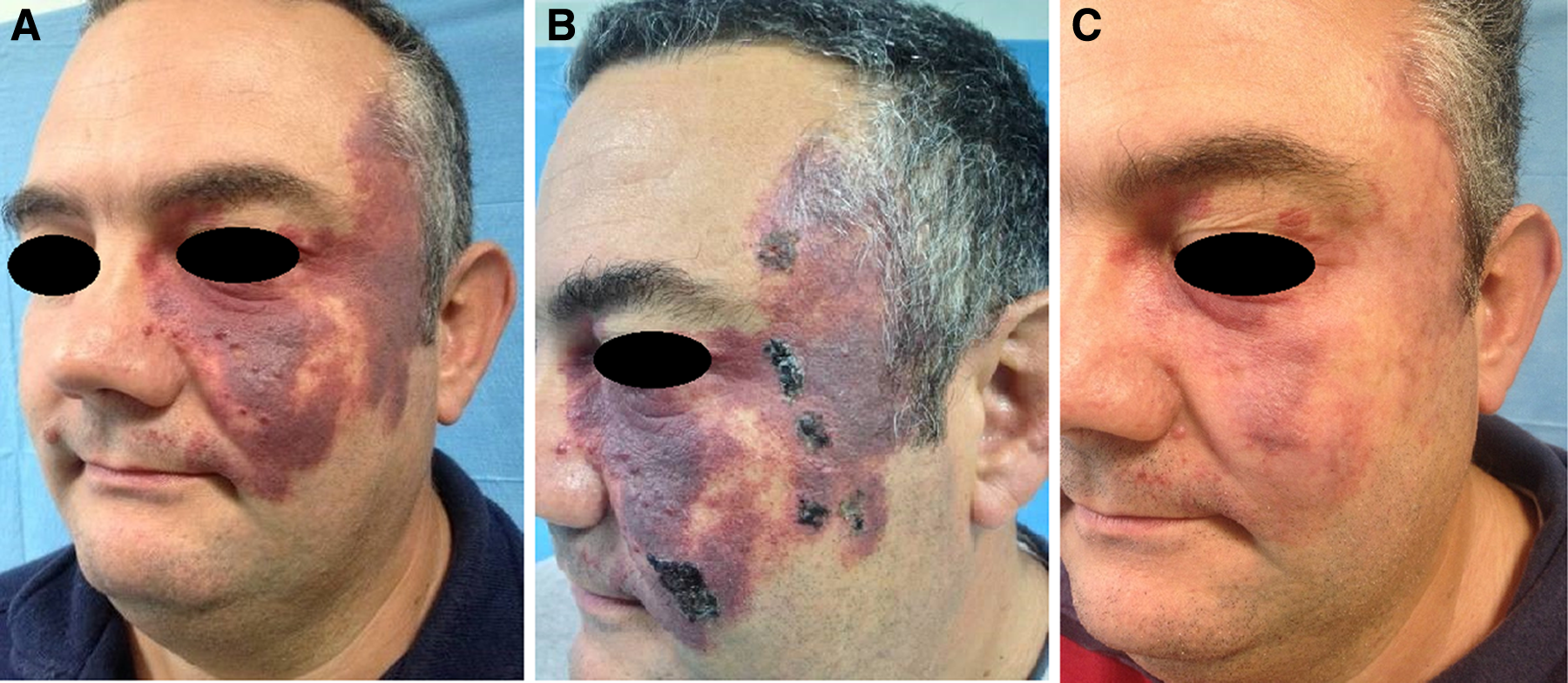
A 48-year-old man with port wine stain of the left orbital region

A 36-year-old woman with rosacea of the cheek
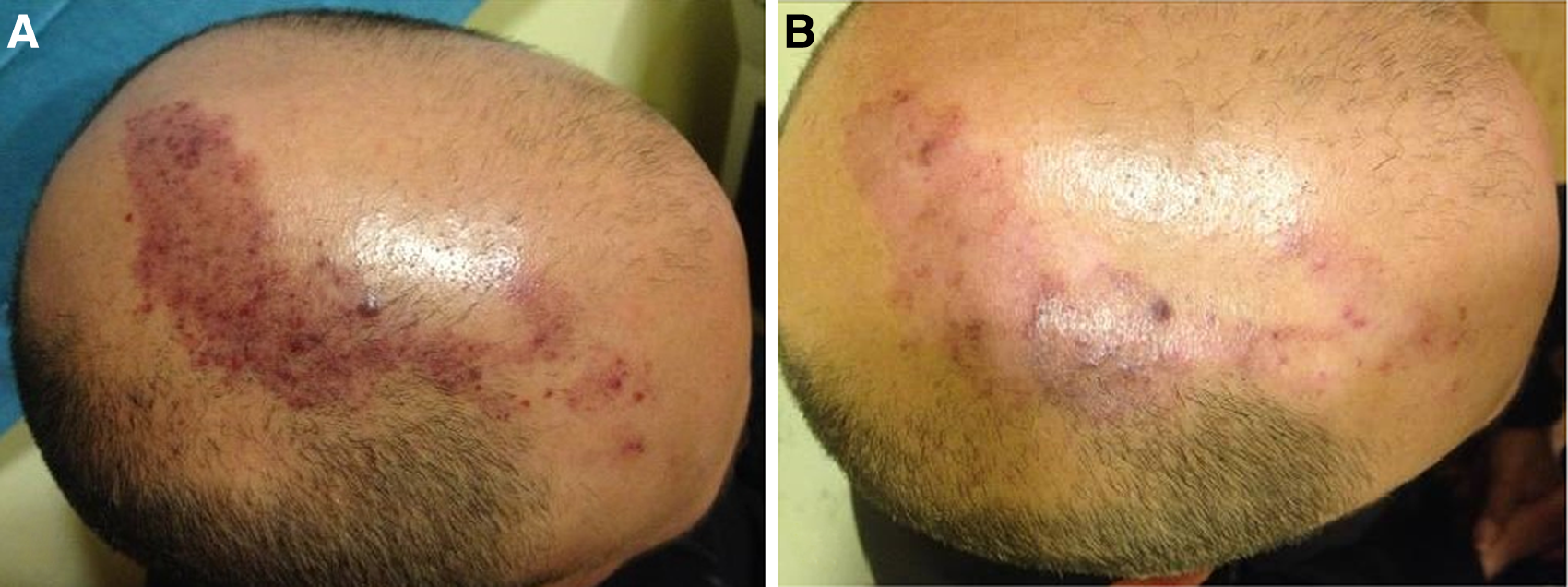
A 40-year-old man with teleangectasia of the scalp
In the objective assessment for the PWS group (12 of 30 patients), the result was 50–75, average 66.7% (±12.3%); for the rosacea group (5 of 30 patients), it was 75–100, average 85% (±13.7%) of improvement; and for the teleangectasia group (4 of 30 patients), it was 75–100, average 81.3% (±12.5%). The patients with hemangioma (3 of 30) had 66.7% (±14.4%) of improvement, the patients with ectasia (2 of 30) had 75% of improvement, the patients with venous lake (2 of 30) had 87.5% (±17.7%) of improvement, and the patients with spider angioma and cherry angioma reported 100% and 75% of positive results, respectively. The overall objective assessment had a 75% of improvement (±14.7%).
The multiple comparisons between groups 1 and 2 were p = 0.013 and p < 0.05.
In the subjective assessment of treatment, all patients tolerated the procedure well. With regards to the efficacy of the method, 75% of patients responded positively and considered their treatment as successful; the self-estimation and social appearance have been improved in 80% of cases. Patients' assessment and improvement are summarized in Table 2.
Multiple comparisons by Bonferroni test: group 1 versus group 2; p = 0.013 and p < 0.05.
SD, standard deviation.
The overall side effects rate of the laser treatment was 10% (3 of 30). One patient showed hyperpigmentation on the face, one patient reported prolonged erythema on the face, and one showed crusting on the left cheek (Fig. 2B). No skin blistering, ulceration, bleeding, hypopigmentation, or hypertrophic scarring was noted.
Discussion
Lasers have been used successfully to treat a variety of vascular lesions, including telangiectasias (rosacea, poikiloderma of civatte, and spider angioma), capillary malformation (PWS), cherry angiomas, pyogenic granuloma, venous lakes, and leg veins (spider veins of the lower extremities). 10 –16 The ultimate goal of laser treatment is to induce vessel wall damage through destruction of the hemoglobin, with minimal injury to local, unaffected tissues. Vessel destruction can occur through either photomechanical or photothermal means. When short pulse widths (or pulse durations) are performed, photomechanical damage occurs. This induces intravascular cavitation, vessel wall rupture, and hemorrhage. 7,8,10 Clinically, this can be manifested as purpura after treatment. With longer pulse widths or stuttered pulses, photothermal damage can occur. This results in gentle heating of the vessel, intravascular coagulation, and collagen contracture. Clinically, this is shown with immediate blanching or delicate darkening of the vessel, followed by consequent erythema and edema. 16 To achieve this aim, several devices were developed, including argon, Argon-pumped tunable dye, potassium-titanyl-phosphate, krypton, copper vapor, copper bromide, PDLs, Nd:YAG, and IPL. The argon laser was used globally in the 1970s. However, side effects frequently occurred, causing a high degree of non-specific thermal injury, pigmentation, and scarring, and it is now largely replaced by flashlamp-pumped PDL. 17 Levine and Geronemus 18 reported few side effects as well as hyperpigmentation, hypopigmentation, and spongiotic dermatitis in their experience using 577- and 585-nm PDL for the treatment of vascular lesions in 500 patients. Subsequently, PDLs with a 585 nm wavelength and a pulse duration of 0.45 msec were selected as the standard treatment for vascular diseases, including nevus flammeus, hemangioma, and telangiectasia. 9
The PDL can be considered the laser of choice for most vascular lesions because of its superior clinical efficacy and low risk profile. However, a current limitation of PDL devices is their inability to deliver uniform, long pulses of energy. 12 Instead, the energy is delivered over a series of very short pulses 19 that could potentially compromise skin safety and increase the risk of ablative, as opposed to the desired coagulative, damage. Another limitation of PDL devices is the use of a single, short wavelength with limited penetration not only through larger vessels but also through vessels that lie deeper in the dermis. 19,20 Therefore, PDL has the limitation of inducing purpura in a significant number of patients, with an inability to treat deeper lesions and achieve optimal results. 21 In contrast, one of the main advantages of IPL technology is the minimal postoperative purpura, which substantially reduces the recovery time. 12 Rather than inducing immediate purpura, the goal of treating vascular lesions with IPL is to raise the blood vessel temperature high enough to cause its coagulation, leading to its destruction and eventual replacement by fibrous granulation tissue. 22 Modern IPL devices provide pulse durations up to 100 msec, and handpieces such as the MaxG that can release double spectral bands can be installed: 500–670 and 870–1200 nm. Unlike PDL and IPL devices, the MaxG output power is very constant and free of high peak-power spikes. This means that the peak power is the same as the average power for every pulse, so the operator knows the energy delivered and which vessels are targeted. 19 Thanks to these features, the MaxG handpiece allows delivery of light energy to vessels over longer periods. This effect results in a gentle, uniform heating or even coagulation across the entire vessel, while reducing the risk of vessel rupture and its associated effects of purpura and hyperpigmentation. 23,24 In this study, purpura has not occurred in any of our cases. One of the side effects reported was crusting, which occurred in a patient with PWS (Fig. 2B). In this case, a high fluence with a short pulse duration (38 msec/56 J cm2) was used and led to crusting. This complication was resolved by applying a topical proteolytic enzyme ointment associated with chloramphenicol (Fig. 2C). Consequently, to decrease the risk of crusting, we decided to adjust the parameter of pulse duration to 40–42 msec and that of fluence to 52–54 J cm2. There were two more patients who reported problems of mild hyperpigmentation and prolonged erythema. These side effects were resolved within a 10 day course of topical application with corticosteroid cream, combined with soothing and moisturizing of the affected areas.
Another advantage of the MaxG handpiece is its deeper penetration of light energy into the skin, releasing less absorption with less scatter. In fact, the near-infrared, 870–1200 nm spectral band of the MaxG allows coagulation of blood vessels that are larger in diameter and/or located deeper in the skin. 25 Hemoglobin shows absorption peaks in the blue, green, and yellow bands (418, 542, and 577 nm) as well as a peak further out in the near-infrared portion of the spectrum (700–1100 nm). This explains the efficiency of the MaxG in the treatment of deep vascular lesions with the characteristics described earlier. In our experience, we found that deeper lesions, including specifically hemangiomas, ectasias, angiomas, and lake veins, are suitable for laser therapy with Max G and they have shown a significant margin of improvement after treatment.
Conclusions
Our results confirm the efficacy and safety of the novel optimized pulsed light source (MaxG) for the treatment of facial vascular lesions. Based on our experience and results, we believe this device could be considered as both an alternative monotherapy and a useful adjunctive to the already existing laser instruments and represent a beneficial addition to the repertoire of every laser specialist.
Footnotes
Author Disclosure Statement
No competing financial interests exist.