
Abstract
Introduction
O
Conventional methods have been developed over the years to remove fixed failed implants. These methods include ultrasonic and Piezo Sonic devices, high speed burs, and trephine burs. Trephine burs are considered to be the best conventional choice because of their effectiveness and rapid removal of implants simply by removing a block of bone surrounding the implant. Nevertheless, mandibular stress fractures after using them have been detected. 3 Osteomyelitis has also been reported as a complication, particularly if the bone has been overheated. 4 In order to overcome these disadvantages, laser technology has been investigated as a safer alternative for removing failed implants. 5
Over the past decade, different types of surgical lasers have been investigated in bone surgery. 6,7 Among them are the Erbium-doped yttrium aluminium garnet (Er:YAG) (2940 nm) and the Erbium,chromium:yttrium-scandium-gallium-garnet (Er,Cr:YSGG) (2780 nm) which have been described as suitable wavelengths for cutting human bone. 8 –11 The mechanism of cutting hard tissues with erbium lasers is accomplished by the interaction of the laser energy with water molecules; absorption of laser energy by the water produces microexplosions, which are responsible for removing calcified hard tissues such as enamel, cementum, and bone. 12,13 It has also shown the capability of ablating hard tissues without causing thermal damage. 10
Moreover, the tip of the laser device can be applied in a way enabling it to reach areas that might be inaccessible with the traditional methods. 14,15 Additional advantages of the lasers include: rapid healing, reduced postoperative complications, reduced trauma, infection control, and a sterilized surgical field. 16
This study compares the Er,Cr:YSGG laser and the traditional trephine bur with respect to the volume of bone loss during removal of osseointegrated dental implants, the procedure duration, and the morphological changes of bone tissues after implant removal.
Materials and Methods
In this investigation, 3 human mandibles obtained from the Department of Anatomy, RWTH Aachen University Hospital, Aachen, Germany were utilized; a total of 12 SPI implants with a diameter of 5 mm and a length of 12 mm were used (SPI, The Original Spiral Implant, Alpha-Bio Tech, Petach, Tikva, Israel), inserting 4 implants in each mandible using a drilling hand piece and surgical burs (Figs. 1 and 2).

Implant placement.

Mandible after inserting four implants.
After the insertion procedure, the implant stability quotient (ISQ) was measured for each implant using Osstell ISQ system (Götenberg, Sweden) to insure initial stability (Fig. 3). The acceptable stability range lies between 55 and 85 ISQ, and all implants showed an ISQ stability score >70 both mesially and buccally, indicating proper stability. 17 The implants were then divided into two groups (n = 6) for removal.

Implant stability quotient (ISQ) measurement.
Using the split mouth technique, two implants were separated from each mandible using a trephine bur with an inner diameter of 6 mm and an outer diameter of 7 mm (Figs. 4 and 5) running at a speed of 1200 rpm in the presence of water irrigation to ensure cooling (Meisinger, Neuss, Germany). 4 The remaining implants were separated from the bone using the Er,Cr:YSGG laser (2780 nm) (iPlus, Biolase Technology Inc., Irvine, CA) using the following settings (power 6 W, pulse duration 50 μs, frequency 20 Hz, water setting 60, air setting 30). A glass tip with a diameter of 500 μm (MZ5) was positioned 1–2 mm away from the target tissue during laser application (Figs. 6 and 7) (Table 1). Removal of the implants was done by two experts in oral surgery in order to ensure the blinded nature of the study, 18 and both surgeons followed the same instructions for implant removal. During the removal procedure, both the laser and the trephine bur were applied until the implants became clinically loose; they were then removed using forceps or tweezers.

Implant separation using the trephine bur.

Implant removal with forceps after separation with the trephine bur.
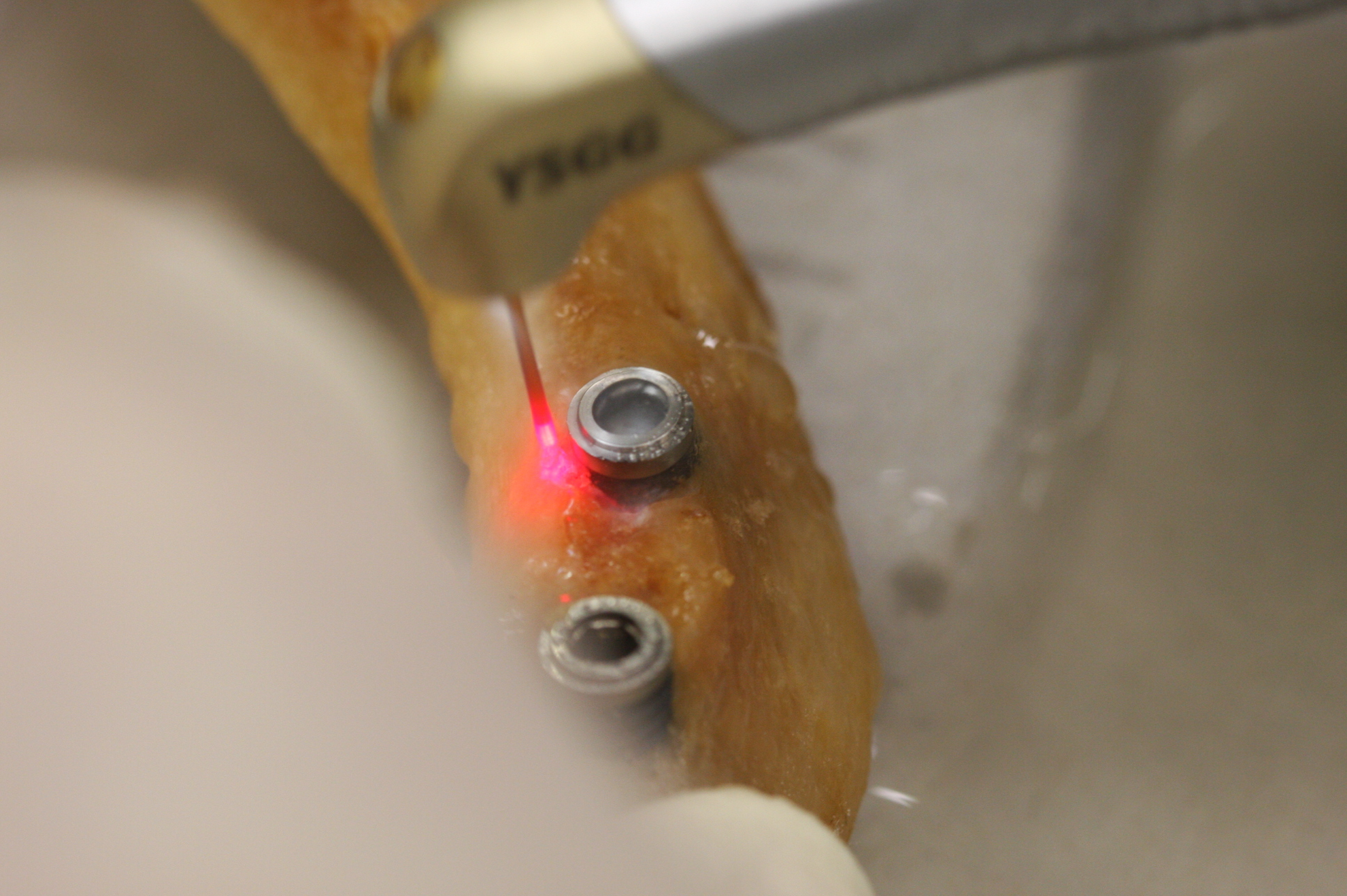
Implant separation using the Erbium,chromium: yttrium-scandium-gallium-garnet (Er,Cr:YSGG) laser.

Implant removal with tweezers after separation with Erbium,chromium:yttrium-scandium-gallium-garnet (Er,Cr:YSGG) laser.
Bone loss measurement
The volume of the bone removed during implant removal was calculated by filling the holes with mercury (Hg) and measuring its volume. Mercury was chosen because its body remains intact and will not flow within the bone, it addition to the ease of calculating mercury's weight and volume, as it will not evaporate at room emperature. The bone lose measurement procedure was as follows: the mandibular bone was weighed before filling the holes with mercury; then it was weighed again after filling each hole at a time to calculate the exact volume of each cavity. The weight of mercury at room temperature was then divided by its density (13.534 g/cm3) to obtain its volume.
Duration of procedure measurement
The time required to remove each implant was measured using a digital stopwatch (Casio, Shibuya, Tokyo, Japan).
Bone morphology examination
Two different holes were randomly selected to collect bone specimens for morphological examination, one sample was obtained from a cavity prepared with the trephine bur, and the other was obtained from the cavity prepared with the Er,Cr:YSGG laser. The specimens were prepared for examination under the scanning electron microscope (SEM). They underwent primary fixation with 2% glutaraldehyde (GTA) followed by dehydration with 50–100% ethanol for 7 h. Both specimens were examined under the SEM (ESEM XL30 FEG, Eindhoven, Netherlands). 19 –22
Statistical analysis
Mann–Whitney U test for independent samples was used in the statistical analysis; denoting a p value of ≤0.05 as significant. The analysis was performed using SPSS software for windows, version 15.0 (SPSS Inc., Chicago, IL).
Results
Bone loss
The results of the study show that the holes prepared with the Er,Cr:YSGG had a mean volume of 0.302 cm3, whereas the conventional trephine group showed a higher mean volume of 0.519 cm3 (Table 2).
Procedure time
The time required to complete the operation with the conventional method was shorter than the time needed with the Er,Cr:YSGG laser method. The former technique was completed with a mean of 17.1 sec, whereas the latter required a mean of 44.3 sec (Table 3).
Morphological results
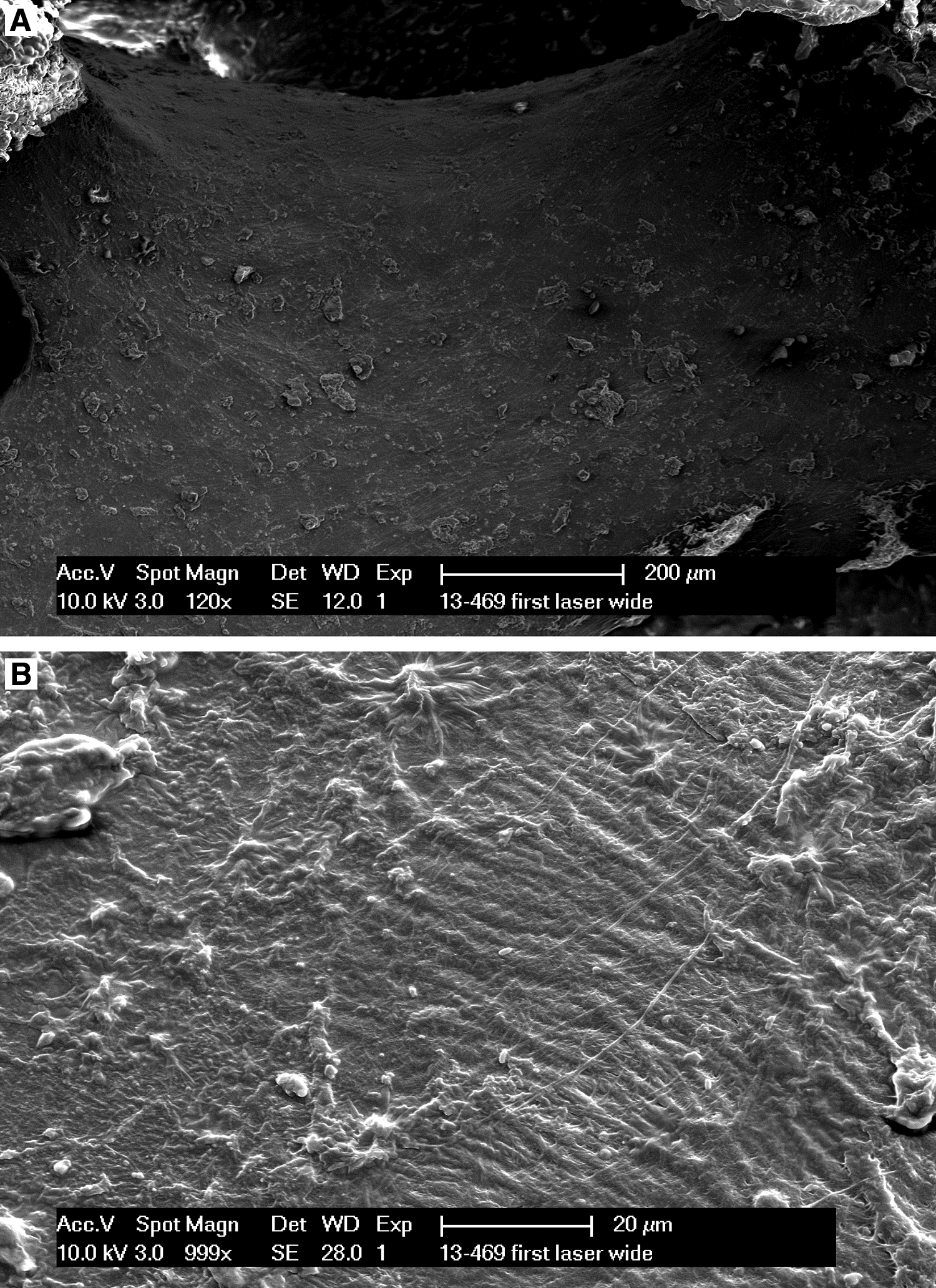
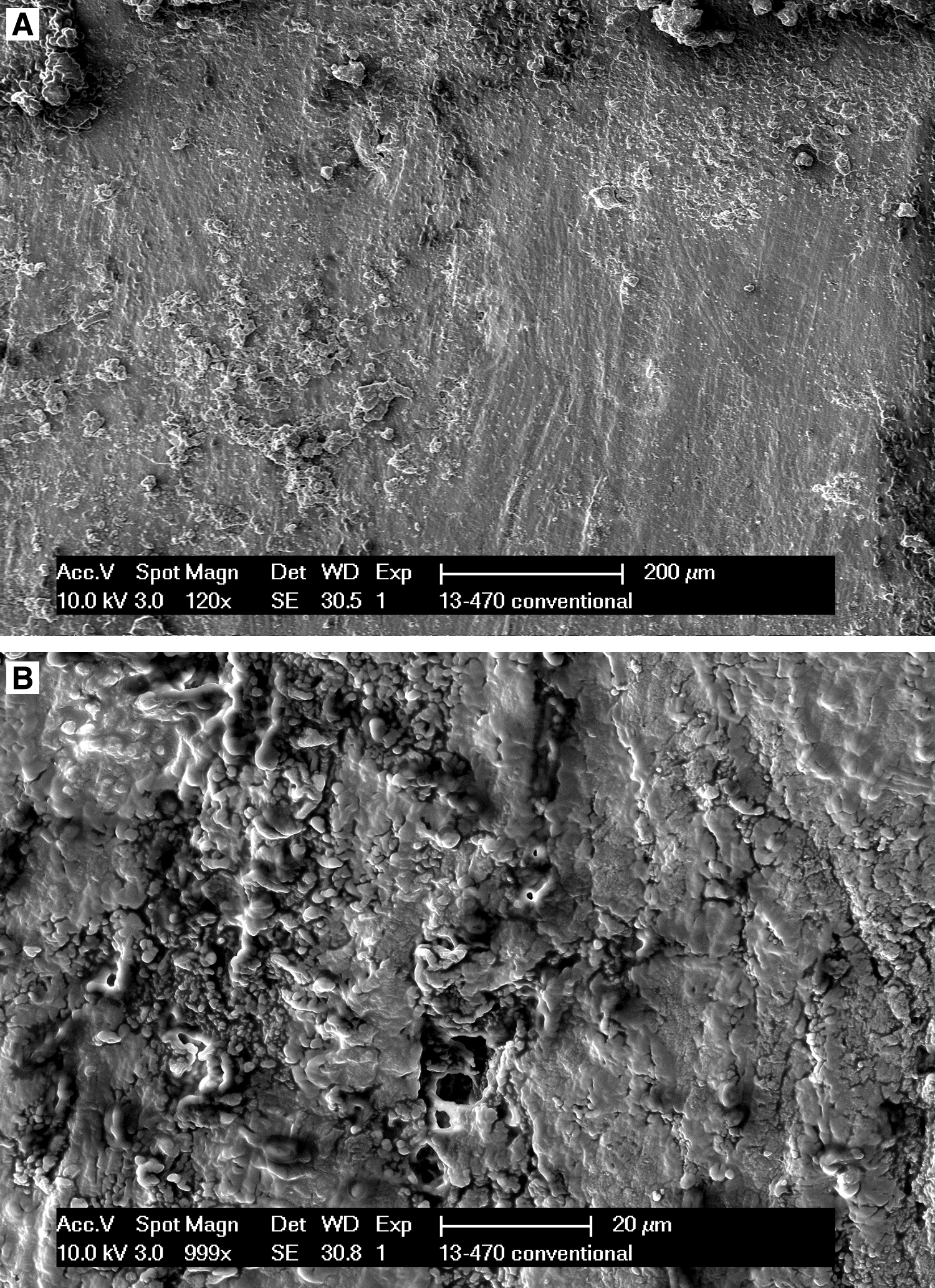
SEM observations for the specimen taken from the Er,Cr:YSGG hole showed well-defined edges and a smear-layer-free surface with a characteristically rough appearance and intertrabecular spaces with no organic matrix (Fig. 8A). The trabecular bone had a normal appearance and showed no signs of thermal damage (Fig. 8B). In the specimen taken from the trephine bur group, the bone surface was coated with a smear layer and fiber-like debris (Fig. 9A). Abnormal fungiform spherical formations and visible microcracks on the bone surface were observed (Fig. 9B).
Discussion
Previous studies concerned with the efficacy and safety of using the Er,Cr:YSGG in dental procedures have proven it to be an adequate tool in manipulating and handling bone and dental hard tissues, 23 in addition to its ability to ablate teeth and bone without damaging the pulp or necrotizing the bone. 13,24,25 We were able to observe the degree of safety while using the Er,Cr:YSGG laser without traumatizing the bone tissues. Moreover, the use of laser was conveniently easy, because the tip of the laser applicator did not have to be parallel to the axis of the dental implant, contrary to the trephine bur, which demands the pathway of the bur to be parallel to the axis of the implant.
The amount of bone ablated while removing the implants was less in the Er,Cr:YSGG laser group than in the trephine group, with a mean difference of 0.217 cm3. The reason behind this can be attributed to the thermomechanical ablative mechanism of the laser, in which only the bone that is in contact with the implant is removed, creating a gap between the implant and the adjacent bone tissues. This is unlike the conventional method with the trephine bur, which results in a larger amount of bone loss, because it mechanically cuts the bone surrounding the implant and removes it as an en bloc specimen.
SEM observations have shown precise, regular borders without any signs of thermal damage in the tissues ablated with the Er,Cr:YSGG laser. Similar findings were presented by Kimura et al., 10 who also did not observe any melting or carbonization after irradiating bone with Er,Cr:YSGG (power 5 W, repetition rate 8 Hz with water and air spray). Further, Romeo et al., 8 who have tested the effect of the Er:YAG laser, confirmed the safely of the 2940 nm wavelength on bone tissues.
The presence of microirregularities on the bone surface is caused by the strong subsurface pressure, which caused explosive removal of the tissue in contact. Controlling the extent of these microexplosions is based primarily on the laser pulse duration. Shorter pulse durations provide a more precise ablation with less thermal transfer to the surrounding tissue, making the Er,Cr:YSGG laser the best choice for hard tissue ablation procedures. 26
The SEM observations of the bone tissue prepared by the trephine bur have shown abnormal spherical formations on its surface. This might be a result of the rapid increase of temperature during cutting, followed by the sudden decrease of temperature caused by the integrated cooling system of the hand piece.
During the experiment, one of the laser applicator tips broke during the implant removal. This incident brought to our attention the financial aspect of using laser devices and the burden it might add to the cost of the procedure, which should be taken into consideration when choosing any surgical method.
Previous reports claimed that the main disadvantage of using the erbium lasers in dental procedures is the prolonged operation time. 27 Although we have observed a difference between the laser and the conventional methods regarding the duration of ablation, with a mean difference of 27.2 sec between the two groups, all operations in both groups were completed in <1 min (chair-side time). This allows us to conclude that even though the use of laser devices might slightly prolong the procedure time, it is unlikely to be significant in the clinical practice, and can be strongly justified with the benefits of the laser technology in terms of safety and precision.
Conclusions
From this in vivo study, it can be concluded that the use of Er,Cr:YSGG laser for removal of failed osseointegrated dental implants is more efficient and precise and considerably safer to the bone, as well as being more versatile in critically accessible regions than the conventional mechanical technique.
Footnotes
Acknowledgment
The authors thank Dr. Frank Hölzle from the Department of Oral and Maxillofacial Surgery of the University Hospital – RWTH, Aachen, for his helpful contribution.
Author Disclosure Statement
No competing financial interests exist.