
Abstract
Introduction
C
The new field of cell-based therapy offers a supplementary mode of treatment, in addition to coronary reperfusion, in patients post-MI by replacing dysfunctional myocytes and improving heart function. 2 –4 Extensive efforts have been made in developing cell-based therapies to promote tissue repair through the introduction of exogenous cells, such as bone-marrow–derived mesenchymal stem cells (BM-MSCs), as reflected in studies in animal models and recent clinical trials. 5 –8 Some of the hypothesized mechanisms behind the effect of these cells include the secretion of paracrine factors, stimulation of neovascularization, and activation of cardiac regeneration through recruitment of stem cells or proliferation and transdifferentiation of transplanted stem cells. In clinical trials, cells were mainly derived from bone marrow (BM) origin but also from adipose tissue, cardiospheres, and CD34+ cells. 6 –10 In some recent clinical trials, the cell-based therapy did not translate to improved left ventricular ejection fraction (LVEF) post-MI. 6 –8 One recent study reported improved LVEF when the progenitor cells were from biopsied heart tissue in patients with cardiomyopathy 9 ; however, they revealed either no improvement or only modest improvement in heart function post-MI or cardiomyopathy, following the stem-cells-based therapy. The inconsistency in clinical outcome using various stem cell types demonstrates the need for a better understanding of stem cell therapy mechanisms. Finding the optimal stem cell type or the right combination of stem cells for cardiac cytoprotection and regeneration may be the key toward improving clinical outcome. 7
Low-level laser therapy (LLLT) has been found to modulate various biological processes. 11 –14 In an experimental model of the ischemic/infarcted heart in rats and dogs, it was demonstrated that LLLT application directly to the ischemic area in the heart at optimal power parameters significantly reduced scar tissue formation. 15 –17 The cardioprotective effects of LLLT by direct application to the ischemic heart or cardiomyocytes in vitro have also been demonstrated. 18,19 Furthermore, it was elegantly demonstrated that low power Helium Neon irradiation promotes the proliferation of endothelial cells in vitro and production of vascular endothelial growth factor (VEGF). 20 In another study, expression of proangiogenic genes was enhanced in cardiomyocytes by application of LLLT. 21 There are also several reports on the effects of photobiostimulation on stem cells or progenitor cells. LLLT application to normal human neural progenitor cells significantly increased adenosine triphosphate (ATP) production in these cells. 22 LLLT delivery to mesenchymal stem cells (MSCs) in vitro caused a significant enhancement in their proliferation rate, and also increased the proliferation rate of adipose-derived stem cells in vitro. 23 –25 Recently, it was demonstrated that LLLT application to autologous BM can induce proliferation and recruitment of MSCs to the infarcted rat heart and markedly reduce scarring, as well as inducing cardiogenesis along the border line of the infarcted area. 26 –28 The aim of the present study was to evaluate the cardioprotective effect of induction of autologous BM stem cells by LLLT, and its effects on heart function in the infarcted porcine heart following MI and reperfusion.
Methods
Animals
Farm pigs (3–4 months old, 35–40 kg) were used. They were housed in a controlled environment in the Preclinical Research Unit of Assaf Harofeh Medical Center (Zrifin, Israel). The experiment was approved by the Committee for Animal Care of the Preclinical Research Unit of Assaf Harofeh Medical Center.
Experimental protocol
Echocardiography (ECHO) was performed with the animals under anesthesia prior to any surgical procedure, to ensure healthy heart contraction and a minimum LVEF of 50%. Myocardial infarction (MI) was induced by balloon catheterization inserted in the middle of the left descending coronary artery (LAD) segment between first and second diagonal and inflated for 90 min. The pigs were continuously monitored with an electrocardiogram (ECG), and for oxygen saturation and blood pressure. Immediately post-reperfusion, ECHO was performed to assess the myocardial injury. The laser-treated (LT) or control [sham-operated, non-laser-treated (NLT)] pigs were randomly selected post-balloon inflation (induction of MI). ECHO was performed.
Blood samples for troponin I, creatinine phosphokinase (CPK), and antioxidants in the blood were collected before MI, 3 and 5 h post-MI, and then daily for 7 days. Fresh whole blood samples were collected for cell characterization by fluorescent activated cell sorting (FACS) before MI, 3 and 5 h post-MI, and then daily for 7 days. Serum was prepared from fresh blood and stored immediately at −700C in small aliquots for determination of troponin-I, CPK and total antioxidants. Pigs were euthanized at 90 days post-MI.
LLLT application
Preliminary experiments on fresh bones of the farm pigs were conducted to determine the optimal transmission of laser power through bones, and also to characterize the histology in various areas of the tibia and ileum in order to find the areas in the BM that were enriched with mononucleated cells (MNCs) probably also containing stem cells. Most of the areas in the ileum were found to be enriched with the MNCs, whereas in the tibias, cells were found close to the proximal end of the bone. Therefore, the location of laser application was chosen at the flat mid portion of the ileum and the proximal part of the tibia. Ga-Al-As diode laser (Thore Photomedicine Ltd., England) 808 nm was used, equipped with a rigid fiberoptic (8 mm diameter). The LT or NLT pigs were randomly selected post-balloon inflation (induction of MI).The laser was applied in each pig at each time point in both tibias (right and left) and in one side of the iliac bone. The application to one side of the iliac bone was chosen in order to avoid muscle injury to both sides that could cause the pig difficulty in walking or standing. At the following time point (2 days post ML) laser was applied to the contralateral side of the iliac bone. In order to expose the sites in the bones for contact with the distal tip of the fiberoptic laser, surgical incisions were made in each hind leg, ∼2 cm distal from the knee, to expose the proximal part of the tibia. An additional incision was made in the gluteus muscle on one side to enable insertion of the rigid fiberoptic through the muscles to full contact with the iliac bone. Laser was applied by contact of the distal tip with the exposed and external side of the tibia or iliac bones (noninvasive to the bone). The laser was set at a power output to deliver an optimal power density of 10 mW/cm2 to the BM tissue (cells). This optimal power density was chosen based on the ability to reduce scarring post-MI in a similar experimental model in rats 26 and also based on previous studies. 13 –15 Laser was delivered each time for 100 sec (1 J/ cm2). Preliminary experiments were performed with a fresh bone to determine the transmission of the laser through the bones at the specific site, in order to set the power output of the laser (see previous study 26 ). Laser was applied 30 min, 2 days, and 7 days post-induction of MI. The 30 min time point was chosen to mimic, in part, the clinical situation (patient admission after MI occurrence), but not to apply the laser too long after MI, so that the laser effect could be minimal in this costly experimental model. The time points of 2 and 7 days were chosen to enhance angiogenesis, 15,26 and to attenuate initial scaring (7 days post-MI). Control NLT pigs were treated similarly, but the laser was not turned on.
Infarct size
Pigs were euthanized 90 days post-MI. Hearts were excised, and 1 cm thick transversal slices were prepared and incubated in triphenyl tetrazolium chloride (TTC) stain at 37°C for 15 min to stain viable heart muscle with red and the scar tissue with light yellow. Slices were then scanned and the scans were processed for determination of the volume of scarring (in %) out of the total volume of the left ventricle (defined here as infarct size) using Sigma Scan software imaging. The extent of scarring (infarct size) was analyzed by two different observers who were blinded to whether the pigs were LT or NLT, and the results were averaged (variability between the two observers did not exceed 10%). Samples from the infarcted area were excised and further processed for histological examination, to evaluate correlation with TTC staining.
Histology and immunostaining
Density of small blood vessels (up to 100 μm diameter) was determined in histological sections for LT and NLT pig hearts in the infarcted area, as described by us previously. 24 Measurements were taken from six random samples in each of the three histological sections that were randomly taken from the infracted area in each pig. In addition, von Willebrand immunostaining was performed using anti-von Willebrand factor (Millipore Inc., CA, USA) according to manufacturer's instructions. Immunostaining for α-smooth actin on the histological section of the infarcted area was performed using sarcomeric actin monoclonal antibody (Covance Inc., NJ, USA) according to the manufacturer's instructions.
ECHO and MRI
The Ultrasound unit “MyLab 30vet” (Esaote Inc.) was used for ECHO. The transducer used for scanning was phased array 2.5–3.5 MHz (PA 230E) with cardiology software. ECHO was performed on all pigs at 2 h and 6 weeks post-MI. For MRI, a Siemens 3 Tesla unit was used. MRI was performed on 2 LT and 2 NLT pigs prior to euthanasia.
Results
At 24 h post-MI, the level of troponin I in the blood was significantly lower (p < 0.005) in the LT pigs than in the NLT ones (Fig. 1). At 48 h, the troponin I levels were similar in the blood of both LT and NLT pigs. Accumulation of CPK in the blood up to 24 h post-MI was significantly lower [51% (p < 0.05)], in the LT pigs than in the NLT pigs (Fig. 2). Total antioxidant levels in the blood were significantly higher [3.6- and 1.2-fold (p < 0.01 and p < 0.05, respectively)], in the LT pigs than in the NLT ones at 4 and 48 h post-MI, respectively (Fig. 3). At 24 and 96 h post-MI, there was no difference in the total quantity of antioxidants in the serum between LT and NLT pigs.
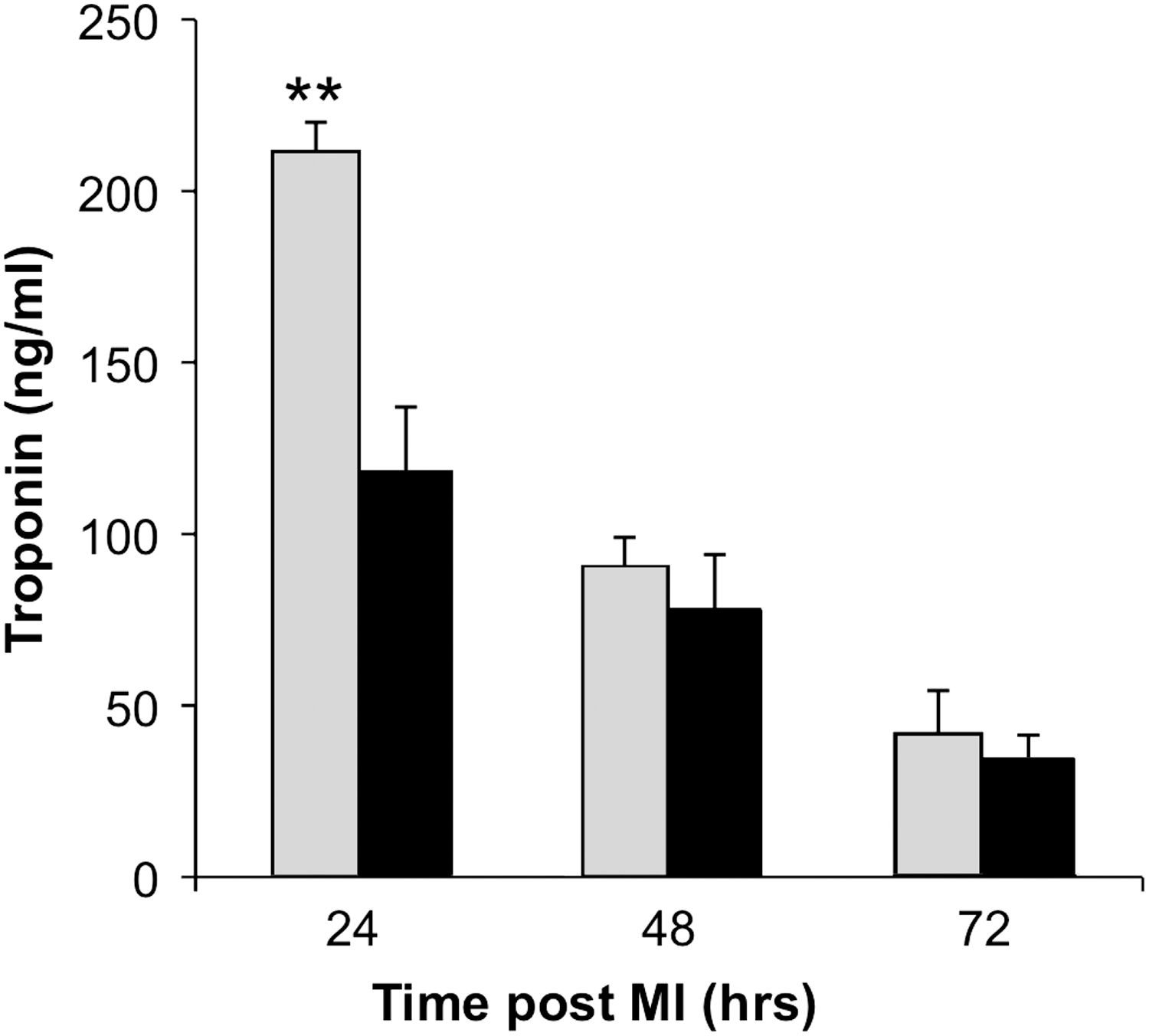
Levels of troponin I in serum of non-laser-treated (gray columns) and laser-treated (black columns) pigs at different time intervals post-myocardial infarction (MI). Results are mean ± SEM of four or five pigs in each group. **p < 0.01.

Creatinine phosphokinase (CPK)_accumulated (area under curve) activity of non-laser-treated (NLT) (gray columns) and laser-treated (LT) (black columns) pigs at different time intervals post-myocardial infarction (MI). *p < 0.05.
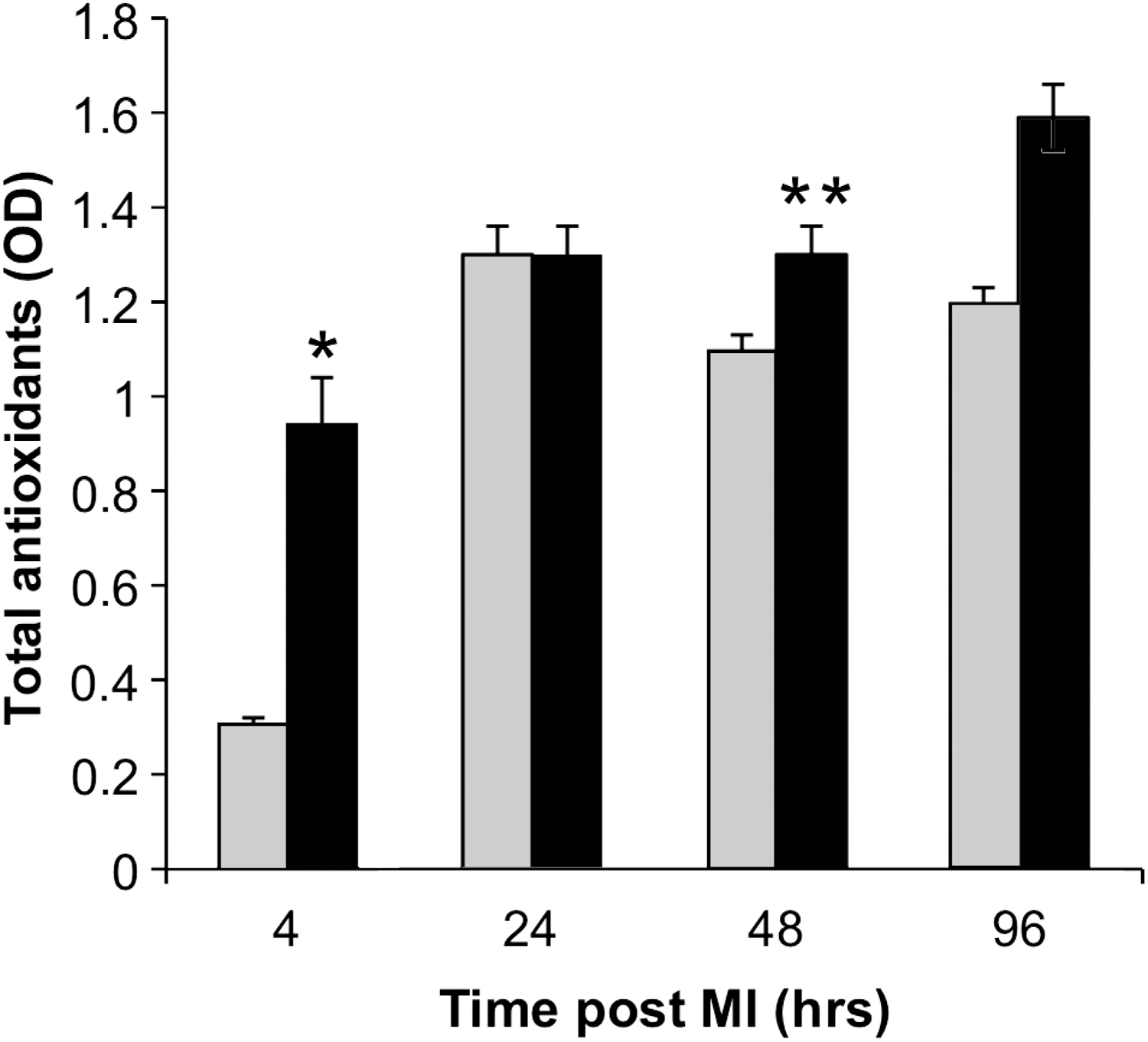
Levels of total antioxidants in serum of non-laser-treated (NLT) (gray columns) and laser-treated (LT) (black columns) pigs at different time intervals post-myocardial infarction (MI). Results are mean ± SEM of four or five pigs in each group. *p < 0.05; **p < 0.01.
Figure 4 presents the FACS analysis for the percentage of macrophages in the circulating blood (out of the total MNCs in the blood). There was a 2.6-, 5.8-, and 3.5-fold higher density of macrophages at 24, 48, and 72 h post-MI, respectively, in the NLT pigs than in the LT pigs, demonstrating a nonstatistically significant (caused by high variability) trend of lower levels of macrophages in the circulating blood because of the LLLT to the BM. In the NLT pigs there was an increase in cell density of macrophages in the circulating blood of 2.2- to 3.8-fold compared with their density in the blood before the induction of MI. This was not the case in the LT pigs, in which macrophage density in the blood did not significantly differ from its level prior to MI and up to 72 h post-MI. FACS analysis of c-kit+ cells in the circulating blood showed significantly higher (p < 0.05) four and twofold levels in the LT group than in the NLT group at 24 and 48 h post-MI, respectively (Fig. 5). The infarct size (% of scar tissue out of the LV volume as measured from histology) in the LT pigs was 5.2 ± 0.82%, which was significantly lower [68% (p < 0.05)] than the infarct size (16.6 ± 3.7%) in the NLT pigs (Figs. 6 and 7). The histology of the interphase between the intact myocardium and the infracted area revealed a typical scaring in the NLT pigs (Fig. 8). However, in the LT pigs, the interphase area was characterized by scaring and cardiomyocytes that intermingled between the collagen with numerous capillaries (Fig. 8). The MRI scans of some of the pigs revealed a greater scarring in NLT pigs than in LT ones (Fig. 9).
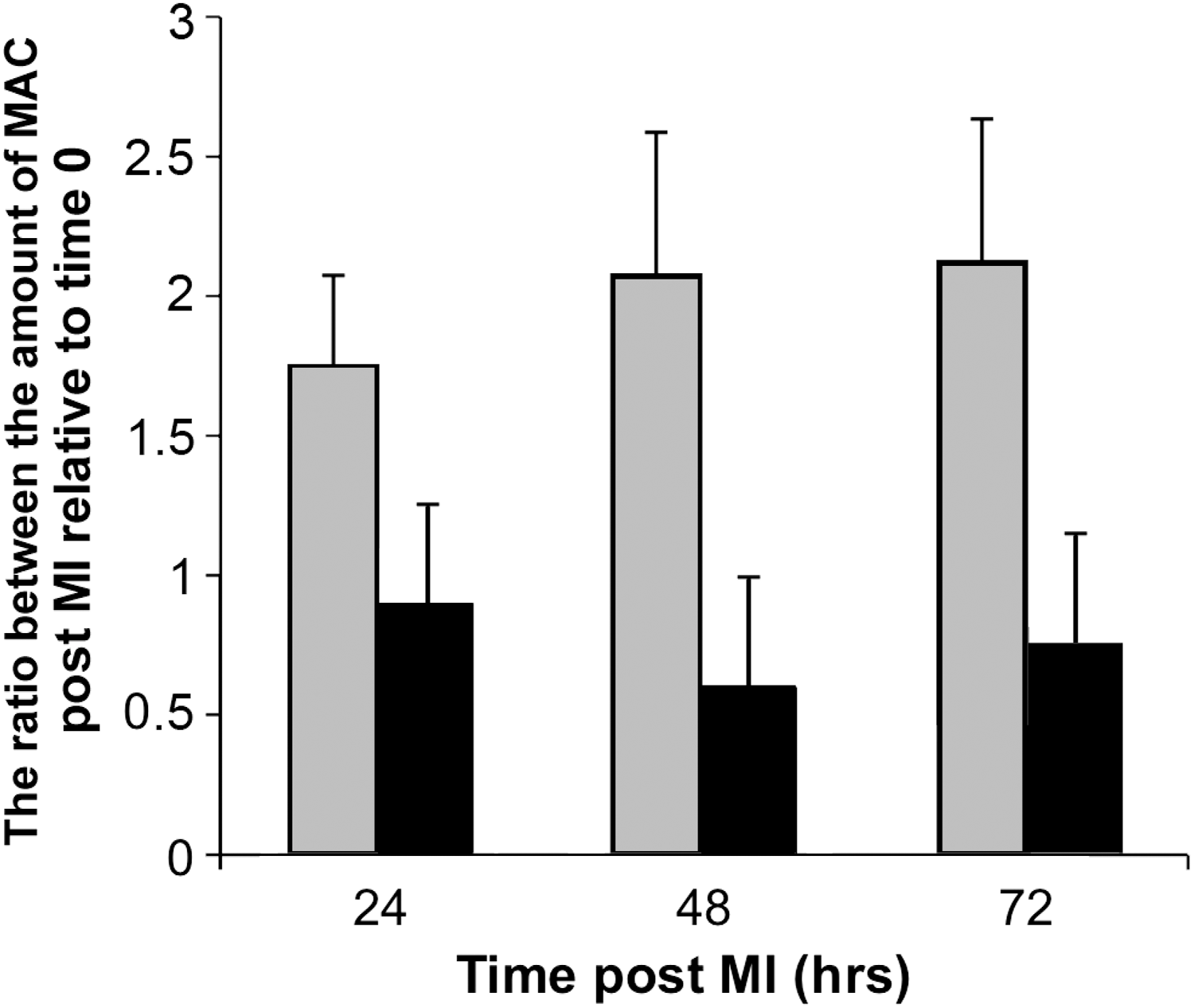
The ratio between the amount of macrophages (MAC) in the circulating blood of non-laser-treated (NLT) (gray columns) and laser-treated (LT) (black columns) at time 0 (before MI) and at different time intervals post-myocardial infarction (MI). Results are mean ± SEM of four or five pigs in each group.
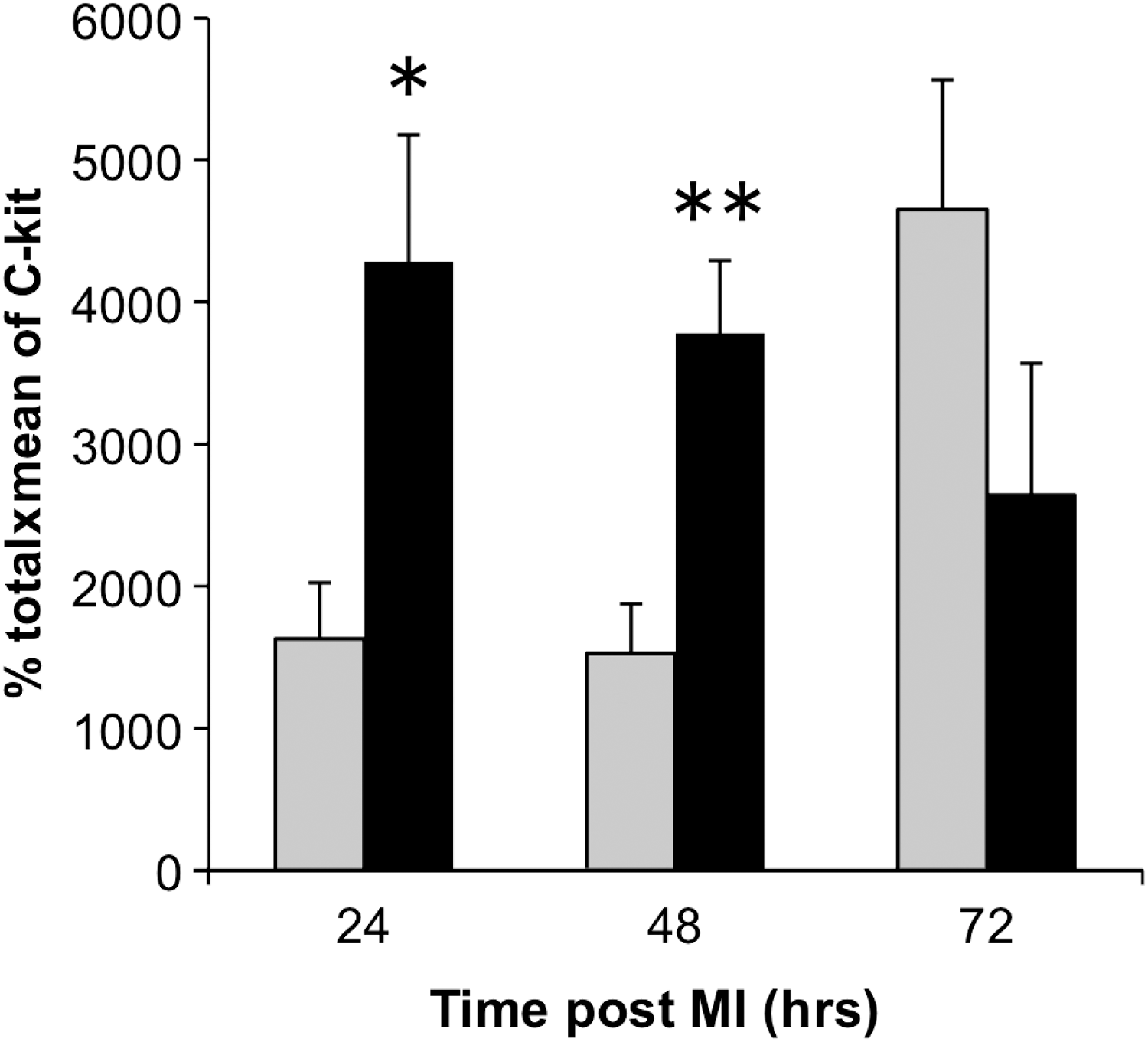
C-kit+ cells levels in circulating blood of non-laser-treated (NLT) (gray columns) and laser-treated (LT) (black columns) pigs at different time intervals post-myocardial infarction (MI). Results are mean ± SEM of four or five pigs in each group. Score of the cells is calculated as % of c-kit+ cells out of the total number of mononuclear cells in the serum multiplied by the mean fluorescence of the cells. *p < 0.05; **p < 0.01.
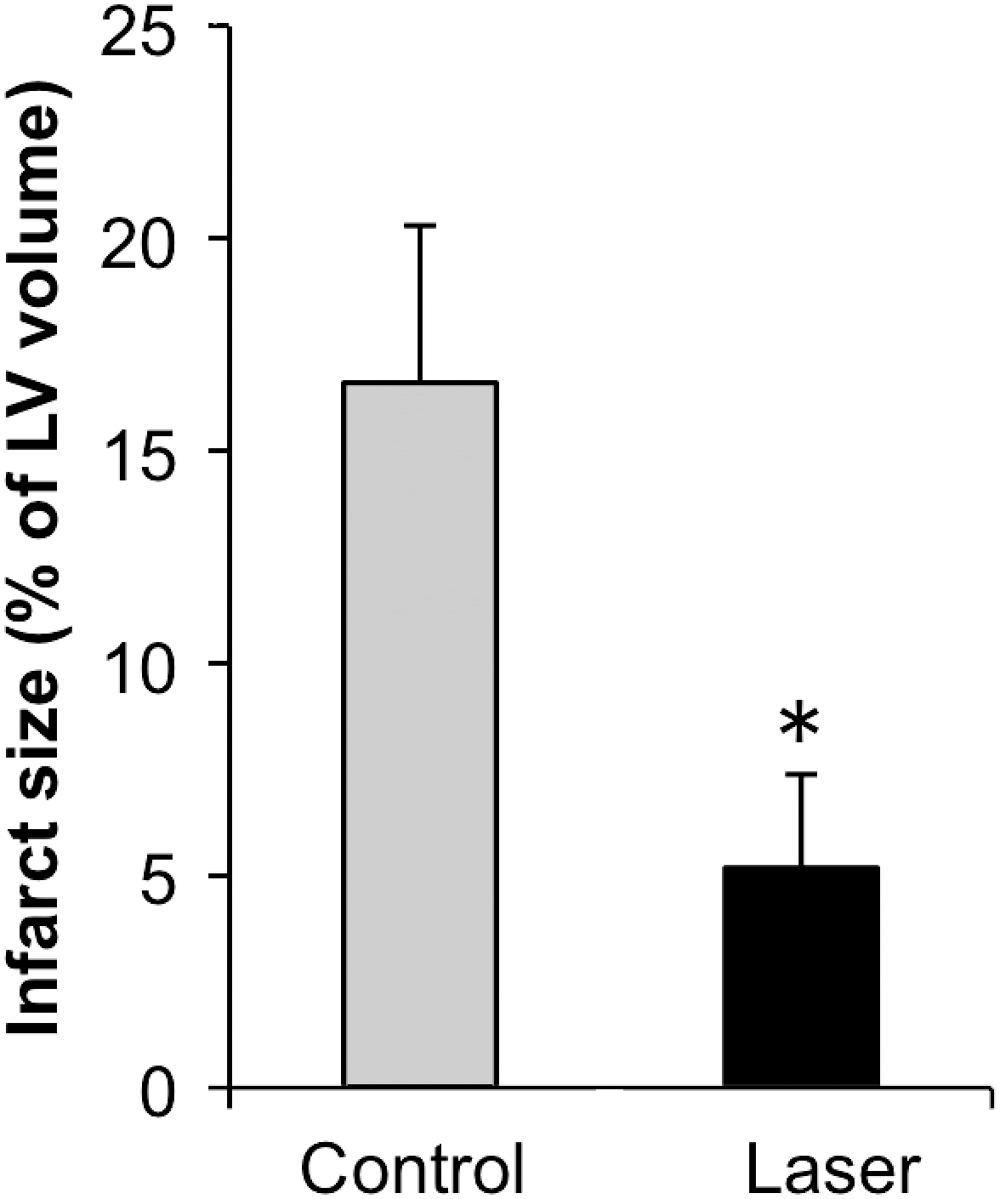
Infarct size (% of left ventricular volume) of non-laser-treated (NLT) (gray columns) and laser-treated (LT) (black columns) pigs 3 months post-myocadial infarction (MI). Results are mean ± SEM of five pigs in each group. *p < 0.05.

Representative triphenyl tetrazolium chloride (TTC) stained transverse slices from non-laser-treated (NLT) and laser-treated (LT) porcine heart 90 days post-myocardial infarction (MI). Note a large infracted areas (arrows) in the NLT pigs relative to small infracted areas in the LT ones. Scale = 2 cm.
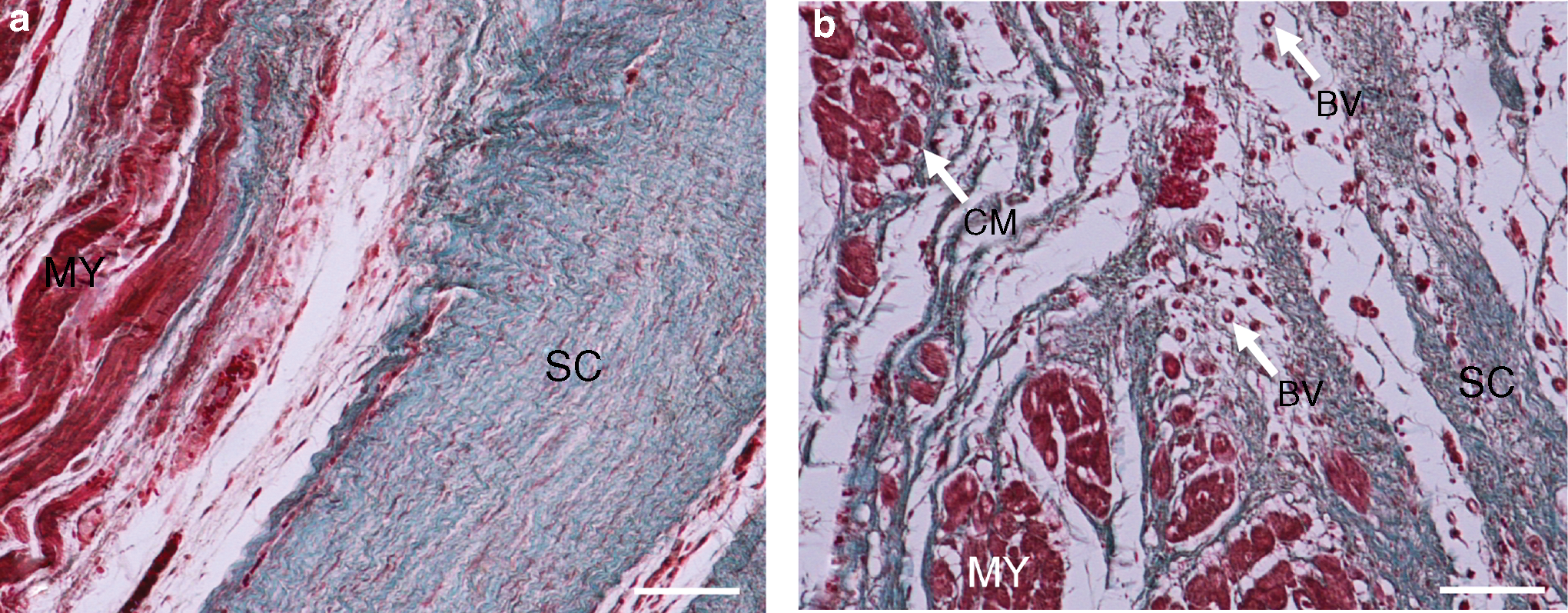
Representative histological micrographs of infracted areas in non-laser-treated (NLT)

Representative MRI scans of non-laser-treated (NLT)
In the control NLT pigs, 6 out of the 14 animals died (43% mortality). Five of them died within 3 h post-induction of MI, and one died between 12 and 20 h post-MI. Of the LT pigs, all six survived post-MI (0% mortality). Fisher's exact test for mortality between the NLT and LT groups showed no significant difference (p = 0.14) in mortality between groups.
The density of c-kit+ cells in the infarcted area of the LT pigs 90 days post-MI was significantly higher [4.8-fold (p < 0.003)], than that in the NLT ones (Fig. 10). The mean density (number per mm2) of small blood vessels was 13 ± 4.0 in the LT pigs, which was significantly [6.5-fold (p < 0.025)] higher than the value (2.2 ± 0.7) in the NLT ones (Fig. 11). The results from using Von Willebrand antibodies to detect newly formed blood vessels revealed the blood vessels density (number per mm2) in the infarcted area to be 0.89 ± 0.19 in the NLT pigs and 1.08 ± 0.14 in the LT ones. There was no statistical difference between the two groups. The histology (Fig. 12) and quantitative results of the density of α-sarcomeric actin positive cells in the infarcted area demonstrated a significantly higher (p < 0.01) density (cells per mm2) of α-sarcomeric actin positive cells in the LT pigs (78 ± 5) compared with their density in NLT pigs (59 ± 3).
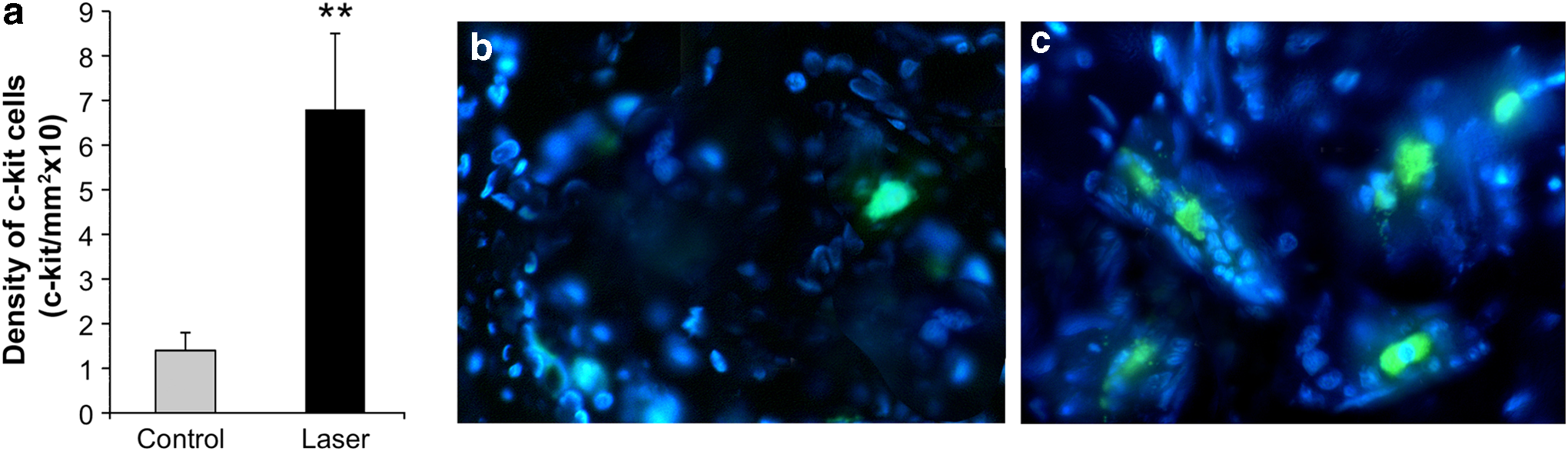
Density (number per area) of c-kit+ cells in the infarcted area of non-laser-treated (NLT) (open columns) and laser-treated (LT) (solid columns) pigs at 90 days post-myocardial infarction (MI). Results
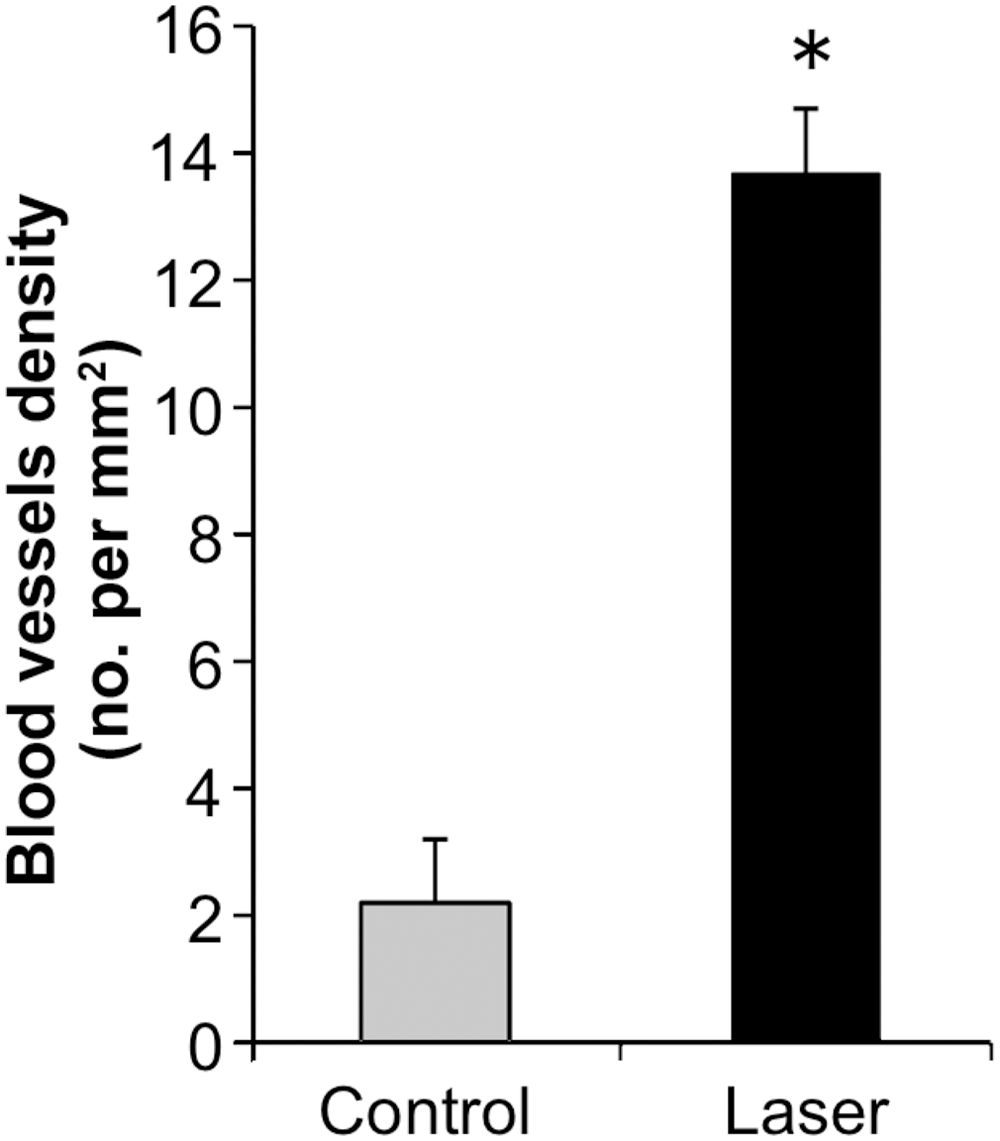
Density of small blood vessels in the infarcted area of non-laser-treated (NLT) (gray column) and laser-treated (LT) (black column) pigs at 3 months post-myocardial infarction (MI). Results are mean ± SEM of random histological sections of the infracted area in the hearts as detailed in the Methods section. *p < 0.05.
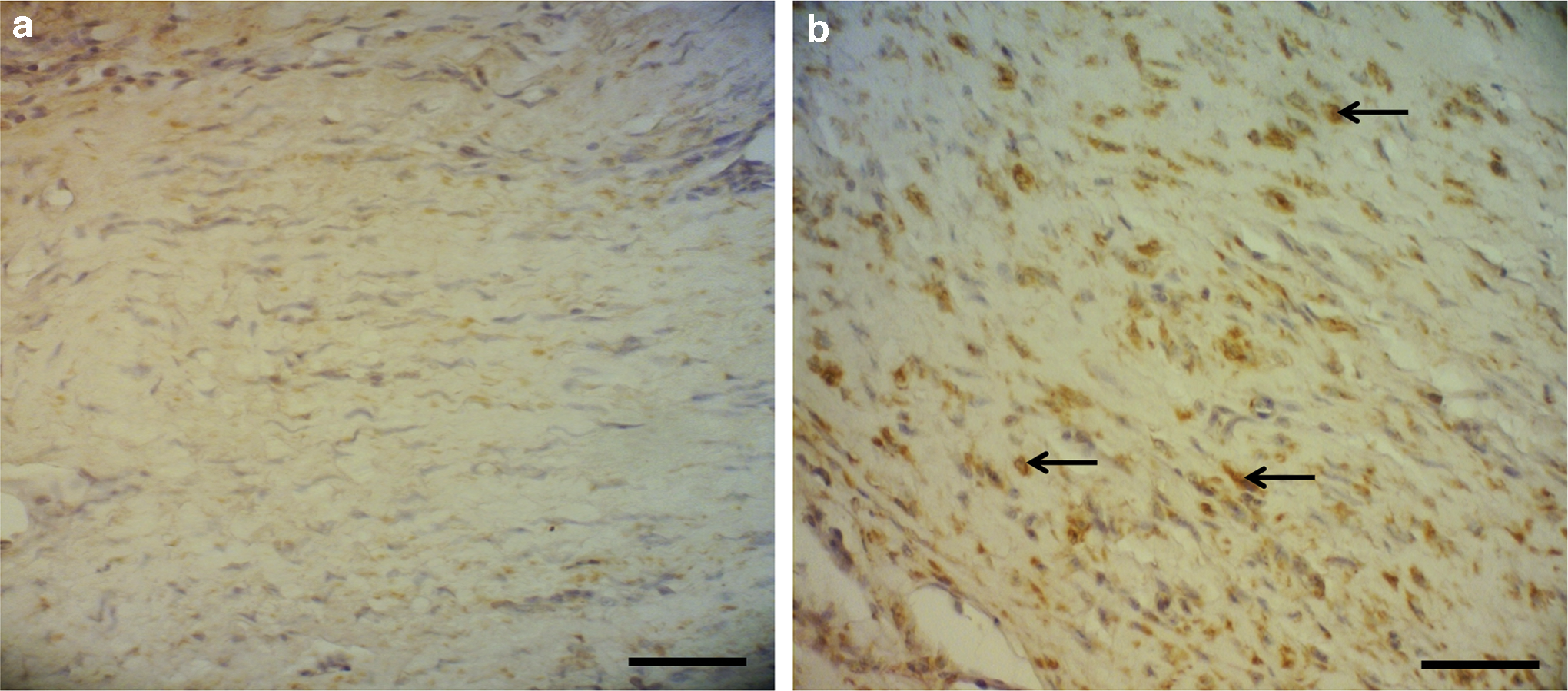
Representative micrographs of α-sarcomeric actin immunostaining of histological sections of the infracted areas in the myocardium of non-laser-treated (NLT) and laser-treated (LT) pigs. Note that there are more stained cells in the sections taken from the LT pigs in
The LVEF and fractioning shortening (FS) prior to MI did not statistically differ between the pigs that were later assigned either to LT or NLT (Table 1). At 2 h post-MI, LVEF and FS of the LT pig hearts were significantly higher [19 and 33% (p < 0.05)], than in the NLT pig hearts, respectively. The same trend was also observed at 6 weeks post-MI, when the LVEF and FS were significantly higher (16% and 27%, respectively) in the LT pigs than in the NLT ones (Table 1).
p < 0.05 and ** p < 0.01 represent level of statistical differences between NLT and LT pig values at a certain time interval.
LVEF, left ventricular ejection fraction; LT, laser-treated; NLT, non-laser-treated; ECHO, echocardiogram; MI, myocardial infarction.
Discussion
The results of the present study clearly demonstrate that LLLT to the BM in the porcine model has beneficial effects on the ischemic heart post-MI both at the acute phase and long term phase. The results from the blood markers (troponin I and CPK) revealed a significant reduction in the LT compared with the NLT pigs and were in accordance with the reduction in scarring, indicating an initial cardioprotective effect of the laser treatment. The significant fourfold higher content of total antioxidants detected already at 4 h post-MI in the LT pigs compared with the NLT ones, may also contribute to the cardioprotection in the ischemic myocardium post-MI. In a previous study, we demonstrated an inverse correlation between levels of catalase (antioxidant) in the blood 24 h post-MI, and the infarct size in dogs 30 days post-MI. 15 The cardioprotective effect of the LLLT to the BM already at early stages post-MI may also be associated with the higher rate of survival of those pigs compared with the NLT ones, as was found in the present study. The cardioprotective effect of LLLT to the BM was also associated with the significantly improved LVEF and FS observed in the LT pigs already at 2 h post-MI. The above-described results corroborate previous studies demonstrating the cardioprotective effects of LLLT to the ischemic myocardium. 18,19
The long-term beneficial effect of LLLT to the BM was evidenced by the significant (p < 0.05) reduction of 68% in the extent of scarring post-MI following laser treatment to the BM. These results corroborate our previous studies in the rat infracted model in which we also demonstrated a marked reduction in scarring caused by LLLT application to autologeous BM. 26 –28 It may be postulated that LLLT may have induced various types of cells concomitantly in the BM, which could cause an increase in their number in the circulating blood following their enhanced proliferation in the BM. These photobiostimulated cells can then, to a certain extent and under certain circumstances, home in on the ischemic zone in the ischemic organ (i.e., the heart). We have shown in previous articles that LLLT to the BM significantly stimulates the proliferation of stem cells. 26
The higher content of macrophages in the blood of the NLT pigs compared with the LT ones during the first few days post-MI may indicate a reduction in inflammatory response post-MI following the LLLT to the BM. The possibility that the laser-induced macrophages homed in to a greater extent on the infarcted myocardium than those in the NLT pigs, and therefore that their percentage in the circulating blood was lower than in the NLT pigs, cannot be ruled out. It was previously demonstrated that macrophages in the infracted myocardium played a significant role in the attenuation of scaring post-MI.
A higher percentage of c-kit+ cells in the circulating blood of the LT pigs than in the NLT ones was also found as soon as 24 and 48 h post-MI, and may indicate a higher rate of proliferation of these stem cells in the BM, and their rapid mobilization to the circulating blood. A significantly higher rate of proliferation of stem cells following LLLT to the BM has been shown by us previously. 26 The finding of a 4.8-fold higher density of c-kit+ cells in the infarcted area of the LT pigs compared with the NLT pigs even at 90 days post-MI may be a result of the enhanced MSC proliferation in the BM post-LLLT treatment that was found previously in the rat infarcted model 26 and also by the higher concentration of c-kit+ cells in the circulating blood of the LT pigs compared with the NLT pigs. Similarly, Hatzistergos et al. 29 found that endogenous c-kit+ cardiac stem cells increased by 20-fold in the porcine infarcted heart model following transcardial injection of BM-derived MSCs compared with in control infracted pigs that did not receive MSC injection. Shintani et al. 30 demonstrated in patients post-MI that the number of MNCs in the peripheral blood increased significantly 7 days post-MI, and thereafter gradually declined up to 28 days post-MI, compared with uninfarcted patients. The number of MNCs in the peripheral blood of these patients post-MI correlated with the quantity of plasma VEGF. Similarly, it can be hypothesized that the MNCs activated by the LLLT in the BM, and which thereafter proliferated at a higher rate, were mobilized to the circulating blood and from there to the infarcted area. The significantly higher density of c-kit+ cells found in the infarcted area of the heart of the LT pigs in the current study lends credence to this hypothesis.
The results of the present study also indicate the promotion of blood vessel formation in the infarcted area of the pig hearts caused by LLLT treatment of their BM. This was reflected both in the significantly (6.5-fold) higher blood vessel density and also in the trend of more Von Willebrand positive-stained endothelial cells in the blood vessels in the infarcted area in the hearts of the LT pigs compared with the NLT ones. It is interesting to note that the induction of Von Willebrand factor production by the endothelial cells, as revealed by the immunohistochemical results in this study, continued to be higher (but not statistical different) in the hearts of the LT pigs even 3 months following application of LLLT to the BM. The higher extent of expression of α-sarcomeric actin in cells in the infarcted area of LT pigs compared with NLT ones, as found in the present study, indicates a higher content of newly formed cardiomyocytes in the infarcted area compared with that in the NLT pigs. This could be the result of a larger number of MSCs differentiating to cardiomyocytes in the infarcted area and/or the induction of cardiogenesis caused by the growth factors secreted by the laser-induced MSCs. It was demonstrated recently that LLLT to the BM in the rat model of MI induces cardiogenesis. 28
The functional performance analysis of the hearts according to the ECHO measurement analysis showed significantly improved LVEF and FS in the LT pigs than in the NLT ones at 6 weeks post-MI. The above-described results corroborate the reduction in scarring and marked elevation of angiogenesis found in the LT pigs relative to the NLT ones. The results from the ECHO analysis also indicated a significant increase in LVEF and FS in the LT pigs as soon as 2 h post-MI. These results can be explained by the cytoprotective effect that occurred during this period of time caused by the rapid increase in antioxidants in the blood of these LT pigs, compared with the NLT pigs. The higher antioxidant levels in the circulating blood may act to reduce the amount of superoxide in the myocardium following balloon deflation at 90 min post-MI. Consequently, this led to a better salvage of the myocardium and hence better performances of EF and FS of the LV in the LT pigs than in the NLT pigs. The LVEF and FS in the LT pigs still remained significantly (16% and 27%) higher than in the NLT pigs, respectively, at 6 weeks post-MI, indicating the beneficial effects of LLLT for the ischemic heart.
Clinical relevance
Our current study also has direct clinical relevance. The laser can be applied noninvasively to the BM of the pelvic girdle, tibia, or other parts of the skeleton containing BM. However, in the present experimental model, we applied the laser invasively through the muscles to ensure proper laser power delivery. In a clinical situation, where a noninvasive approach may be preferable, proper measurement should be done in human skin, muscles, and bones in order to calculate the transmission of the laser from the surface of the skin to the BM. The novel approach presented in this study, of the use of stem cells for cell therapy to the infarcted heart, avoids the need to isolate stem cells, grow them in vitro, and inject them back into the patients. It also avoids the massive loss of cells involved in cell implantation/injection caused by insufficient seeding of cells or cell death shortly after implantation. The approach in the present study also overcomes the problem of growing autologeous stem cell cultures, and determining the optimal number of implanted cells and the optimal timing for their delivery post-MI.
Conclusions
In conclusion, to the best of our knowledge we have demonstrated here, for the first time, a novel approach of applying LLLT to autologous BM of the infarcted porcine heart in order to induce the proliferation of stem cells that are consequently recruited to the ischemic heart, leading to a significant cardioprotection of the heart in the acute phase post-MI, marked reduction of scarring, and enhanced functional performance of the heart post-MI.
Footnotes
Acknowledgments
The authors thank Naomi Paz for editorial assistance and Varda Wexler for help with preparation of the figures. This study was supported in part by Johnson and Johnson's Inc., and by Nicolas and Elizabeth Shlezak Super Center for Cardiac Research and Biomedical Engineering.
Author Disclosure Statement
No competing financial interests exist.