
Abstract
Introduction
D
One of the most important steps in endodontic treatment is preparation of the root canal system, and root canal instrumentation techniques have undergone major changes in recent years. Rotary and reciprocating instrumentation systems have been developed in an attempt to simplify these techniques and facilitate endodontic treatment. These systems reduce the rate of accidents and complications 4 –7 and provide centered root canal preparation, 4 less apical extrusion of debris, and substantial bacterial reduction in the root canal. 4 Reciprocating systems use a single file and reciprocating motion to accomplish endodontic treatment while reducing cross-contamination. 6,8 The alternating motion of this technique also reduces the incidence of instrument fatigue. 7
Photodynamic therapy is used both as an alternative and as an adjunct to endodontic instrumentation to reduce the residual microbial load in root canals after chemical and mechanical debridement. 9 –11 Photodynamic therapy is a low-toxicity method that consists of application of visible light combined with administration of a photosensitizing agent. This photosensitizing agent, or photosensitizer, is a compound capable of absorbing light in a specific wavelength and can produce lethal cytotoxic agents able to selectively destroy cells. 12
Application of photodynamic therapy before instrumentation can reduce contamination of the root canal system, facilitating cleansing and reducing postoperative sensitivity. During biomechanical preparation, scraps of dentin, pulp fragments, necrotic tissue, and microorganisms mix with the irrigant solution and may remain attached to the root canal wall, thus obstructing the dentin tubules, or may be extruded through the apical foramen and cause flare-ups. 13 When bacteria and their by-products are extruded into the periapical tissues, this triggers an inflammatory response, the intensity of which depends on the number and virulence of the microorganisms involved, as well as on the host defenses. 14
Several techniques can help reduce the microbial load present in root canal systems before and after instrumentation and thus minimize the risk of reinfection and the degree of postoperative discomfort. 5 Within this context, the present study sought to evaluate the antimicrobial activity against E. faecalis of photodynamic therapy when applied before and after reciprocating instrumentation of permanent molars. Our null hypothesis was that no significant differences in reduction of E. faecalis would be observed before and after photodynamic therapy and after instrumentation.
Materials and Methods
The present study was approved by the local research ethics committee (Protocol No. CE/UCS-218/2013).
Sample selection
Eighteen mesial roots were selected for the study, taking into account predefined inclusion and exclusion criteria (Fig. 1).
Sampling flow chart.
The inclusion criteria were 15 as follows: complete root formation; no history of endodontic treatment, obstructions/calcifications, pathological external and/or internal root resorption, root cracks, or fractures; root length equal to or greater than 15 mm; canal diameter smaller than a No. 15 K-file; distinct foramina for the mesiobuccal and mesiolingual canals; and root angulation 10°–40° as determined by Schneider's method (moderate and severe). 16
Sample size was calculated by means of analysis of variance (ANOVA) for α = 0.05 and β = 0.80, which revealed a need for six repetitions per treatment.
Procedures
Radiographs of all teeth were obtained in the buccolingual direction, and the degree of mesiobuccal root curvature was established. 16 Using a silicon carbide disc (Carbodent; Gysi SA, Buenos Aires, Argentina), the teeth were decoronated near the cementoenamel junction to obtain a standard root length of 15 mm. The distal root was sectioned with a silicon carbide disc (Carbodent; Gysi SA) and discarded. The cervicoapical dimension of the mesial root was measured with calipers and the measurement transferred to a millimeter ruler. The orifice of the mesiolingual canal was sealed with light-curing resin (Z250 XT; 3M, Deutschland, Germany) in accordance with the standard dental restorative technique.
The apical foramen was sealed with epoxy resin (Araldite, São Paulo, Brazil) and the outer surface of the roots, except for the root canal orifice, rendered impermeable with two coats of nail polish. The actual working length was established through the visual method by inserting a No. 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) into the root canal and advancing it until the file was visible at the apical foramen under the operating microscope. The instrument was withdrawn and 1 mm subtracted from the measurement thus obtained. 17 To facilitate contamination of the root canal system with E. faecalis, all canals were initially instrumented with a manual No. 15 K-file (Dentsply Maillefer) down to working length and irrigated with 1 mL sterile distilled water. 18,19 Teeth were then sterilized by the moist heat method in an autoclave at 121°C for 15 min.
Root canals were contaminated with the E. faecalis ATCC 19433 standard strain, reactivated in sterile Brain Heart Infusion (BHI) broth (Acumedia Manufacturers, Lansing, MI), and incubated for 24 h at 37°C in a 5% CO2 atmosphere. The 24-h culture was seeded onto a Petri dish containing BHI agar and incubated for 24 h at 37°C in a 5% CO2 atmosphere. After microbial growth was observed, a suspension was prepared in a tube containing 10 mL sterilized normal saline solution and adjusted to match a McFarland turbidity standard of 2. In a sterile test tube, 5 mL of the prepared solution was added to 5 mL sterile BHI broth (Acumedia Manufacturers) to obtain the final suspension. 4,11,15
A 20 μL aliquot of the final suspension was injected into each root canal using a 0.3-cc insulin syringe. Specimens were stored in 24-well cell culture plates (Costar, New York, NY). Sterile cotton pellets moistened in sterile distilled water were added to four wells in each plate to ensure a moist environment. The plate lid was closed and sealed with adhesive tape, and the preparation incubated for 21 days at 37°C in a 5% CO2 atmosphere. Every 2 days, 20 μL sterile BHI broth (Acumedia Manufacturers) was added to the root canals with a 0.3-cc insulin syringe and the cotton pellets were replaced with freshly moistened ones. 4,15,20
The viability and purity of the microorganisms within the canals were checked weekly by random sampling of two teeth using sterile paper points (Dentsply Maillefer), which were placed and kept inside the canals for 1 min, seeded onto sterile BHI broth (Acumedia Manufacturers), and incubated for 24 h at 37°C in a 5% CO2 atmosphere. After microbial growth, smears and Gram stains were prepared for morphological and stain-based confirmation of bacterial identification. 11,15
After 21 days of contamination, the teeth were randomly divided into three groups (n = 6) (Fig. 2):
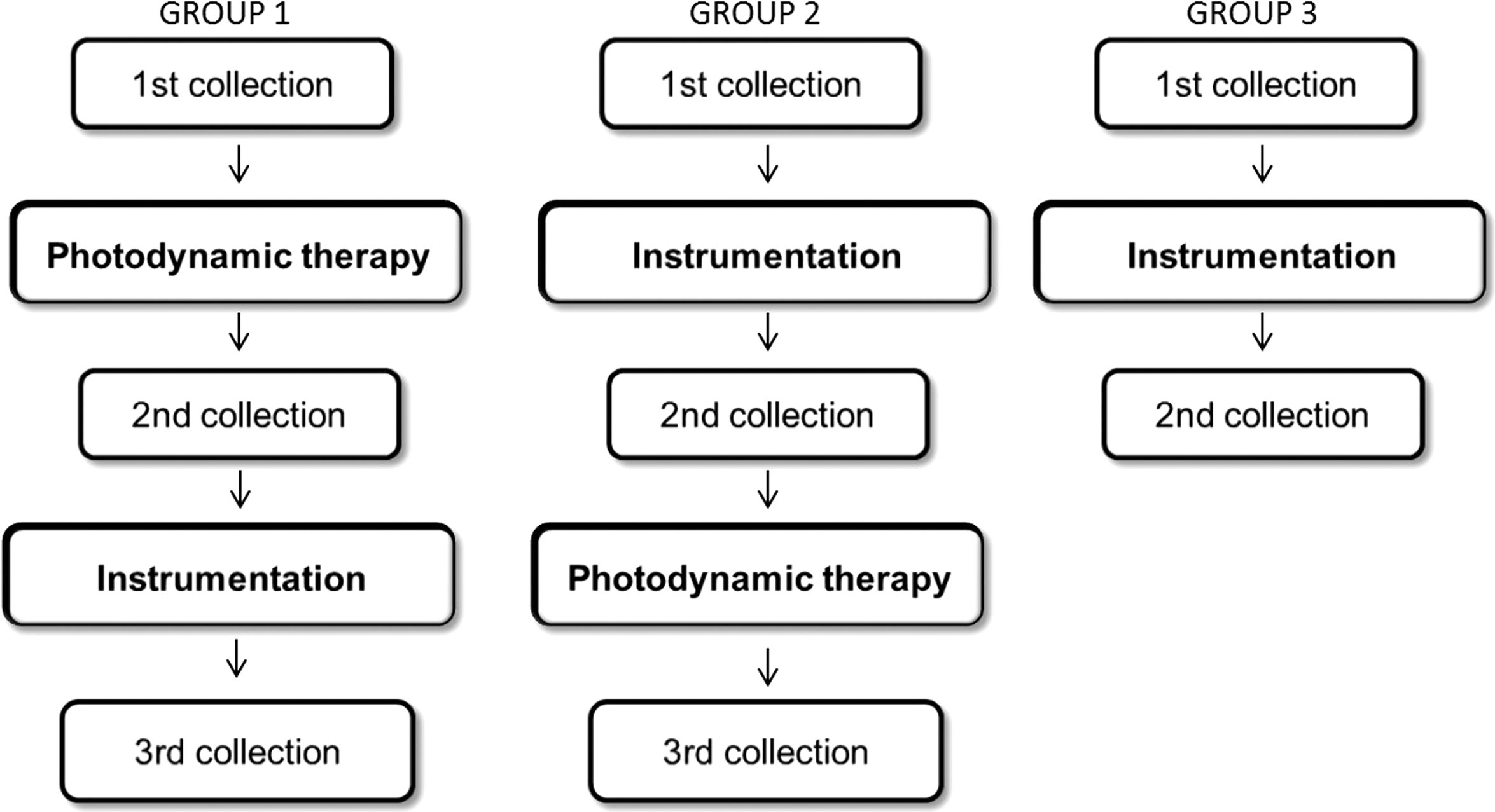
Group allocation flow chart.
Group 1: initial sampling was performed for enumeration of viable bacteria, and photodynamic therapy was performed using a low-level laser system (Flash Lase III; DMC, São Carlos, Brazil; energy density 4 J/cm2, wavelength 660 nm, power 100 mW) and 0.01% methylene blue as the photosensitizing agent (DMC). 9 The photosensitizer was administered along the working length of the canal by inserting a sterile paper point (Dentsply Maillefer) with a diameter consistent with the anatomy of the canal and leaving it in place for 3 min. 9 Diode laser was applied to the root canal orifice with a 600 μm diameter fiber optic probe (DMC) for 40 sec. Before instrumentation, the fiber optic probe was introduced into the canal and advanced until resistance was felt. Throughout the application, the active tip of the laser device remained in contact with the canal. After this therapy protocol, the viable bacterial count was determined. Subsequently, the canals were instrumented with the WaveOne system (Dentsply Maillefer) and a new viable bacterial count was obtained.
Group 2: canals were swabbed for enumeration of viable bacteria and instrumented with the WaveOne system (Dentsply Maillefer). After instrumentation, the viable bacterial count was determined. Photodynamic therapy was performed using the same protocol as in Group 1, except for the fiber optic probe, which was advanced to the full working length. After completion of photodynamic therapy, a new viable bacterial count was performed.
Group 3: canals were swabbed for enumeration of viable bacteria and instrumented with the WaveOne system (Dentsply Maillefer). After instrumentation, the viable bacterial count was determined. The canals were instrumented with a WaveOne reciprocating system (Dentsply Maillefer) using a single 25.08 file (Primary) 21 powered by an X-Smart Plus electric motor (Dentsply Maillefer) in the WaveOne mode. Three cycles of instrumentation were performed. Each cycle consisted of three in-and-out motions. During the first cycle, the file was advanced solely into the coronal third of the canal, past the orifice. During the second cycle, the file was advanced to the canal curvature, or 5 mm short of the working length, which corresponds to the middle third of the root. Finally, during the third cycle, the file was advanced to the full working length, completing instrumentation of the apical third. 4 Between cycles, the tooth was instrumented to its actual length with a No. 10 K-file (Dentsply Maillefer). At each cycle, the canals were irrigated with 1 mL of saline solution (total volume 3 mL) in Groups 1 and 2 and with 1 mL of 2.5% sodium hypochlorite (total volume 3 mL) in Group 3, using a plastic syringe and NaviTip needle (Ultradent Products, Inc., South Jordan, UT) with an external length of 0.3 mm applied within 1 mm of the working length. 22 All teeth were instrumented by the same investigator.
Bacterial sampling was performed using sterile paper points (Dentsply Maillefer) of a size compatible with the anatomic diameter of each canal. The gauge of the paper points used for bacterial sampling and photosensitizer delivery was consistent with the diameter of the file. As canals were initially instrumented with a No. 15 file, No. 15 paper points were used for initial sampling and delivery of the photodynamic therapy (PDT) agent before instrumentation. Bacterial sampling after instrumentation and after PDT was performed with No. 25 paper points, a size consistent with the diameter of the primary file (25.08). The paper points were introduced and kept within the canal for 60 sec and immediately placed into a test tube containing 5 mL of sterile BHI broth (Acumedia Manufacturers). Before each sampling collection, the canal was irrigated with 0.1 mL sterile BHI (Acumedia Manufacturers).
The samples were diluted, seeded, and cultured. Homogenization was performed for 3 min using a shaker. Five 1:10 dilutions were prepared in sterile peptone water (Acumedia Manufacturers), and three 25-μL aliquots were seeded with a micropipette onto BHI agar plates. 23 Between each dilution, the preparation was homogenized for 30 sec. All plates were incubated in anaerobic jars (Oxoid Ltd., Basingstoke, Hampshire, England) for 24 h at 37°C in an 85% N2, 10% CO2, and 5% H2 atmosphere, obtained using gas-generating envelopes (Anaerogen™; Oxoid Ltd.), and stored in a microbiological incubator. The total viable bacterial count was established using a colony counter.
D'Agostino's test for normality revealed non-normal distribution of sample data. Therefore, the results were log10 transformed and descriptive analyses were performed. Results were then analyzed by the nonparametric Wilcoxon and Kruskal–Wallis tests.
Results
Significant reductions in E. faecalis were observed when photodynamic therapy was performed before and after instrumentation of the root canal system (p < 0.05) (Tables 1 and 2). Reciprocating instrumentation significantly reduced E. faecalis contamination (p < 0.05) when saline solution and 2.5% sodium hypochlorite were used as irrigants (45.11% and 52.34% reduction, respectively) (Tables 2 –4). There were no significant differences in baseline E. faecalis counts among the three groups, which demonstrates the efficacy of specimen standardization (Table 4). Comparison of baseline E. faecalis counts to those obtained after PDT and after instrumentation revealed greater reductions after instrumentation, regardless of the irrigant used (Tables 4 and 5).
Different superscript letters along the same column denote p < 0.05.
INST, instrumentation; IQR, interquartile range; PDT, photodynamic therapy; SD, standard deviation.
Different superscript letters along the same column denote p < 0.05.
Different superscript letters along the same column denote p < 0.05.
Different superscript letters along the same line denote p < 0.05.
p < 0.05.
Discussion
The objective of this study was to evaluate the efficacy of reciprocating instrumentation and photodynamic therapy for disinfection of root canals contaminated with E. faecalis. This species of bacteria invades the dentinal tubules, which protects it from conventional chemical agents. 24 To the best of our knowledge, there are no published studies involving concomitant use of reciprocating instrumentation and photodynamic therapy as adjuncts to the root canal decontamination process.
During specimen preparation for the present study, root canals were preshaped with a No. 15 K-file 18,19 to facilitate contamination, as reported by Zand in 2014 and Nunes in 2011. 3,18 During instrumentation, in Groups 1 and 2, root canals were irrigated with saline alone, 18 as the chemical irrigants commonly used during endodontic treatment have antimicrobial effects and could interfere with the results of the experiment. A control group was established using 2.5% sodium hypochlorite as the irrigant solution.
The method of canal contamination used in the present study was based on several previous reports, 4,11,15 while the choice of the culture method to assess antibacterial activity was based on the work of Alves in 2012, 25 who found no differences between PCR and the culture method for assessment of the antimicrobial activity of reciprocating versus rotary NiTi instrumentation and concluded that the culture method can be used effectively to test the antibacterial efficacy of treatment protocols in the ex vivo setting.
Several photodynamic therapy protocols are available, with differences in choice of light, photosensitizer, and fiber optic, among other parameters. For this study, we chose to use fiber optics, and all laser parameters were based on prior research. 3,18 The use of fiber optics directs radiation within the root canals, distributing light homogeneously, when inserted to the entire length of the root canal, as in Group 2. However, when PDT was performed before instrumentation (Group 1), the fiber optic was advanced into the canal only until resistance was met. Therefore, the fiber optic did not penetrate the entire length of the canal, preventing homogeneous distribution of light throughout the canal system. Nevertheless, significant reductions in bacterial burden were achieved, as demonstrated on comparison of E. faecalis counts before and after PDT. It also bears stress that failure to advance the fiber optic the entire length of the canal when PDT is performed before instrumentation actually prevents apical extrusion of microbial pathogens.
The choice of methylene blue as photosensitizer was based on its ability to absorb light at the 620–660 nm wavelength, 26 which is consistent with the red light emitted by the laser diode used in this study. Methylene blue was delivered into the root canal system not by irrigation but by using paper points. 9 In this technique, paper points are soaked in the photosensitizer agent and pressed into the root canal, thus releasing the agent.
Low-level laser activates the photosensitizing agent, emits radiation at the appropriate wavelength, and features low power consumption. The wavelength determines the depth of light penetration into the target tissue. A wavelength in the 630–700 nm range corresponds to a light penetration depth of 0.5–1.5 cm, 27 which has therapeutic effect. Interaction between the photosensitizer and the light produces reactive oxygen species (singlet oxygen, free radicals, and superoxide anions). These substances produce bacterial lysis by damaging the bacterial cell wall, nucleic acids, and protein membrane. 28
The results obtained in the present study demonstrated a significant reduction in E. faecalis after application of photodynamic therapy to the root canal system, which is in agreement with prior investigations, 3,9,22 thus refuting the null hypothesis. Postinstrumentation photodynamic therapy enabled reduction of E. faecalis resistant to instrumentation, as demonstrated in several previous studies. 2,9,29 Residual microorganisms can remain in the root canal system even after chemical and mechanical preparation, creating an environment conducive to reinfection and failure of endodontic treatment. 30,31 According to Siqueira Júnior and Rôças 2008, 31 the presence of bacteria within the canal after instrumentation is a risk factor for development of posttreatment apical periodontitis. The complex anatomy of the root canal system, which consists of the lumen of the main canal, the accessory canals, ramifications, apical deltas, and recesses, means that instrumentation alone can be insufficient to ensure complete disinfection. 32 The bacteria detected in posttreatment samples are either remainders of the initial infection that survived the disinfection process or were introduced into the canal through a breach in aseptic technique. 31 Reciprocating instrumentation cleanses the root canal system by removing significant amounts of smear layer and debris 7 and consequently exposing the dentin tubules, facilitating dye penetration and achievement of the photodynamic effect.
In the present study, the reduction in E. faecalis achieved when photodynamic therapy preceded root canal instrumentation led to a significant decrease in the burden of E. faecalis present in the root canal system. This decrease in bacterial burden can help reduce apical extrusion of microorganisms during the instrumentation process. Apical extrusion of debris can cause flare-ups due to introduction of bacteria, pulp tissue, and irrigating solution into the periapical tissues. 5 Even a small amount of infected debris, when extruded apically, has the potential to cause or exacerbate periapical inflammation. 33 One may presume that, by minimizing the amount of apically extruded debris, the dental practitioner can also minimize postoperative reactions. The literature has shown that extrusion of material beyond the apical foramen occurs with essentially all instrumentation techniques to a greater or lesser extent, 34,35 even when instrumentation of the root canal is kept short of the apical foramen. 36 There is little published research on the use of photodynamic therapy before root canal instrumentation. The present study sought to bridge this research gap. Photodynamic therapy can be used as an adjunct to endodontic instrumentation before or after decontamination protocols, as the results of this study demonstrated efficacy in both groups.
Conclusions
The present study demonstrated that instrumentation with a reciprocating system significantly reduced E. faecalis colonization in experimentally contaminated root canal systems. Photodynamic therapy effectively reduced E. faecalis in the root canal system, whether performed before or after reciprocating instrumentation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.