
Abstract
Introduction
T
The disruption of this tendon is considered a serious injury, because of its scarce blood supply, and it may take weeks or even months before complete cicatrization. 9 This injury generally occurs between 2 and 6 cm from its insertion in the calcaneus bone, 1 and some important alterations may occur, such as: functional complications 6 and ultrastructural, 10,11 biochemical, 5,12,13 and biomechanical 14 changes.
Many studies have been developed to better understand the processes of tissue repair and the shortening of cicatrization time for the calcaneal tendon. 3,15,16 In the rehabilitation scenario, the use of some physical agents, such as electrical stimulation, 17 therapeutic ultrasound, 3,18,19 and low-level laser therapy (LLLT) 4,7,8,20 –23 have demonstrated positive results for tissue recovery and repair.
For the development of more detailed studies on the effects of physical agents on injuries in the calcaneal tendon, it is necessary to develop an experimental model similar to intrinsic problems found in human beings. Among the main factors that may lead to injuries and make repair more difficult is poor vascularization of the central region of the calcaneal tendon, which indicates that proximal and distal regions have richer vascularization. 24
Experimental studies have been developed with different types of calcaneal tendon lesions; namely, partial injury, total rupture, and conditions varying from inflammatory to degenerative. Despite the technological improvements to diagnose vascularization and formation of new vessels in tendinopathy, there are no studies investigating the process of calcaneal tendon vascularization or determining if the tendon in rats has the same vascularization processes found in humans. Another important factor is to aid researchers and clinicians in choosing the place to apply the LLLT, because most studies in the literature have used the medial (central) part, the point with the least amount of blood vessels. This is why it has become necessary to evaluate vascularization in the proximal, medial, and distal regions of the calcaneal tendon post-LLLT irradiation in injured and uninjured tendons.
Methods
Study design
This was a primary, experimental, controlled, randomized and single-blind study.
Sample
We used 28 adult rats (Rattus norvegicus: var. albinus, Rodentia, Mammalia, of the strain Wistar), 3 month old, weighing from 280 to 320 g, obtained from the Faculdade de Ciências da Saúde—Universidade Metodista de Piracicaba (FACIS-UNIMEP) vivarium. The animals were kept individually in polypropylene cages with a 12 h light–dark cycle at a constant temperature of 22°C, and were fed with suitable ordinary feed as well as water ad libitum. Animal handling was conducted in accordance with the guidelines of the Assessment and Accreditation of Laboratory Animal Care.
Experimental design
All 28 animals were distributed randomly by computer sorting (BioStat 5.0) and divided in four groups of seven rats each.
Control group: animals did not undergo any injury or treatment. Their calcaneal tendon was removed for histological and morphometric analysis of blood vessels.
Sham group: animals underwent partial injury of the calcaneal tendon and simulated LLLT.
Group 830 nm: animals underwent calcaneal tendon injury and, after 1 min, 830 nm LLLT (GaAlAs) and irradiation at energy density of 40 J/cm2.
Group 660 nm: animals underwent calcaneal tendon injury and, after 1 min, 660 nm LLLT (AlGaInp) and irradiation at energy density of 40 J/cm2.
Calcaneal tendons of animals in sham, and LLLT 830 and 660 nm groups were excised 5 days after injury for histologic and morphometric analysis. In the sham group, the tendons were obtained from animals who did not undergo injury, in the same period.
Equipment
We used an LLLT device (DMC® - São Carlos - Brazil - Sebastião Moraes, 831 - 13562-030) of visible and infrared diode, using 830 nm (GaAlAs) and 660 nm (AlGaInp) wavelengths, power output of 60 mW for both lasers, 40 J/cm2 energy density, 1.14 J (energy), 0.028 cm2 of beam spot, and continuous wave (Table 1). Before the study, equipment was calibrated by Laser Company and radiant power was determined using digital potency analyzer Coherent LM 10 HTD. Before each application, the calibrator was adjusted by attaching the end of the laser diode, at a 90 degree angle, to the digital potency analyzer Lasercheck (Coherent, Staunton, VA) sensor, and used according to the manufacturer's recommendations.
Injury procedure
Animals were weighed and anesthetized proportionately to body mass, using an intramuscular injection of 100 mL/kg of ketamine chlorhydrate and 50 mL/kg of xylazine chlorhydrate. After anesthetic induction, the skin around the right calcaneal tendon underwent manual shaving and then, positioned in the lesion device, the injury process was performed. Traction was performed in the calcaneal region, with the ankle in dorsiflexion, and a 200 g weight was released perpendicularly from a height of 20 cm, over the animal's tendon. The fall's potential energy over the tendon was 364.9 mJ (Fig. 1).
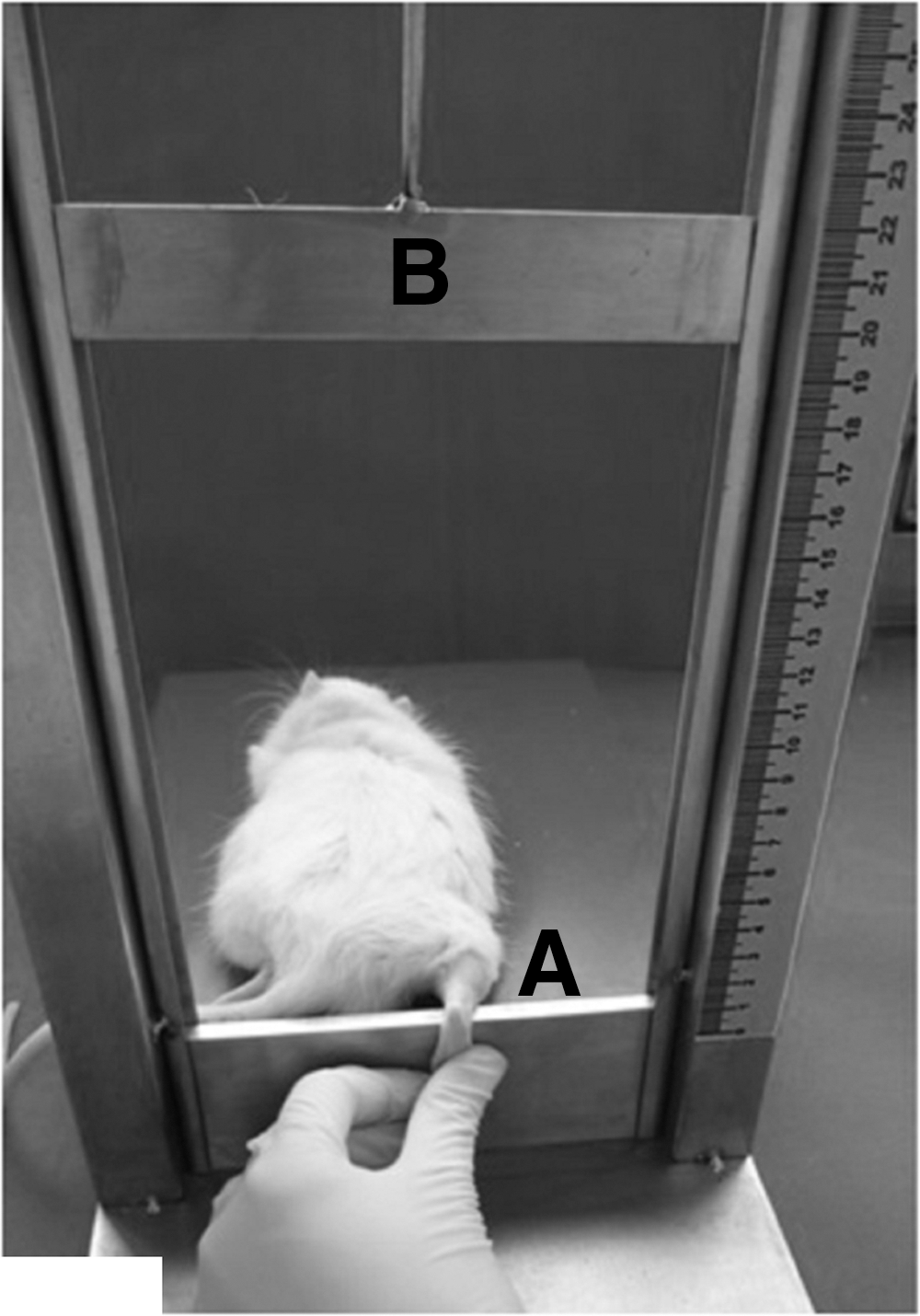
Positioning of the animal in the injury device.
After this procedure, the weight was removed and the medial part of the Achilles tendon was marked with a circle around it, using a dermographic pen, to be able to perform local laser application in the future. Then, the animal was put in its cage and observed until the end of the anesthetic effect.
LLLT procedure
LLLT applications were performed during 4 days, starting 1 min after injury, always in the afternoon. Irradiation for the sham 830 and 660 nm groups was performed using the punctual contact technique, and the probe was positioned perpendicularly to the skin. Power output was set for 60 mW for both lasers. Energy density was 40 J/cm2, total energy was 1.14 J, power density was 2.14 W/cm2, and application time was 18.6 sec.
Preparation of samples and data analysis
Animals underwent euthanasia 5 days after trauma with a high dose of anesthesia, and their tendons were removed surgically by dissection from the calcaneal insertion to the myotendinous junction.
Immediately, tendons were rinsed in a 0.9% saline solution, as a preparation for the following histological procedures.
Immediately after, tendons were rinsed in running water to be dehydrated in increasingly stronger solutions of ethylic alcohol at 70% and 90%, for 1 h in each solution. Then, tendons were subjected to six baths of 1 h each in a 100% alcohol solution.
After immersions in 100% alcohol, tendons were diafanized in 1:1 alcohol/diaphanol solution for 1 h, and then subjected to two pure xylol baths of 1 h each.
Tendons were removed from xylol and put immediately in liquid paraffin (60°C). After a few hours, this paraffin was changed to a second paraffin (Paraplast®). During the second paraffin bath, the pieces were placed in a vacuum oven and left for a 2 h period; then, the pieces were removed from the oven and put into paraffin to obtain histology blocks.
After the inclusion of tendons in paraffin blocks, their length was measured using rulers, and they were cut into three parts: the first proximal part, the second medial part, and the third distal part. All parts had equal dimensions, according to the length of each tendon. From each region, we obtained semiserial transversal cuttings using a rotary microtome. Cuttings were arranged in histology laminates, deparaffinized, and rehydrated for coloration using hematoxylin and eosin, to analyze blood vessels.
Histology analysis was performed using a reticulate ocular (Carl Zeiss® KF 10x/8, Germany), with a zoom of 40×, and a 25 μm reticulum in each quadrant; therefore, for each animal, an area of 37.500 μm2 was assessed (three reticulum areas were counted, measuring 2.500 μm2 in each cutting, and a total of five cuttings were counted for each animal).
Statistical analysis
After finishing data collection and histological slide analysis (examiner blind), we identified and sorted samples according to their groups. We used the Shapiro–Wilk normality test to check data distribution and the Levene test to check for variance homogeneity. Data were compared among groups by conducting an analysis of variance (inter- and intragroup analysis), followed by the Tukey test. Analyses were conducted using the data processing software SPSS 13.0. Significance level was 5% for all analyses mentioned.
Results
The distribution of blood vessels (V) in different parts of the calcaneal tendon (proximal – A, medial – B, distal – C), as well as fibrocyte (Fb) and collagen fibers (Col), can be found in Fig. 2.
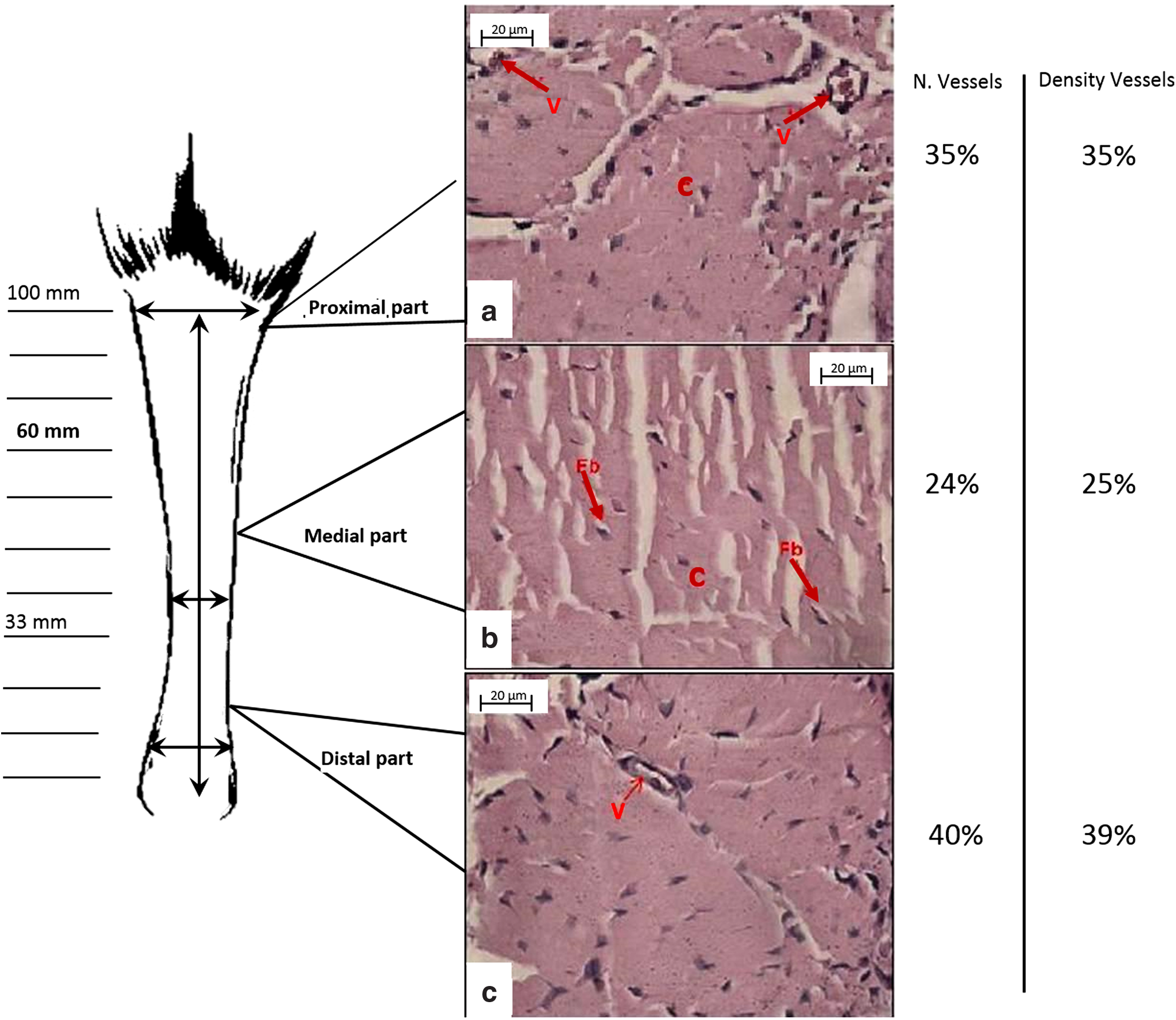
Photomicrography of the proximal, medial, and distal parts of the Achilles tendon. The number and density of vessels from each part are shown. Note the presence of blood vessels (V) in the proximal and distal part (
Results of the morphometric analysis in all experimental groups can be found in Table 2. There was no significant difference for either variable analyzed (number and density of blood vessels) between groups treated with 660 and 830 nm, nor was there any difference among treatment groups when compared with the sham group.
Statistically significant when compared with control group.
Statistically significant when compared with medial part.
When comparing all groups, one can observe that the control group showed higher values of area density and a greater number of blood vessels than the other groups in all three parts of the calcaneal tendon.
Comparing different parts of the tendon in the control group only, we can state that the central part of the calcaneal tendon of rats showed less density of blood vessels when compared with the proximal and distal parts
Discussion
One of the reasons for studying experimental models in tendinopathy is related to the deep knowledge of tissue repair in different phases. Evaluation of the initial phases of injury repair in the calcaneal tendon is the key to understanding injury evolution. Studying experimental models has been found to be an outstanding method for investigating tendinopathy and performing therapies in a continuous and controlled way. Additionally, this method benefits from quantitative and qualitative analyses. 25
One of the components that was studied and reported in literature is the vascular support of the calcaneal tendon, which was thoroughly described by Zantop et al., 24 who studied vascular composition in cadavers and observed that the hypovascularization of the tendon's central region can be a predisposition factor for spontaneous or degenerative injuries. However, Ahmed et al. 26 conducted a histomorphology analysis of the blood supply through conventional light microscopy and found no differences in vessel density in different tendon parts. Kannus et al. 5 stated that there is also hypovascularity and avascularity in tendons of the supraspinatus, biceps brachii, and tibialis anterior muscles.
We did not find scientific literature regarding the composition and vascular dynamics of the calcaneal tendon in animals; such observation deserves attention, given the importance of this subject for the development of therapies that favor blood supply. This study has shown that the composition of a rat's calcaneal tendon differs in the proximal, medial, and distal parts, by having a greater number of vessels in the proximal and distal parts than in the medial part. These results corroborate the findings of Chen et al., 27 who studied the vascular anatomy of the calcaneal tendon in humans and detected a hypovascularized region in the medial part, when compared with the proximal and distal parts. These authors also stated that this medial region may be irrigated mainly by the fibular artery, whereas the proximal and distal parts may be irrigated by the posterior tibial artery. The origin of tendon irrigation was not contemplated in our study, but it was observed that the vascularization pattern in rats is similar to that of humans.
This observation is very relevant, given that literature regarding LLLT for tendon repair points out that therapy should be applied at the medial region of the tendon, which is supposed to be the hypovascularized area. In the study by Oliveira et al.,
16
laser therapy at 830 nm (GaAlAs) was applied at the medial region of the calcaneal tendon after partial injury with only one local treatment, obtaining significant results and favoring fiber realignment. Arruda et al.
28
also used infrared and visible laser (670 and 904 nm, respectively) in the medial region of the calcaneal tendon after tenotomy. However, none of these studies mentioned, approached, or evaluated the effect of vascularization on tissue repair. Regarding the parameters, we had the objective of following some of the same parameters used by Neves et al.
22
and Pinfildi et al.,
29
which used the same infrared wavelength and the density energy that reached from 30 to 40 J/cm2. We have tried to keep some of parameters found in the literature with the purpose of comparing them with other studies already conducted. In further study, we will follow World Association for Laser Therapy (WALT)´s guidelines to standardize some parameters (
We observed that blood vessel area density was proportional to the number of vessels; for example, in distal and proximal regions, blood vessel area density was greater than in the medial region. The medial part is the exact hypovascular region of the calcaneal tendon in humans, and, according to Knobloch, 30 it is the area where most tendinopathies occur. This fact is not exclusively or confirmed to be related to vascularization, but it is a strong hypothesis nonetheless, because a region with less blood supply would be more susceptible to injuries than other tendon regions that are more vascularized and, therefore, receive adequate nutrition to keep the tissue healthy.
Laser applications were performed on the medial part, aiming at improving blood circulation. However, our study has shown that laser irradiation did not increase the number of vessels in the medial part of treatment groups when compared with the control group, given that there was no significant difference among the groups, which were irradiated with infrared laser (830 nm) and visible laser (660 nm), or (the sham group) only a simulated treatment.
The absence of change in the number and density of blood vessels after LLLT may be related to intensity of the impact on the tendon during the injury procedure. Our results showed that the load applied on the tendon might not have been enough to cause inflammation, which would explain the absence of angiogenesis in the model and the similar values of blood vessel number and area density found between experimental and control groups. On the other hand, we observed, in the intragroup analysis, that the addition of LLLT contributed to the permanence of the number of vessels in the medial part, where laser therapy was delivered, when compared with the other parts of the Achilles tendon. When we compare the parts of the tendon in the control group, we can note that the difference is greater among the parts when compared with other groups.
Nevertheless, the model used in the current study deserves attention, because it simulates tendon lesions that are common in humans. However, more studies are necessary to determine the ideal load needed to cause the wound, as well as to investigate the influence of LLLT.
Conclusions
Based on the results of this study, we conclude that LLLT had no effect on the studied parameters, and that vascularization of rat tendon is similar to in humans, which contributes to the studies of therapies that have been applied in humans.
Footnotes
Statement on the Welfare of Animals
All procedures performed in studies involving animals were in accordance with the ethical standards of the institution or practice at which the studies were conducted.
Author Disclosure Statement
No competing financial interests exist.