
Abstract
Introduction
T
Dentin is a complex structure composed of carbonated apatitic mineral, collagen, and water. 6 Dentin contains tubules that increase in number and diameter with depth, and its sensitivity is caused by the nerve fibers that enter the periodontoblastic space within the dentinal tubules. The nerve fibers are responsible for sensitivity recognition and transmission to the pulp organ. 7
The most accepted theory for the phenomenon of hypersensitivity is the hydrodynamic theory of Brännström, which suggests that dentin hypersensitivity occurs when there is movement of the fluid inside the tubules. The fluid movement causes pressure in the odontoblasts, which stimulates the response of mechanoreceptors of the adjacent nerve fibers and consequently causes pain. 2,8 The factors that determine different degrees of dentin hypersensitivity are the number and diameter of tubules, as well as their permeability. In sensitive teeth, the number of tubules per area is approximately eight times that of nonsenstive teeth. Tubule diameter is also double that of nonsensitive teeth. 9
Based on the concept that sensitive dentin is more permeable, agents capable of blocking the dentinal tubules have been developed. There are several factors that limit the effectiveness of current commercial desensitizing treatments, including the limited time that the patient feels sensitivity relief. Because the relief is transient, the patient must repeatedly apply the dentin desensitizing agent. 10
The most commonly used agent for dentin desensitization is fluoride, whose action is associated with the formation of precipitates similar to calcium fluoride (CaF2), which can occlude dentinal tubules. However, this deposition does not remain in the tubules, notwithstanding the environmental stress in the oral conditions, which degrade in a short period of time. 11 –13
Another agent applied for the reduction of permeability is an adhesive system, which acts by establishing hybrid layer adhesion. However, studies report that the hybrid layer may be porous, with areas of exposed collagen. 14 –16 When the adhesive is used only for purposes of reducing permeability, it quickly loses its efficacy. 17,18 Therefore, alternatives for improving adhesive penetration and longevity have been developed, such as collagen deproteinization and laser exposure. 19,20
Researchers suggested that the removal of the collagen matrix with a proteolytic agent, such as NaOCl, can improve the sealing of the tubules. The proteolytic agent increases the porosity of the dentin, which allows penetration of the adhesive into the lateral branches. Increased infiltration of the adhesive into the lateral branches can improve the sealing of tubules, 21 with concomitant reduced dentin hypersensitivity. 22,23
The Nd:YAG laser, in turn, is capable of increasing the temperature such that the dentin melts and obliterates the dentinal tubules. 24,25 In most cases, the laser system applied before the adhesive resulted in reduced bond strength. The reduced bond strength was attributed to denaturation of the organic components as a result of the heat generated by the laser. 26 In contrast to the results with Nd:YAG, Gonçalves et al. 20 reported a significant increase in bond strength when Nd:YLF laser was used. Based on these contradictory results, it was hypothesized that more effective sealing of dentinal tubules could be achieved by combining laser treatment with the conventional reagents.
Some methods have been used to verify dentin permeability alterations: scanning electron microscopy (SEM) and transmission electron microscopy (TEM) enable the observation of precipitates that obliterate the dentinal tubules; 26,27 fluorescent light microscopy evaluates the depth of penetration of surface treatments 19 (clinical reports verify reduction in sensitivity after treatment, but do this subjectively); 13,17 and the model used in this study offers the possibility of direct and accurate measurement of the fluid flow that pervades the dentin in a laboratory simulation. 28 –30
The objective of this in vitro study was to evaluate dentin permeability after dentin hypersensitivity treatments: fluoride, adhesive system, and collagen NaOCl-induced deproteinization with and without Nd:YAG laser exposure, and after erosive and abrasive challenges.
Null hypotheses are as follows: H0, the different dentin hypersensitivity treatments did not influence dentin permeability; and H1, the experimental conditions did not influence dentin permeability.
Materials and Methods
Specimen preparation
Eighty freshly extracted bovine incisors were collected and stored in distilled water at 4°C until the time of use. Dentin disks with 6 mm diameter and 1 mm thickness were obtained 31,32 through the reduction of crown dentin with a silicon carbide granulation 600 sandpaper coupled to a circular polishing machine. The surfaces were then polished with 1200 and 2400 sandpaper for 30 sec each to obtain specimens with accurate surface smoothness.
As permeability varies with the thickness of dentin, a digital caliper (Starrett, Itu, São Paulo, Brazil) was used to standardize the final thickness. The specimens were cleaned for 5 min using deionized water and an ultrasonic cleaner (Ultrasonic Cleaner, Odontobrás, Brazil).
Permeability
The split chamber model was used, in which the pulpal side of the dentin disk is placed in contact with a fluid under pressure and the other side is under atmospheric pressure. 31 A device was used to measure permeability (THD - 02b - Odeme Dental Research, Joaçaba, SC, Brazil). The perfusion fluid flows from a reservoir to the perfusion chamber through a capillary tube. After filling the entire system with the perfusion fluid (deionized water), air was introduced into the capillary tube by means of a micrometer syringe. The rate of movement of fluid through the dentin disk was measured by following the linear displacement of the air bubble in the capillary tube (starting position/final position) for 3 min, using a digital caliper 29,32 –34 (Fig. 1). The measurement of the displacement of the bubble was used to calculate the permeability rate as a function of time, pressure, and the dentin disk area. The pressure used was 10 psi 29,32,34
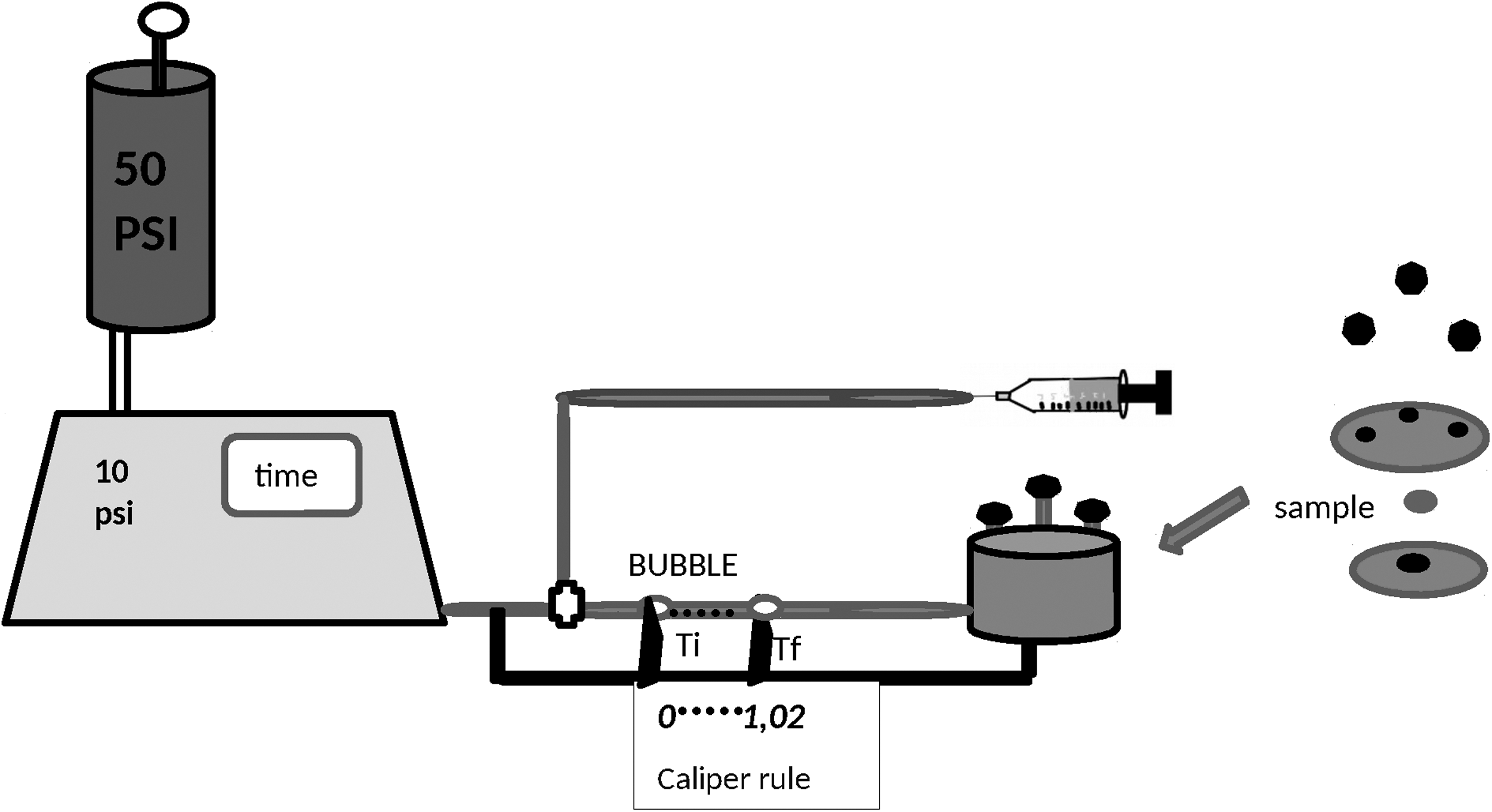
Schematic figure of permeability measurement.
For the calculation of fluid flow through the dentin disk, it was first calculated that the filtration rate (
Four readings were performed successively on each disk at all measuring times, yielding four values of
Dentin permeability was expressed in values of hydraulic conductance (
Permeability was recorded in four distinct stages: (1) with the presence of the smear layer on the occlusal surface (minimum permeability), (2) after 0.5 M ethylenediaminetetraacetic acid (EDTA) application for 5 min (maximum permeability), (3) after saliva storage and treatments (treatment), and (4) after the erosive/abrasive challenge (challenge). 30
Minimum permeability
To compare with the conditions of teeth with no sensitivity,
30
the initial permeability was measured while there was an intact smear layer on the buccal face.
29,30
The smear layer formed on the pulp side of the specimen was removed with EDTA application for 5 min.
32,33
To ensure that EDTA only touched the pulp surface of the dentin disk, the specimen was placed in a silicone matrix with the exact dimensions of the specimen. The
Maximum permeability
To simulate the open dentin tubules present in cervical hypersensitive areas, the dentin smear layer was removed using 0.5M EDTA for 5 min.
28,33
The
Treatments
The specimens were positioned in a silicone matrix, so that only the outer surface received treatment, according to Table 1: Group C, control group–no treatment; Group L, Nd:YAG laser; Group F, fluoride varnish; Group FL, fluoride varnish plus Nd:YAG laser; Group A, adhesive system plus light curing; Group AL, adhesive system plus Nd:YAG laser plus light curing; 20 Group D, 10% NaOCl plus adhesive system plus light curing; 19 and Group DL, 10% NaOCl plus adhesive system plus Nd:YAG laser plus light curing.
Nd:YAG Laser (Pulse Master 600 IQ, American Dental Technologies) was irradiated at 60 mJ/pulse/10 Hz/47.7 J/cm2/1 W. 35,36 The diameter of the optical fiber was 400 μm, and the laser was applied to the surface without contact, with the angulation of the tip perpendicular to the surface of the specimen, at an approximate 2 mm distance, by scanning the surface freehand for 60 sec.
After the treatments, the specimens were placed in a silicone matrix and immersed in artificial saliva
37
for 24 h, to provide the contact of saliva only with the treated surface, and dentin permeability was evaluated (
Erosive and abrasive challenge
Erosive cycles were performed for 5 days by immersion of the specimens in Coca-Cola (Coca Cola Company Spal, Porto Real, RJ, Brazil, pH 2.6, without stirring, at 25°C), four times a day for 90 sec each.
After the first and last erosive challenge of each day, all specimens were brushed for the abrasive challenge. 38,39
A straight soft bristle toothbrush and a toothpaste were used in the brushing simulation device, (model MEV −2T/Odeme Dental Research - Joaçaba, SC, Brazil). The device has a steel arm that swings. This arm is fitted to a crossbar with six vertical axes. Each axis has adjustable metal braces for the placement of the toothbrushes. They were adapted in contact with the specimen surface, displayed in stainless steel niches, and immersed in toothpaste solution. The device has a sensor to control temperature at 37°C.
The toothpaste was diluted in 3:1 proportions, meaning three parts of toothpaste to one part of deionized water.
40
The specimens were subjected to brushing cycles with a 3.8 cm range and 200 g weight. Under these conditions, 24,000 cycles were performed corresponding to 1 year of toothbrushing.
41
After the erosive/abrasive challenge, permeability data were recorded (
Permeability calculation in percentage after each phase
Permeability of each specimem, after each phase, was calculated as a percentage relative to the maximum permeability. 28 –30,32,34
The following formula was applied:
where:
As all disks present a certain difference in diameter and number of tubules, a biological variability is expected among all groups. 31 To reduce this variability, each disk was its own control. 29,31 –33 and the data were analyzed by two way repeated measures ANOVA (groups and phases) and Tukey test (5%).
SEM
The SEM was performed only to assess the quality of dentin after abrasive/erosive challenges, in terms of tubule obliteration. One specimen of each group was examined using electron microscopy (JMS 5310 - Jeol Scientific Instruments Brazil Ltda. - SP, BR).
Results
Table 2 and Fig. 2 show the values in percentage, mean, and standard deviation for each treatment in the experimental conditions (minimum initial permeability = minimum, permeability after treatment = treatment, and permeability after erosive and abrasive challenges = challenge).
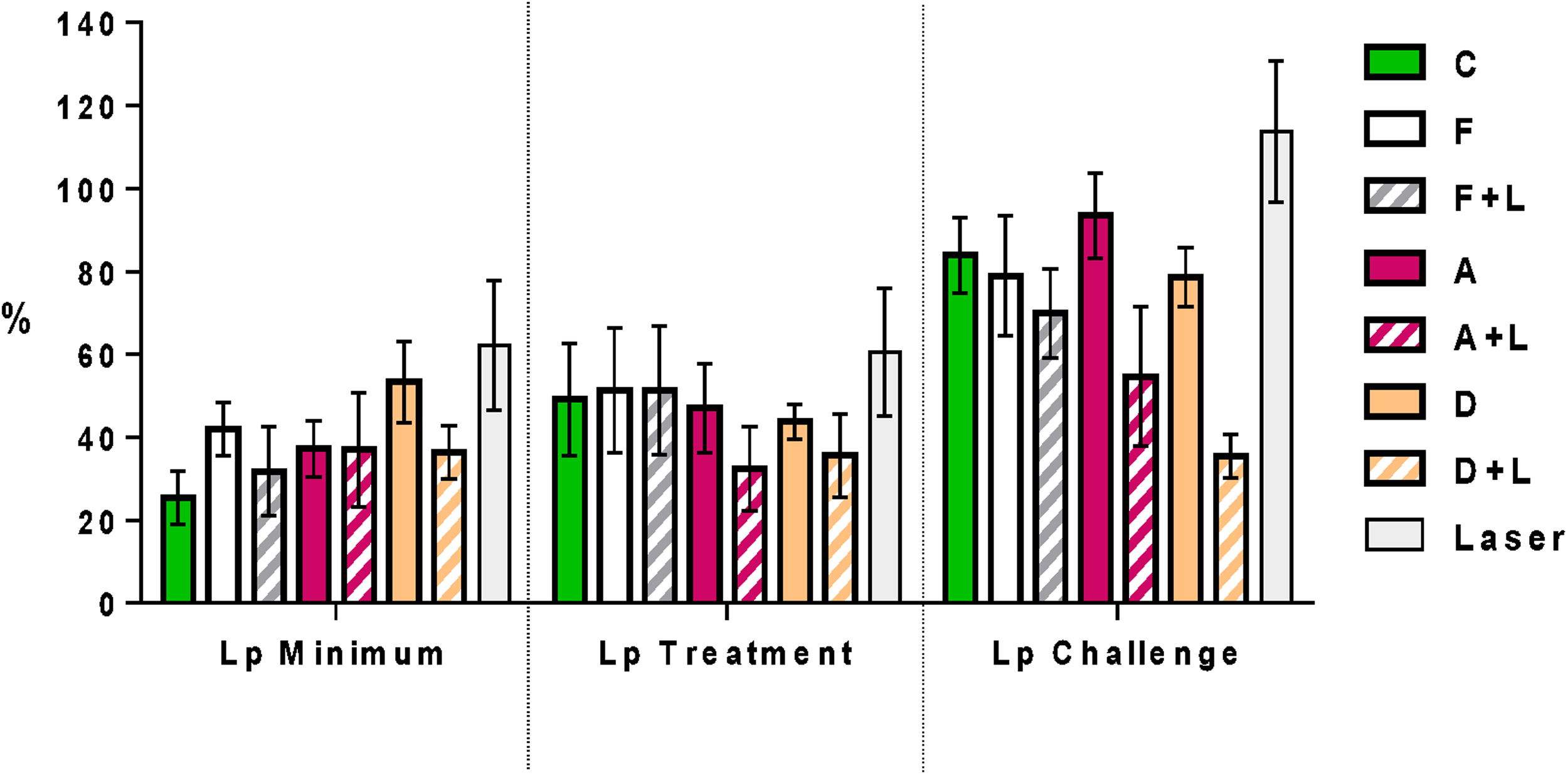
Graph of mean ± standard deviation of the percentage of permeability in each group for each experimental condition.
The effects of the two primary factors: group (control, fluoride, laser, fluoride plus laser, adhesive, adhesive plus laser, deproteinization, and deproteinization plus laser) and conditions (minimum treatment and challenge) and their interaction according to the ANOVA for repeated measures with two factors (group and conditions), all treatments showed a statistically significant effect (p < 0.05) in permeability variation. ANOVA was shown to be statistically significant in the factors: Group (p = 0.0001), conditions (p = 0.0001), and on interaction (p = 0.0001).
These are the results of the Tukey test (α = 0.05) in which the three experimental conditions (minimum, treatment, and challenge) were compared within each group (C, L, F, FL, A, AL, D, DL), and the difference was statistically significant. It was observed that when comparing the conditions minimum x treatment, group C, group FL, group A, and group D were statistically different, and that when comparing the conditions minimum x challenge and treatment x challenge, only the DL group showed no significant differences.
Here are the results of the Tukey test (α = 0.05) in which the eight groups were compared within each experimental condition. It can be observed that within the minimum condition the statistical difference found was between groups C × F, C × D, C × L, F × L, FL × D, FL × L, A × D, A × L, AL × D, AL × D, AL × L, D × DL, and DL × L. For the treatment condition there was statistical difference between groups C × AL, F × AL, FL × AL, AL × L, D × DL, and DL × L. Within the condition challenge there was no difference between groups C × F, C × FL, C × A, C × D, F × FL, F × A, F × D, FL × AL, FL × D, and A × D.
SEM
Photomicrographs illustrating the dentinal tubules after treatments represent the erosive/abrasive challenge (Fig. 3.)
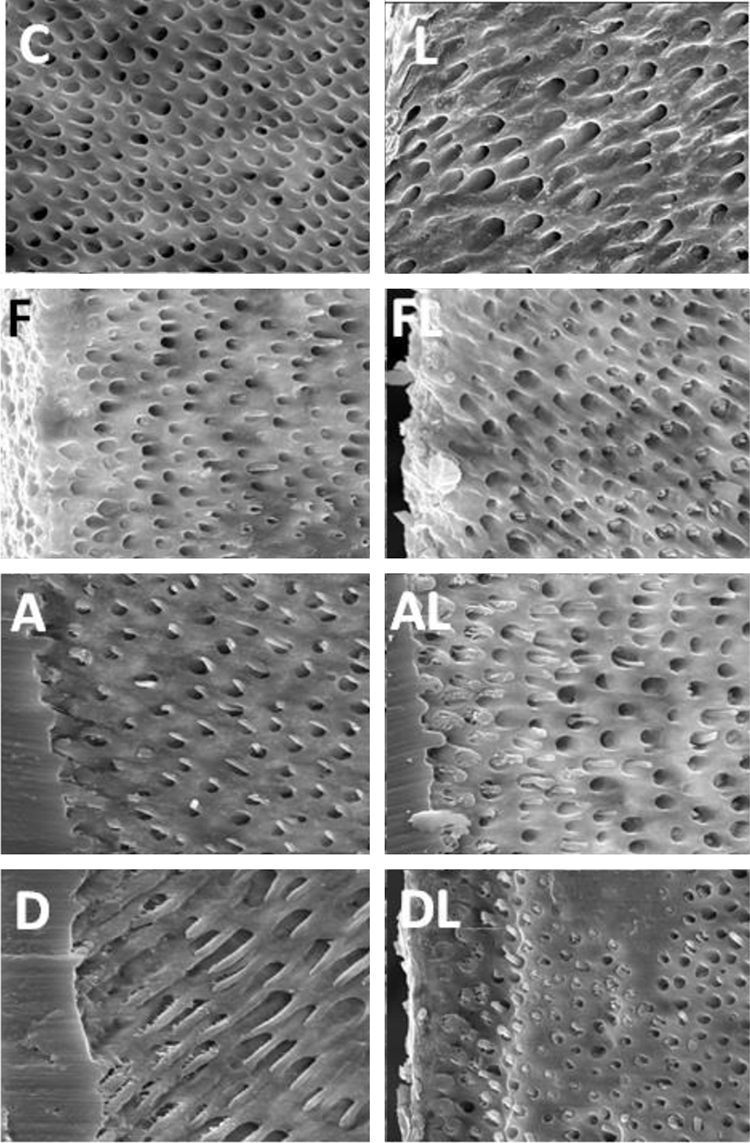
Photomicrographs illustrating the dentinal tubules after erosive/abrasive challenge (original magnification X 3000).
It can be observed that in group C, tubules are completely clear. Group L presents open tubules. Groups F and FL present precipitates within the mouths of the tubules, but do not totally obliterate them. Groups A, AL, D, and DL present resin tags. Group DL shows more significant dentin tubule obliteration per surface area.
Discussion
Dentin hypersensitivity treatments include oxalate-based desensitizers, gel or varnish fluorides, toothpastes, and dentin adhesives. The primary mechanism of action of these desensitizing agents is the total or partial obliteration of exposed dentinal tubules, with a consequent reduction in dentin permeability. 11,17,30,34,42,43 These treatments can be removed by the acid present in food and/or by the mechanical abrasion process associated with toothbrushing. Therefore, one of the limitations of current treatments for dentin hypersensitivity is the limited time that they are effective.
Nd:YAG laser promotes tubule obliteration by the melting and recrystallization of the dentin mineral component, thereby reducing dentinal permeability. Some studies suggest that laser can induce analgesia by direct action on the nerve, promoting a suppression of the intradental nerve responses to both electrical and mechanical stimuli. 44 –47 In vivo studies could assure the efectiveness of such a response.
In this study, minimum permeability, corresponding to the nonsensitive tooth permeability, was used as a reference to analyze the treatments performed after obtaining maximum permeability (EDTA). The results of the comparison between the conditions minimum by treatment showed that the fluoride varnish (F), adhesive and laser (AL), 10% NaOCl plus adhesive (D), and 10% NaOCl plus adhesive and laser (DL) groups resulted in the return of the permeability to minimum values. These results suggest that the treatments blocked the movement of dentinal fluid. The differences in movement of dentinal fluid are attributed to the treatments, as opposed to precipitates from the artificial saliva. This conclusion is supported by the observation that permeability in the control group was above the minimum values after storage in artificial saliva.
One of the selected treatments was fluoride varnish (Duraphat), whose action is associated with the formation of precipitates similar to CaF2. Although it does not present different results from that of acidulated phosphate fluoride in terms of dental erosion blocking, 43 this varnish was chosen because of its intense pigmentation. It was hypothesized that the pigmentation would potentiate the effects of the laser. The results, however, did not confirm this hypothesis, showing no statistically significant difference when compared with fluoride varnish without the laser. The SEM images illustrate the similarity in the partial obliteration of the tubules with precipitates.
The adhesive used in this study was Scotchbond Universal Adhesive. The self-etching technique was chosen, as the specimens had had their smear layer removed previously and the dentinal tubules exposed with EDTA to measure maximum permeability. There was a statistically significant reduction in permeability when the adhesive was used in combination with the laser as compared with the adhesive alone. There are several variables that may have contributed to this difference. The heat generated by the laser could have increased the reaction kinetics associated with the adhesive. The heat could have melted the mineral and organic components of the dentin, leading to sealing of tubules and lateral tubule projections. Differentiating between these variables requires further investigation, but the results suggest reduced dentin permeability when the adhesive is used in conjunction with laser application. These results support the conclusions presented by Gonçalves et al., 20 using a laser with a different wavelength; that is, Nd:YLF as opposed to the Nd:YAG used in this investigation. Gonçalves and colleagues 20 report that the combination of the Nd:YLF laser with the adhesive is capable of forming larger and longer tags and a more uniform hybrid layer, which means that there is an effective reduction of dentin permeability. 48
The deproteinization was performed according to the technique recommended by Dayem in 2010, 19 with modification as to the dentin demineralization with EDTA instead of phosphoric acid. The combination of deproteinization and the laser has not been reported in the literature. This combination provided the best results in terms of reducing permeability. Dayem hypothesizes that the Nd:YAG laser also takes part in deproteinization. Potentially, the heat from the Nd:YAG laser leads to disorganization and/or denaturing of the remaining organic component within the dentin. 49 Therefore, deproteinization may have been increased by the combination of both (NaOCl and laser). The SEM images illustrate blockage of the dentin tubules with the NaOCl treatment in combination with the laser.
The fluoride varnish plus laser application group did not show a return to the minimum values of permeability. These results contradict the literature, in which the association, as in Group FL, achieved better results. 11,13 There is a potential that the colored film of varnish prevented the modification of dentin, contrary to what happens when the adhesive, which is transparent, is placed. When comparing the results for the factor treatment, statistical difference could be seen only between the F and FL groups with the AL group, with lower permeability for the AL group.
Permeability after the abrasive and erosive challenge was performed to verify the durability of the treatment, simulating a 1 year period. 38,39,41 The results showed that the groups associated with the laser had lower permeability than the equivalent groups without this association. However, statistically, when comparing the condition treatment by challenge, only deproteinization plus laser showed the same permeability, being, therefore, the longer-lasting treatment. This may have occurred because the deproteinized dentin, with collagen fibers partially removed, leads to a more porous structure. The porous structure allows space for a broader and deeper penetration of adhesive among the tubules, forming a stronger barrier when associated with the laser. 19,50
Within the condition challenge, statistical differences were noticed between group deproteinization plus laser (DL) and all other groups. The AL group differed statistically from groups C, F, A, and D, groups in which the treatment was not associated with the laser, demonstrating that association with the laser increases the durability of treatments for reducing permeability. However, for group L, when laser was not associated to the treatments, there was a significant increase in dentin permeability, and, therefore, the laser cannot be considered a long lasting treatment for hypersensitivity. Further studies are necessary to verify new interactions, as with desensitizing agents and gel fluorides associated with the laser.
Direct comparison of this study's results with clinical desensitization is limited as a result of several factors. One of such factors is the use of bovine teeth. Bovine teeth were used because they are more standardized in terms of genetic strain, age, and diet. These factors reduce the variability in terms of the number and diameter of dentinal tubules. 51 A pressure of 10 psi = 703 cmH2O 28,29,32 was used, which is much higher than the physiologic dental pressure (15–40 cmH2O). This pressure allowed the investigator to read the movement of the bubble in the permeability device. 52 In this study, deionized water as opposed to pulpal fluid was used for dentin perfusion. This allows ready fluid flow within the dentinal tubules without potential interference from organic substances. 29,32 –34 There may be inconsistency in the fluid flow because of changes within the capillary tube with time. For example, leachates from the capillary tube may skew the results from one replicate to the next. 53 Within the limits of this investigation, it can be concluded that, in general, the treatments for reducing dentin permeability were more effective when combined with the application of the Nd:YAG laser. Furthermore, only the DL treatment was effective at reducing dentin permeability after the erosive/abrasive challenge.
Conclusions
Dentin hypersensitivity treatments reduced dentin permeability when associated with Nd:YAG laser, even after erosive/abrasive challenges. The association between adhesive and Nd:YAG laser led to the lowest rate of permeability after 24 h. NaOCl-induced deproteinization associated with Nd:YAG laser showed the lowest permeability rate after erosive/abrasive challenges.
Footnotes
Author Disclosure Statement
No competing financial interests exist.