
Abstract
Introduction
T
Several studies demonstrate that lasers can be superior in comparison with other techniques regarding their debridement and disinfection properties. 9 –18 However, when inappropriate laser parameters are used, they can produce high thermal increments, negatively affecting the surrounding periodontal tissues. 19–20
Thus, the primordial goal for using lasers in endodontics is to remove the smear layer and to disinfect the root canal system without exceeding a temperature rise of 10°C, above body temperature, for more than 1 min. 21
Wide ranges of temperature analysis have been reported with regard to distinct diode lasers. Gutknecht et al. 22 evaluated the temperature rise in the periodontal surrounding tissues while using a 810 nm diode laser inside the root canal, using output powers of 0.6–1 and 1–1.5 W in continuous wave and 0.6–1 W in chopped mode with 10 msec pulse duration and 10 msec interval. Their results showed that none of the settings has increased the temperature of the surrounding tissues more than 7°C.
Hmud et al. 23 assessed the thermal changes inside root canals and on root surfaces using 940 and 980 nm lasers with 4 W/10 Hz and 2.5 W/25 Hz, respectively, delivered by 200-μm fibers. The maximum temperature rise on root surfaces using these settings was 4°C. The authors of this study concluded that both 940 and 980 nm diode lasers could be safely used in endodontics.
Other studies evaluated the safety, bactericidal effects, and the ability for smear layer removal using erbium lasers in endodontics. George and Walsh 24 measured the temperature changes in teeth apical thirds while applying Er:YAG (4 W/20 Hz) and erbium, chromium: yttrium, scandium, gallium, garnet (Er,Cr:YSGG) (1.25 W/20 Hz) lasers using either conical side emitting or conventional bare fiber tips. Their results showed that, regardless of the fiber types, the temperature elevation was less than 2.3°C. Moreover, this study reported that conical fiber tips could be beneficial by minimizing the risks of thermal injury.
Franzen et al. 25 evaluated the extent of the bactericidal effect of an Er,Cr:YSGG laser with a very low power setting of 0.25 W/20 Hz in the root canal, using both microbiological and scanning electron microscope (SEM) analyses. This report showed that bacterial reduction was significant up to 500 μm deep into dentin, whereas SEM images revealed the absence of smear layer, open dentinal tubules, and no detectable signs of thermal damage.
Martins et al. (2013–2014) 26,27 performed a blind randomized clinical trial by analyzing the efficacy of the Er,Cr:YSGG laser and radial firing tips (RFT)2 (140 μs, 37.5 mJ, 20 Hz) and RFT3 (140 μs, 62.5 mJ, 20 Hz) versus the use of 3% sodium hypochlorite and interim calcium hydroxide paste in necrotic teeth with chronic apical periodontitis. They concluded that for single-rooted and premolar teeth, the laser-assisted protocol could achieve predictable endodontic outcomes.
Finally, Al-Karadaghi 28 investigated the radicular dentin permeability and degree of smear layer elimination comparing the Er,Cr:YSGG laser (1.25 W, 50 Hz, 50 μs, 60% water, and 30% air) and a dual wavelength Er,Cr:YSGG laser (same settings) in combination with a 940 nm diode laser (2 W, chopped mode) through 270 μm RFTs. Scanning electron micrographs of dual wavelength group showed a distinctive removal of smear layer, and dye penetration was significantly higher than that of the Er,Cr:YSGG laser group. They also suggested that the use of RFTs removes the smear layer in more homogenous pattern.
Aim
The aim of this study was to detect the temperature changes on root surfaces during the use of a dual wavelength laser (940 and 2780 nm) within the same endodontic protocol to combine the deep disinfection potential of near IR radiation at 940 nm with the cavitation abilities of the Er,Cr:YSGG laser for smear layer removal.
Material and Methods
Sample selection
This study used 18 human single-rooted teeth extracted for periodontal or orthodontic reasons. The approval to use these teeth for the experiment was obtained from the ethics committee of Iraq's Ministry of Health. Absence of carious lesions, pre-existing root canal treatments, and abnormal root canal anatomy was verified radiographically. The teeth were stored in normal saline containing 0.08% thymol to prevent dehydration and bacterial colonization. Samples were divided into three groups (n = 6), namely A–C. Five teeth per group were selected for the temperature measurements and one sample from each group was used for SEM examination.
Sample preparation
All crowns were dissected at the cemento–enamel junction; patency was verified with an ISO #8 K-file. The root canals were prepared and enlarged through a reciprocating technique (Reciproc; VDW GmbH, Munich, Germany) up to an ISO #0.25/0.08, with the working length 1 mm shorter than the root length. To simulate the clinical situation during laser procedures, the samples were embedded in a two-component polyurethane cast resin (ISO-PUR K 760), having a thermal conductivity (0.6 W/m K) similar to that of bone (0.58–1.2 W/m K). 29
Laser parameters and protocols
The laser setup for the first group was an Er,Cr:YSGG laser (1.25 W, 25 mJ, 50 Hz, 50 μs pulse duration, 50% water, and 30% air spray) without any adjunct diode laser irradiation. The laser setup for the second group consisted of an Er,Cr:YSGG laser whose pulses were alternated with pulses of a 940 nm diode laser operating with a duty cycle of 0.2 (pulse duration to pulse period ratio = 20%). The third group used an Er,Cr:YSGG laser whose pulses were alternated with those of the 940 nm diode laser with a duty cycle of 0.5 (pulse duration to pulse period ratio = 50%).
RFTs; Biolase with 25 mm in length and 275 μm diameter (RFT2) were used. Each RFT was introduced inside the root canal, 1 mm short of working length and withdrawn in coronal direction with a speed of 2 mm/sec, performing helicoidal movements. Before each laser round, each canal was irrigated with 2 mL of distilled water at room temperature. All the parameters and protocols for the three Groups A–C are shown in Table 1. The alternating pulses emitted through the same laser tip during the laser device operation are illustrated in Fig. 1.
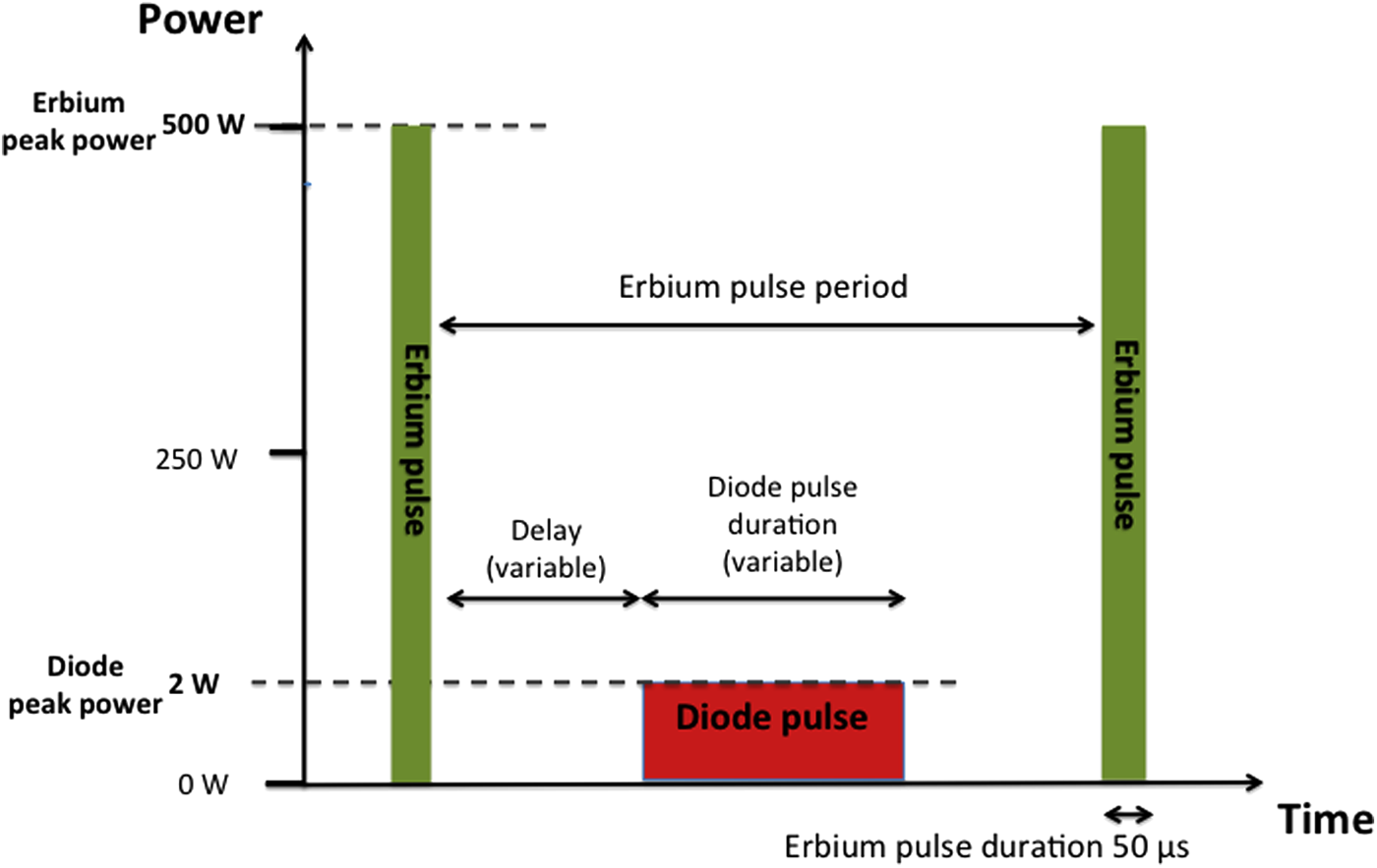
Schematic view of the alternating pulses of Er,Cr:YSGG and 940 nm diode lasers, emitted through one radial firing tip.
W/A, water to air ratio.
Delay, the delay time after Er,Cr:YSGG pulse to start the diode pulse.
RFT, radial firing tip.
Temperature measurements
The temperature measurements were carried out using a digital thermometer (OM-USB-TC, OMEGA ENGINEERING, INC.) and six thermocouples (K-Type, model OMEGA 5TC-TT-36, 0.13 mm in diameter). Three thermocouples were placed on the cervical, middle, and apical thirds of the external root surface, whereas the remaining three thermocouples were placed in 0.5 mm diameter, 1 mm deep holes that were created on the root surfaces. Silicone heat conducting paste (ARCTIC, MX-2) was used to improve heat conduction from the root surface to the thermocouples. Radiographs were taken to verify the correct placement of the thermocouples (Fig. 2). The specimens were immersed in a 37°C thermal bath during laser irradiation. The temperature rises on the external tooth surfaces above the baseline temperature (37°C) were described as delta T (ΔT). The same operator performed the laser irradiation procedures.
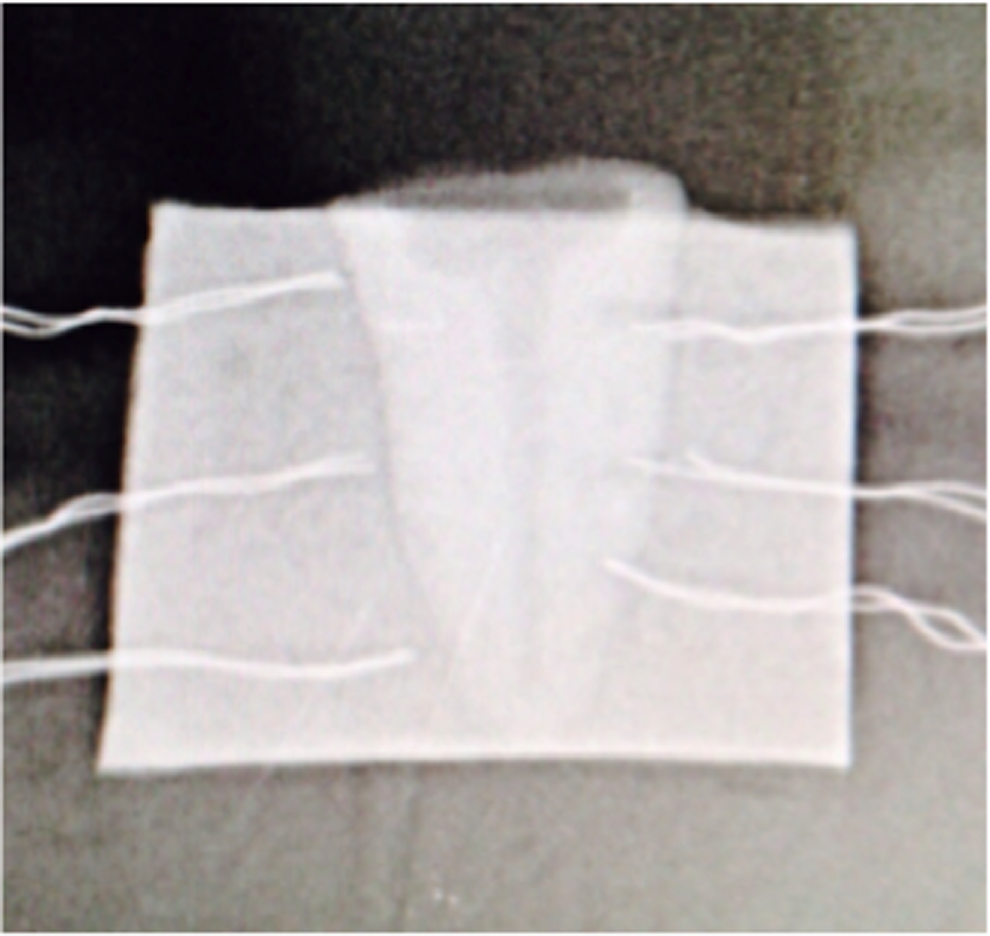
Radiograph showing the position of all thermocouples.
Sample preparation for scanning electron microscope (pilot study)
After laser irradiation and for SEM imaging (XL 30ESEM; FEG Company), the coronal, middle, and apical thirds of one sample from each group were sectioned and examined.
Data analysis
ANOVA and post hoc Tukey tests were used to compare the groups regarding the temperature rise between the three groups as well as differences between the different areas (cervical, middle, and apical) within the same group.
Results
Temperature measurement results
The statistical results of the temperature rises and their distribution between the three groups and within the three different regions (cervical, middle, and apical) are shown in the box-plot graphs, (Fig. 3A–C). Within all groups, the mean temperature rise was highest in the apical thirds followed by the middle and cervical root thirds.

Box-plot graphs showing the results of the temperature rise in the cervical, middle, and apical regions for Groups
The mean, median, standard deviation, minimum, and maximum values of ΔT for Groups A–C in cervical, middle, and apical thirds are shown in Table 2. The mean values of ΔT in different areas (cervical, middle, and apical) within the same group were significantly different (p < 0.001; Table 3). Moreover, the mean values of ΔT between Groups A–C were also significantly different (p < 0.001; Table 4).
In all samples, the recorded thermal changes were below the critical value of 10°C. The highest increase in temperature was measured in one specimen from Group C (8.36°C), which lasted for 10 sec. The highest temperature rises (ΔTMax) of all Groups A–C are expressed in Table 5. A representative example for a single measurement (i.e., from Group C) is shown in Fig. 4.
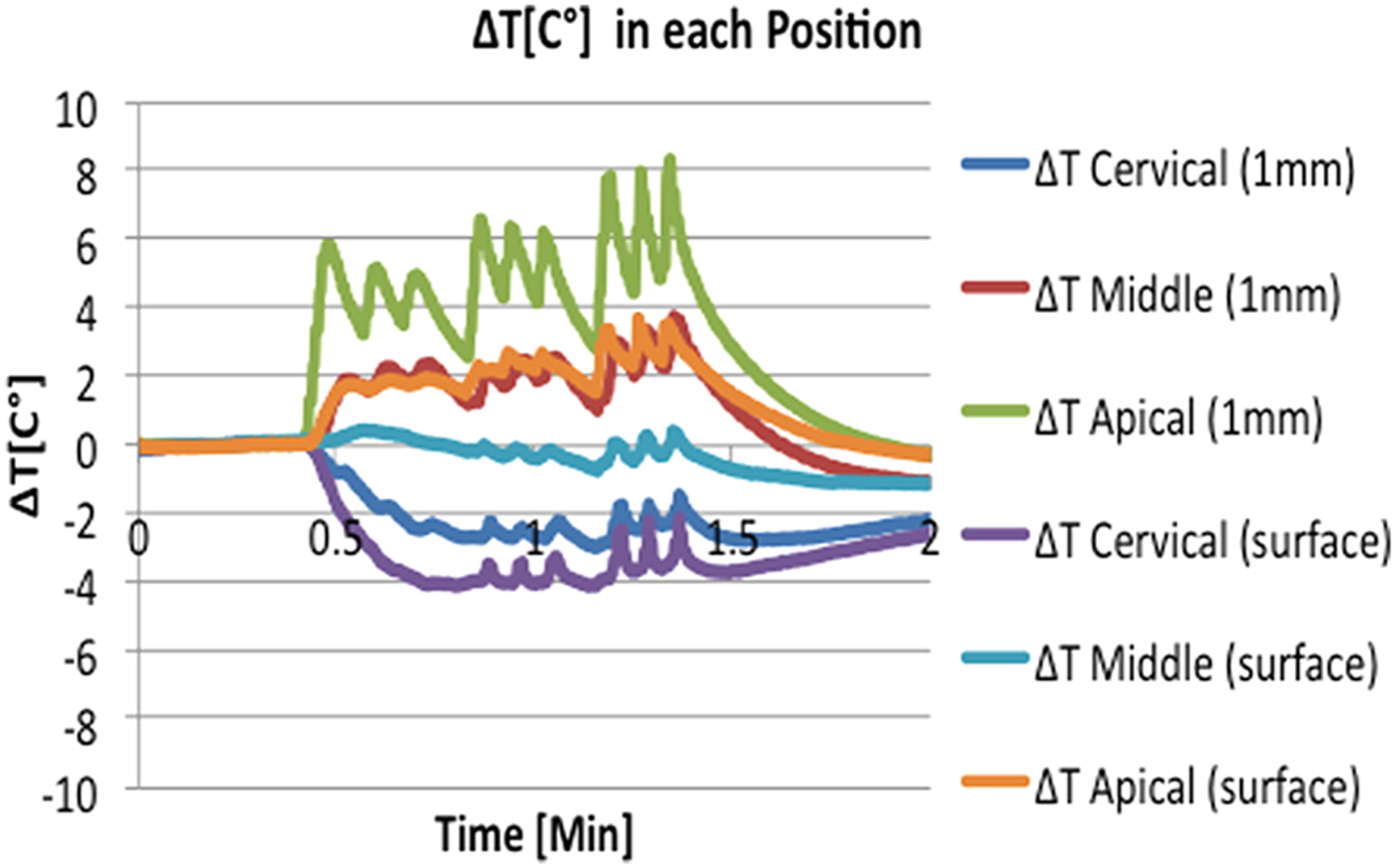
Typical thermal measurement of one specimen in Group C.
Scanning electron microscopy results
SEM micrographs were taken for each third (cervical, middle, and apical) in one specimen from each group. No cracking, fissuring, or sign of thermal side effects were observed in any of these samples.
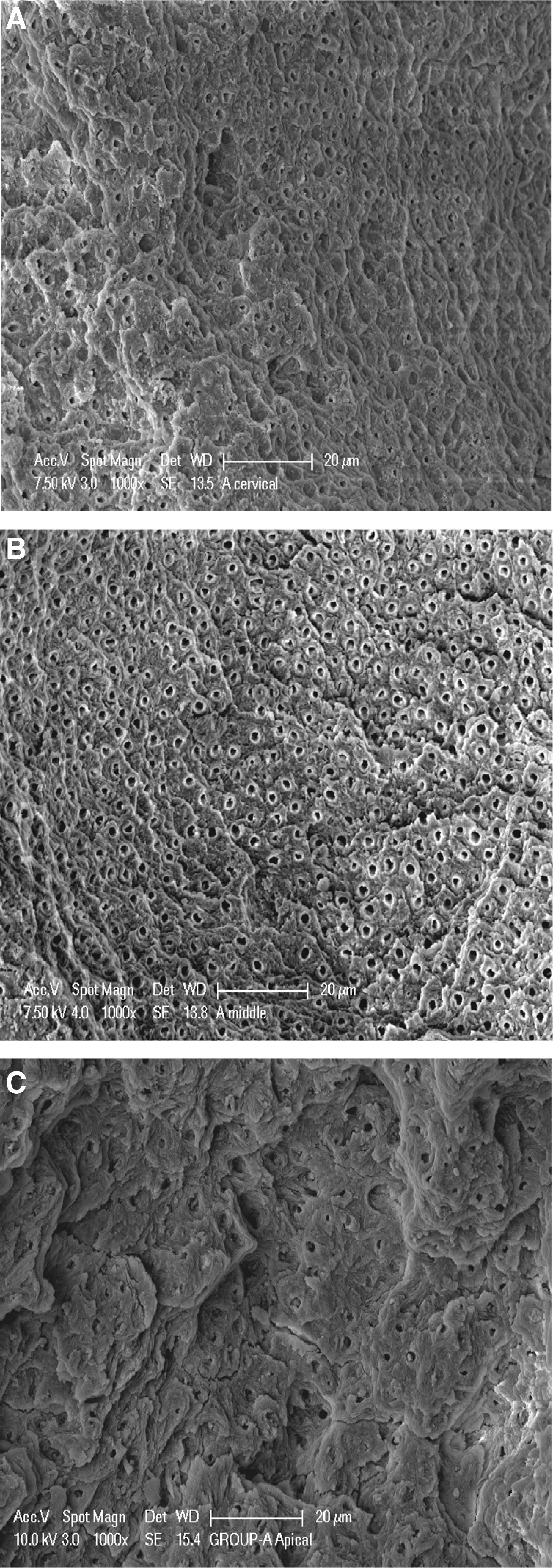
In Group A (Er,Cr:YSGG laser), the smear layer removal and open dentinal tubules could be detected in both the cervical and middle thirds. However, in the apical third, some dentinal tubules were obliterated with smear layer, indicating insufficient debridement in this area (Fig. 5A–C).
In Group B (Er,Cr:YSGG and diode 940 nm 2 W, 20% duty cycle), SEM images did not reveal any significant morphological alteration in comparison with Group A in the cervical and middle thirds (where the ablation pattern was nonhomogeneous) and only partial removal of smear layer could be observed. In the apical third, a heavy smear layer covered the root canal walls and only a small number of open dentinal tubules could be detected (Fig. 6A–C).

In Group C (Er,Cr:YSGG and diode 940 nm 2 W, 50% duty cycle), a uniform smear layer removal along the three areas of the root canal wall (cervical, middle, and apical) could be detected (Fig. 7A–C). The dentinal tubules were completely uncovered and the intratubular dentin was more ablated than the peritubular dentin (Fig. 8).
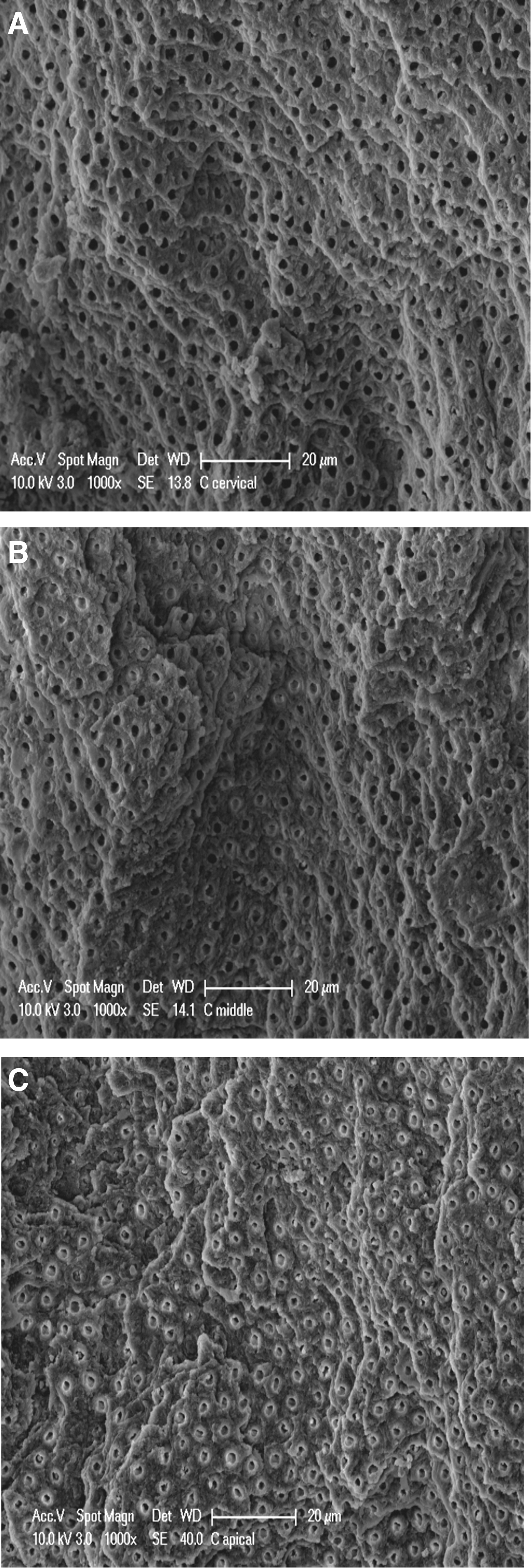
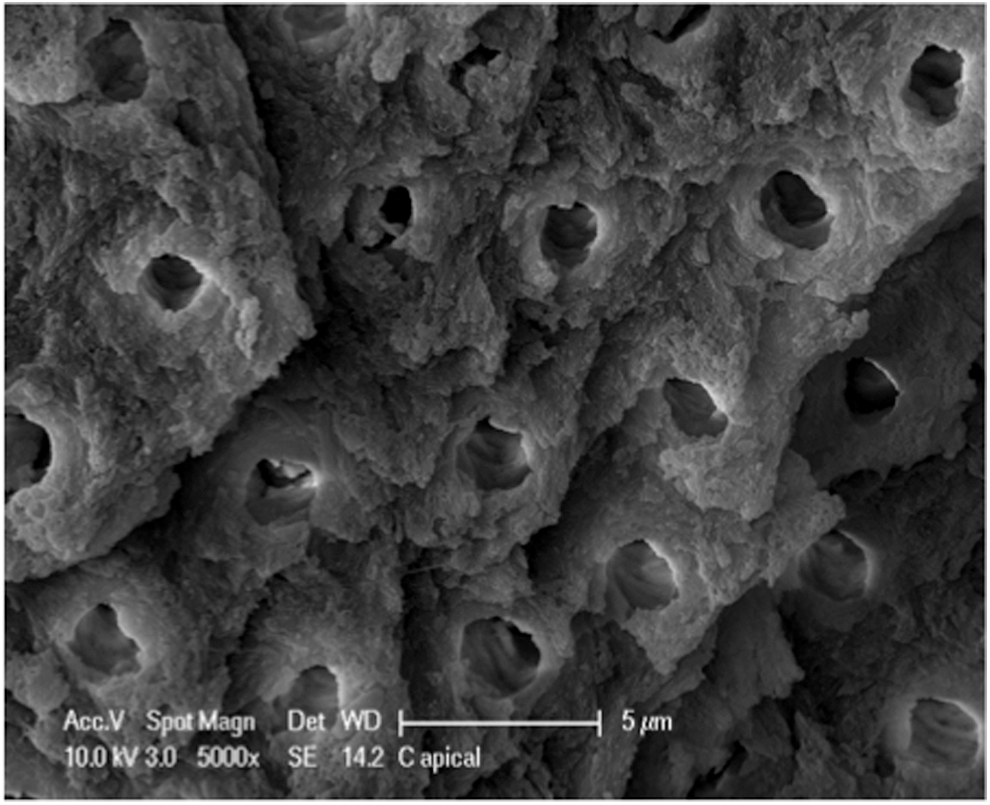
Scanning electron microscopy of Group C apical third (5000×).
Discussion
In our study, a dual wavelength protocol was used to fulfill the goal of removing the smear layer along with bacterial eradication within the root canal system. 30–31 The Er,Cr:YSGG laser, at a wavelength of 2780 nm, has been shown to be able to remove the smear layer because of the high absorption coefficients in hydroxyapatite and water molecules. 32 –34 The 940 nm diode wavelength is transmitted through the dentin and is able to penetrate deeper into the dentinal tubules, improving the disinfection properties. 35,36
We aimed to compare the temperature rise in human teeth, induced by the alternating use of the Er,Cr:YSGG laser and the 940 nm diode laser. The pattern of temperature changes is shown in Fig. 4. Each peak value corresponded to the rapid temperature rise and the passage of the optical fiber near the thermocouples. Then temperature dropped firmly as the fiber was moved away. The negative ΔT values are attributed to the water spray effect, as well as the use of irrigants, which were at room temperature of 21°C.
Although most of the temperature changes between the three groups and between different areas within the same group were significantly different (p < 0.001), the highest increase in temperature was 8.36°C for 10 sec, which is lower than the physiological limit of 10°C. 21 Therefore, these statistical significant differences may be considered clinically irrelevant.
Our results are in accordance with a recent study that evaluated the temperature elevation on the external root surface and subsurfaces during root canal treatment using a dual wavelength laser Er,Cr:YSGG (1.25 W, 50 Hz, 50 μs, 60% water, and 30% air) and a 940 nm diode laser (2 W, pulsed mode). It was concluded that within the limits of an in vitro study, the alternative use of a dual wavelength laser can be considered safe for endodontic purposes. 37
With regard to the differences in temperature elevation between the different areas within the same group, the highest temperature rises were consistently measured at the apical thirds. This can be attributed to the fact that the dentin thickness in this area is thinner, which makes it the most susceptible region to display thermal damages. 38 In fact, previous studies reported that temperature elevation in both external root surfaces and their surrounding tissues is highly influenced by the anatomy of teeth (i.e., shape and size), 39 and the heat flux on the root surface is not only related to the laser power but also to the canal surface area. 40 Our results may confirm such findings.
Unlike bare fibers, which deliver the laser beam in a forward direction, the RFT fibers such as those used in this experiment have the advantage of delivering the laser beam in a radial pattern, decreasing the possibility of any thermal damage to the surrounding tissues. 24,41 The tip of the laser fiber might also lead to a higher temperature rise in the apical area, since it comes closer to the canal walls because of the tapered shape of the root canal; this supports why the fiber should be constantly moved in a helicoidal motion. 33,42
Blood circulation in an in vivo situation must be taken into consideration as it will enhance thermal conductivity of the periodontal tissues. Saunder 43 demonstrated that in an in vivo situation, the body's recovery from temperature elevation is faster than in an in vitro situation. Most in vitro studies measured the root surface temperature from a baseline temperature of room temperature or human body temperature. 44,45 In this study, the samples were immersed in a water bath stabilized at 37°C to simulate the in vivo situation. In fact, a drop in temperature was observed during temperature measurement between the laser radiation rounds; this observation is similar to those from previous studies. 46
In addition, the water spray during laser irradiation is an important factor in the cavitation effects promoted by the Er,Cr:YSGG laser and its effects on smear layer removal. 34,47 This was confirmed by the morphological evaluation in our study. In Group A (Er,Cr:YSGG, 1.25 W) and Group B (Er,Cr:YSGG, 1.25 W and 940 nm diode, 2 W, 20% duty cycle), the smear layer was removed. However, some areas showed inefficient cleanliness, specifically in the apical third, where the smear layer occluded the dentinal tubules. This can be explained by the fact that the root canal is constricted in the apical third, where most of the debris is produced during conventional root canal instrumentation. 5
In Group C (Er,Cr:YSGG, 1.25 W and diode 940 nm, 2 W, 50% duty cycle), the SEM images presented a different pattern, showing uniform smear layer removal along the entire root canal wall and open dentinal tubules. The increased irradiation time (nine laser cycles) may have influenced the superior results of this group, as an effective removal of the smear layer could be noticed even at the apical third (Fig. 8).
Based on the results of this preliminary study, it can be expected that this dual wavelength laser (2780 and 940 nm) protocol can be safely tested in clinical studies, possibly offering a new contribution to endodontic treatment.
Conclusions
Based on the conditions of this study, it can be concluded that the alternate use of the Er,Cr:YSGG (1.25 W, 25 mJ, 50 Hz, W/A: 50/30) and the 940 nm diode (peak power 2 W, duty cycle 50%) lasers is safe regarding its thermal assurance. Further studies with regard to smear layer removal, root canal surface morphology, and microbiological tests are recommended.
Footnotes
Author Disclosure Statement
No competing financial interest exits.