
Abstract

A
Transparency is one crucial factor for EBM, and there are some indications that a lack of transparency has become an increasing problem. The Cochrane Collaboration seems to have been unable to avoid influence from “Big Pharma” in some of their editorial review boards dealing with pain. By clicking my way through links in their web site, I found that 8 out of 14 editorial board members in the Musculoskeletal Group have received some sort of funding from pharmaceutical companies. In the Back Group, conflicts of interest are less frequent, but previous editorial board members still have had funding, honoraria, and travel costs paid for by pharmaceutical firms.
The Pain and Palliative and Supportive Care Review Group has, perhaps, the most interesting web site with respect to transparency, as I was unable to find any list with disclosures of conflicts of interest for the editorial board there. This contrasts with some of the recent reviews from this review group which state that: “…have received research support from charities, government and industry sources…consulted for various pharmaceutical companies…and…have received lecture fees from pharmaceutical companies related to analgesics.” 2 The latest Cochrane review of topical nonsteroidal anti-inflammatory drugs (NSAIDs) for acute musculoskeletal pain, states that reviewers: “…have no conflicts relating to this review or any similar product.” This is, however, a question of definition. Another issue possibly indicating a decline in transparency is their current procedure for exclusion of trials if only average pain scores, and not dichotomous data of success, are reported. In their topical NSAID review, seven trials were excluded for not reporting dichotomous data. For low-level laser therapy (LLLT) trials, it has been more common to report mean pain scores rather than dichotomized outcomes. Consequently, our research group has reported both continuous and dichotomized outcome measures, to give the fullest picture of the evidence from available LLLT data. Omitting continuous data, which consist of more than half of the evidence, is in my opinion, scientifically unacceptable, whereas integrating both outcome measures will make the review conclusion more robust.
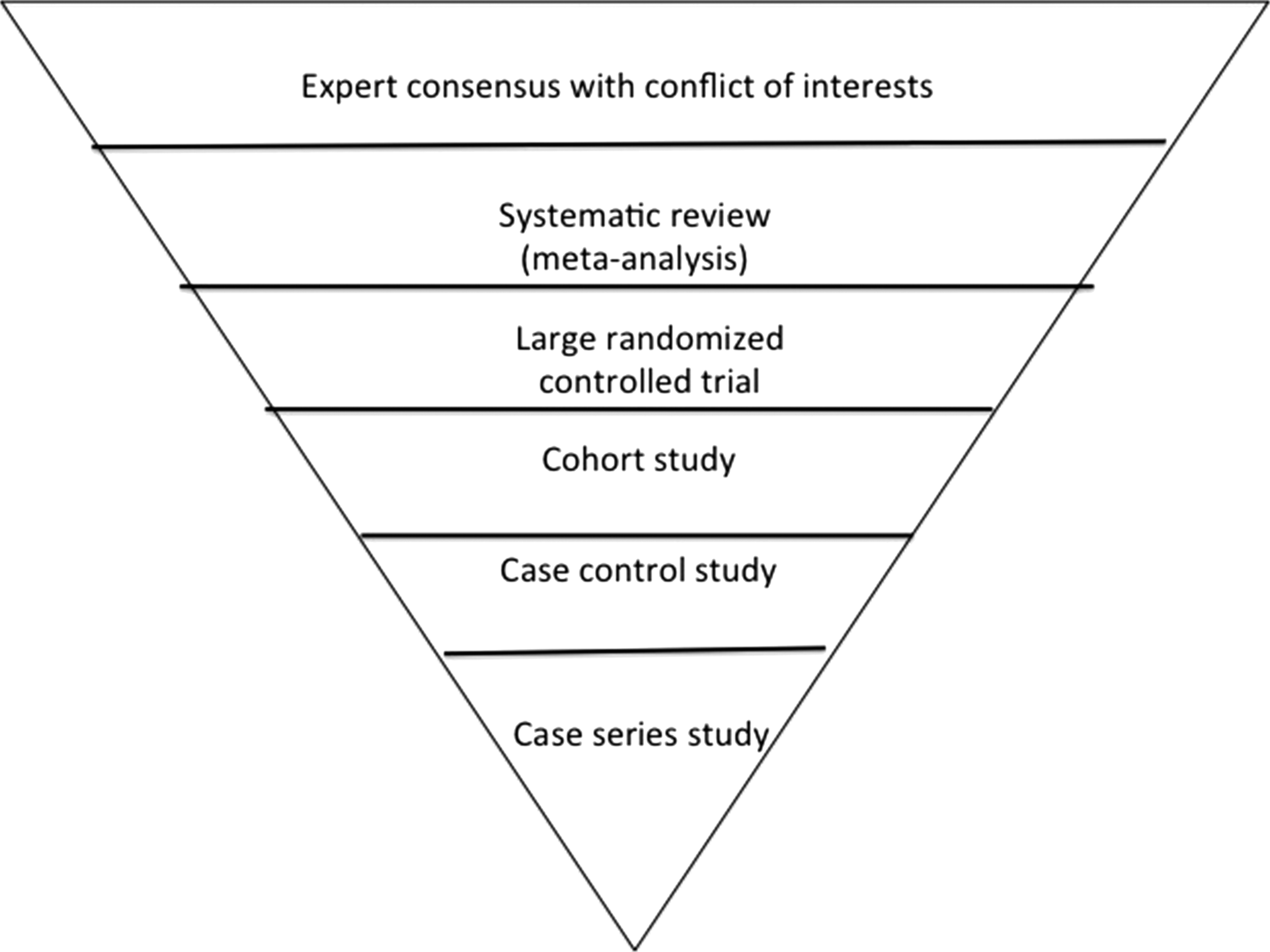
Evidence-based pyramid turned upside down.
The question then is, why are continuous data omitted from meta-analyses. The most obvious reason is that it makes the results look better than they are. This is easier to understand if I use an example and convert the two types of outcomes to percentages. I have previously calculated in a meta-analysis of knee osteoarthritis that the mean effect of NSAIDs on a 100 mm visual analogue scale (VAS) was only 7.9 mm over placebo. 3 If I take one included study 4 as an example, mean pain was reduced from baseline pain at 60 mm to 36 mm in the NSAID groups and to 42.6 mm in the placebo group. However, the percentage difference between NSAID and placebo in pain reduction was only (40%−29%=11%), but if one uses a responder cutoff value of at least 50% pain reduction, then, because of variance, the number of responders in the NSAID group will probably be ∼1 in 5, but the number is probably only 1 in 10 in the placebo group. In this way, the reader is seduced into thinking that NSAIDs are 200% more effective than placebo, although the mean difference is only a mere 11%. The second problem with this choice of dichothomous outcome is that most trial data for LLLT must be converted by statistical formulas from the continuous data in the LLLT trial reports. It can be argued that this will imply a barrier, which makes it more difficult to compare effects of NSAID across other interventions such as LLLT.
Another question is why are esoteric meta-analysis methods and conflicts of interest important when considering the scientific evidence of osteoarthritis treatments. The answer is simple. When you have >40 competing treatment methods for osteoarthritis, then comparisons of effects and harms must be made on available data, assessments of trial quality, and equal terms. There are strong indices that reviewers receiving financial benefits from industry reach significantly more positive conclusions from similar trial material than do reviewers without conflicts of interest. 5 It is very disappointing that entities such as the Cochrane Collaboration and the Osteoarthritis Research Society International (OARSI) allow reviewers and editors to have conflicts of interest with Big Pharma when reviewing competing nonpharmacological treatments. The OARSI started out in 2007 with making systematic reviews of the evidence levels and meta-analyses of the 51 competing treatment methods. 6 This evolved into making clinical guidelines partly based on evidence and partly based on consensus from existing guidelines. It was found that LLLT had the highest (and similar) level of evidence to that for NSAIDs, as well as a comparable treatment effect size on pain, 7 but LLLT was left out of the new OARSI guidelines because it was infrequently recommended by other guidelines.
That could be considered acceptable if the LLLT evidence was presented by OARSI at the top tier of the level of evidence, the quality of studies, and the effect size, 8 but in 2014, it all changed when OARSI left the evidence mostly untouched, omitted LLLT completely, and founded their guidelines largely on expert consensus. After a quarter of a century with EBM, it is sad to witness how OARSI has effectively turned the evidence pyramid upside down. I should also add that 9 out of 17 members of the OARSI guideline board declare conflicts of interest with Big Pharma.
Consequently, I prefer to seek advice directly from the data in high quality trials in osteoarthritis, rather than relying on biased expert opinions. I feel that I owe my patients the option of a safer nonpharmacological treatment alternative for their osteoarthritic pain.