
Abstract
Introduction
C
The adult forms are exceptional. 4 –6 Redenbacher described lymphangiomas for the first time in 1828, but their relationship with the lymphatic system was reported half a century later by Koester. 7 The frequency of occurrence of lymphangiomas is 42% in the cervicofacial area; 23% in the cervicothoracic zone; and 35% in the limbs, intraperitoneal, and retroperitoneal parts.
Several clinical forms of lymphangiomas are described in the literature, starting with the microcystic lymphatic malformations (lymphangioma circumscriptum). 8,9 These are superficial to the skin and manifest as small papules or translucent pink plaque-like infiltrated lesions. They are, in most cases, on the limbs, the genital area, and the dorsal surface of the tongue. Presentation varies from asymptomatic, inflammatory with infectious episodes, to bleeding in lymphatic cavities. Another form are the macrocystic lymphatic malformations (cystic hygroma), 9 corresponding to large unilocular or multilocular cysts lined by a layer of endothelium and surrounded by fibroblasts and numerous smooth muscle fibers. Thirty to fifty percent of these macrocystic malformations are present at birth, and in rare cases occur in adulthood. They affect the neck in 75–85% of the cases, and ∼20% are localized in the maxillae. Their clinical expression depends upon their location. The third form are the mixed lymphatic malformations (cavernous lymphangiomas). 9 These are combinations of the two previous forms, and present as painless masses on the surface of microcystic elements. They are most often located in the face and neck areas, but they can also affect other parts of the body. Frequency of occurrence is the same in both sexes.
The literature is rich in treatment modalities of lymphangiomas. Several treatments were proposed with variable rates of success. 3,4,8,9 Some authors believe that the spontaneous regression of lymphangiomas is common and could possibly happen in 15% of the cases. Accordingly, they suggest delaying the interventional treatment until the age of 3–5 years. 3 Sclerotherapy involves injecting an irritant solution directly into the vein, causing inflammation, which induces the contraction of the blood vessel wall. 10 –13 Surgical excision is the conventional approach to avoiding the risk of hemorrhagic or infectious complications or unpredictable growth of the cystic volume with the possibility of mechanical consequences. 10 –14 Complete excision of lymphangiomas sometimes requires multiple interventions with risk. The frequency of complications varies between 10 and 33%, and the intraoperative blood loss can be significant. Nerve damage was observed in 30% of surgically treated head and neck lymphangiomas. The most frequently injured nerve is the mandibular marginal branch of the facial nerve. Nerve damage is generally a function of the size and location of the lymphangioma. 9 –11,14 Radiotherapy has been described for nonsurgical treatment of lymphangiomas. 15
Several types of lasers were used in the treatment of lymphangiomas. 16 –18 Argon, CO2 and Nd:YAG lasers were suggested for the treatment of lymphangiomas and hemangiomas. 16,18 –24 The CO2 laser has been used for the resection and removal of superficial lymphangiomas by photocoagulation. 25 There were no studies that reported long-term results for laser treatment of large, unexcisable oral lymphangiomas
The aim of our study is to evaluate the efficiency of a new therapeutic method using CO2 laser to avoid mutilation or total excision for the treatment of invasive, large. and unexcisable oral lymphangiomas.
Patients and Methods
Seventeen patients were included in this study. The age range of patients was 9–38 years, with an average age of 23 years.
Exclusion and inclusion criteria
Only invasive and extensive lymphangiomas in oral cavities were reported in this study. Cases with the possibility of being treated simply by excision or other therapies were not considered, and only lymphangiomas involving exclusively oral soft tissues were selected. Patients with lymphangiomas invading the face skin were excluded.
We included in our study patients who had received previous treatments (surgeries, cryosurgeries) without success, and for whom the decision to use mutilating therapies was considered.
Patients with lymphangiomas that could be treated simply by excision or other therapies and localized outside of the oral cavities were excluded.
This new therapeutic method was proposed as a last choice of therapy before any mutilating techniques. All selected patients were healthy. We excluded risky patients (immunosuppression, organ transplant, heart diseases, under chemo or radiotherapy, coagulation disorder, diabetic, tissue healing disorder, etc.) from our study. No medications were prescribed before surgeries.
In order to confirm our clinical diagnosis, ultrasound and/or magnetic resonance imaging (MRI) examinations were usually performed.
According to the recommendations of the ethics committee of our university hospital, the decision to perform surgery was made after informing patients about the different steps in each surgery, the risks, and the expected postoperative discomfort, and surgery was performed only after receiving the consent of the patient.
Surgical protocol
A CO2 laser machine (10.6 μm: Smart US20 D Laser 10 600 nm, High Tech Laser, Herzele, Belgium) was used in this protocol. The parameters of irradiation were output power of 2 W in defocus and in noncontact mode for 3 min minimum. The distance between the laser handpiece and the tissular impact point was ∼6 cm, the delivered focal point was 0.3 mm, the effective spot diameter range at tissue was ∼2 cm (power density = 0.63 W/cm2), and the estimated energy density range was 114.65–191 J/cm2. The treatment was almost the same for all patients.
Most surgeries were performed with the patient under local anesthesia (articaine with vasoconstrictors). All medical staff and patients wore specified glasses to protect their eyes against CO2 laser beam. The surgical procedures were performed as follows. The treatment was performed in one or multiple sessions depending upon the extent of the lesion, to allow patients to continue their normal lives. We always started by using a defocus beam maintained perpendicularly on each treated area of 2 cm in diameter for 3–5 min, in order to generate a deep penetration of heat in lased tissue (tissue overheating). Under those conditions, the laser beam was not able to disintegrate tissues, but was only able to generate heat. The deep tissular overheating was induced by a cumulated effect. After 3–5 min of irradiation, the aspect of the surface of the operated area became totally carbonized. An overlapping was done for adjacent treated areas. To avoid tissue vaporization, the laser beam was never used in focus mode. We did not make any incision or excision of the lymphangioma. The aim of the surgery was to provoke an extreme tissue overheating and to induce a fibrous healing process in order to change the nature of the tissue from lymphatic to fibrous. The carbonization was kept on the tissue surfaces and the wound was left without any makeup and without wound dressing in order to avoid postoperative bleeding. No sutures were used; the wound healed by second intention.
An adapted antibiotic, nonsteroidal anti-inflammatory, analgesic, and oral disinfecting solution (chlorhexidine 0.2%) were prescribed for 10–14 days during the postoperative period. In some cases, patients took nonsteroidal anti-inflammatories and painkillers for 20 and 25 days, respectively.
The patient's postoperative oral hygiene instructions were always complied with. Patients were prohibited from rubbing their wounds for any reason. A liquid or semiliquid cold food diet was recommended for 4 weeks postoperatively.
For more extended or spread lesions, the procedure was performed over several sessions (treated area was 3 × 3 cm or 4 × 4 cm per session) to reduce postoperative discomfort, and allow patients to continue their normal lives without major difficulties.
Follow-up
Patients were recalled after 10 days, 4 weeks, 8 weeks, 6 months, 12 months, and once per year over 20 years from 1994 to 2014. The purpose of this was to determine the aspect of the healed mucosa in order to exclude an eventual recurrence.
Case report of a patient treated with the new technique
A 38-year-old Caucasian female had a deep diffuse lymphangioma on the tongue (Fig. 1). The lesion affected the whole tongue, with the following complaints: macroglossia causing serious difficulty in chewing, swallowing, and speaking (because of the abnormally large tongue); and patient always had a bloody taste because of the opening and bleeding of superficial vesicles filled by blood (Fig. 1).
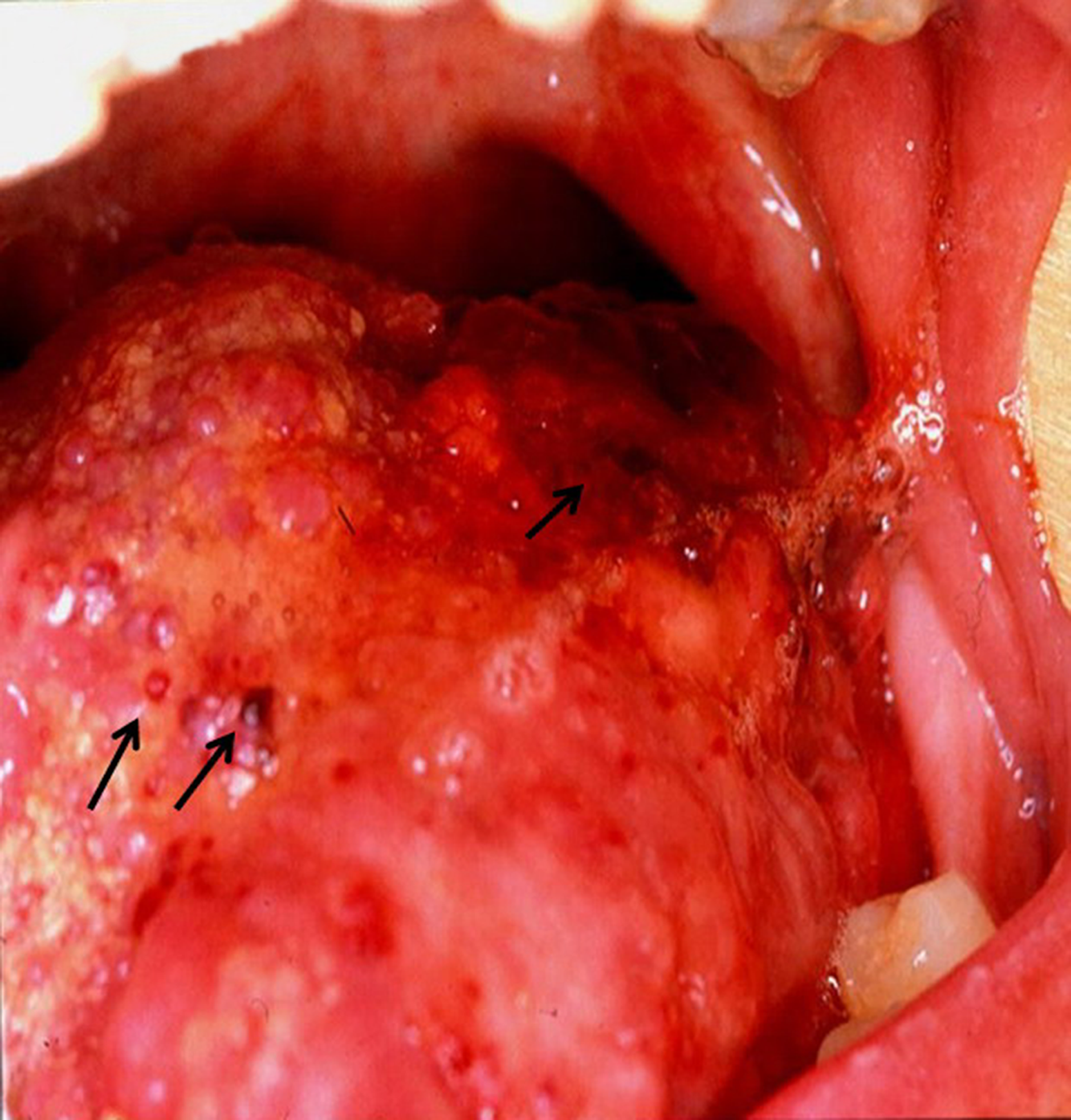
View of the invasive and diffuse lymphangioma. It involved all the tongue volume, causing a macroglossia. Arrows show some blood vesicles of different sizes.
The patient reported that she had received many treatments since she was 2 years old (surgeries, electrocoagulation, excisions, radiotherapy, cryotherapy, injection of sclerosing agents, drainages) without any success. The patient was treated in five sessions to reduce severe postoperative discomfort, allowing her to continue a normal life. Each session concerned the treatment of one fifth of the total volume of the tongue.
Before starting any surgical procedures, the operator, assistants, and patient put on specific protective eyeglasses and local anesthesia (articaine with vasoconstrictor) was administered. The surgical procedure was similar to that described in the our surgical protocol (described previously). No sutures were applied at the end of the surgery. The wounded area was left to heal through secondary intention, without any specific treatment. As postoperative treatment, an antibiotic, anti-inflammatory, analgesic, and mouthwash solution (chlorhexidine 0.2%) were prescribed.
Results
Pain, postoperative edema, and swelling were always reported during the postoperative period. In some cases, the complete healing of wounds with a normal tissular aspect was reached 6–8 weeks postoperatively (Fig. 2). During the healing period, the wounds appeared to have recovered, having a layer of fibrins with a white or gray aspect.
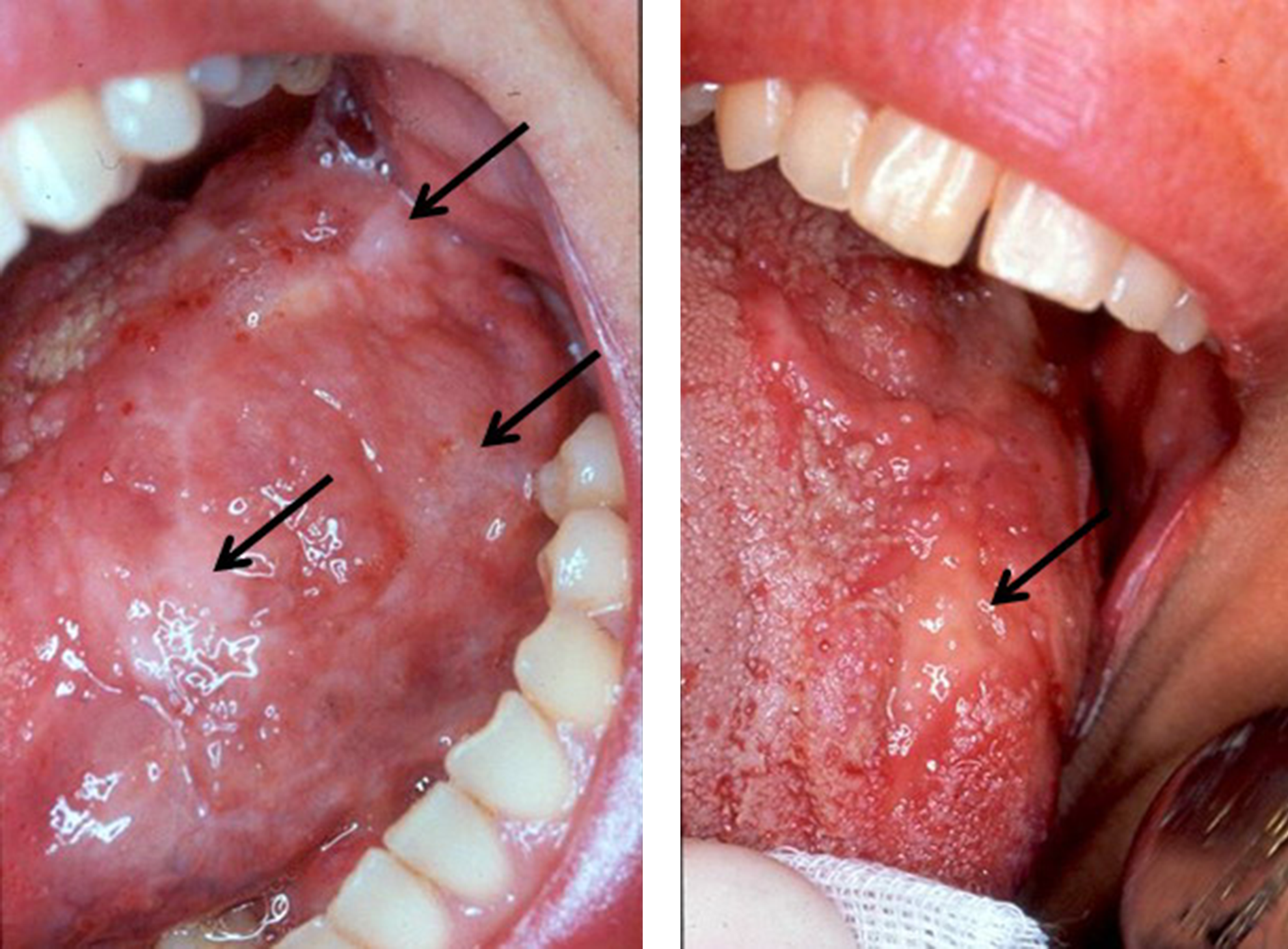
Postoperative view of the last operated part of the tongue. The fibrin is still covering the wound 6 weeks postoperatively (see arrows).
No serious side effect (embolism, secondary infection of operated site, nerve damages, mutilation) was reported during the postoperative period.
A permanent residual aspect of scar healing continued to be noticed after many years. No recurrence was monitored after long-term follow-up (10–20 years) (Fig. 3). The volume of operated tissue was reduced to normal (Fig. 3). Patients resumed a normal lifestyle with improved functionality, and enjoyed the new functionalities (eating, swallowing, and speaking, and, therefore, participating in more social activities). The results of biopsies performed 5 years postoperatively confirmed that fibrous tissue replaced the lymphatic tissue.
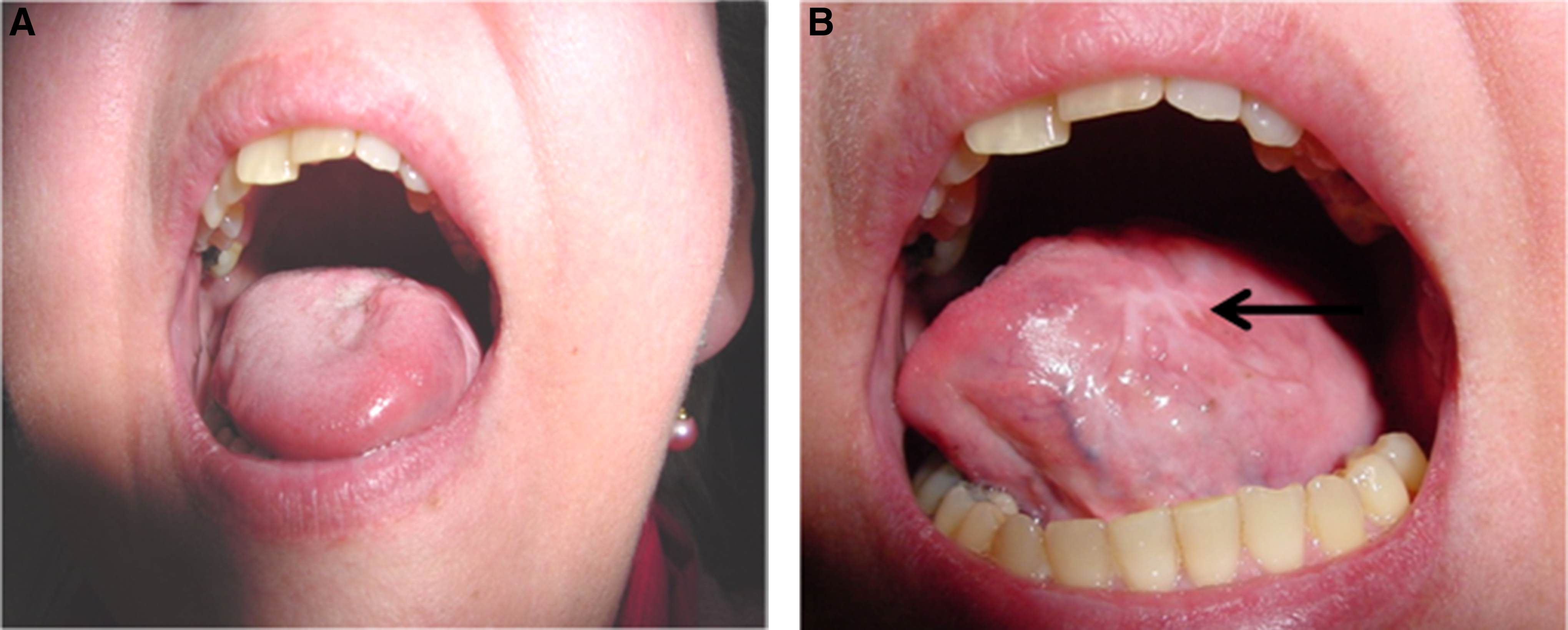
At 20 years follow-up, the normal volume of the tongue is stable. The aspect of tongue surface is satisfactory
The results of the proposed treatment on 17 patients had an 82% total success rate (14 patients), without any recurrence after 10 years' follow-up. Approximately 18% (three patients) had a localized and limited recurrence of the lymphangioma at the surgical sites (Table 1). The localized recurrences were re-treated, with complete healing.
Discussion
The pathogenesis of lymphangiomas is not yet fully understood. Various theories have been proposed to understand and manage this pathogenesis. The first is that it is congenital. This is the most widely advocated among the pathogenic assumptions because of the discovery of lymphangiomas in the first decade of life, with a high frequency in infants. 3,26 The second possibility suggested is that it is an acquired affection. According to this theory, which is now discredited, the lymphatic circulation would be interrupted, causing ectasia of the vessels. But the abundant anastomoses that exist in the lymphatic system, which are easy to highlight, oppose the theory of obstruction of all lymphatic channels. 3 The third pathogenesis is the relationship between the presence of lymphangiomas and antenatal exposure to alcohol, which has been reported by Edwards and Graham. 3 Lymphangiomas are most often isolated, but they can also be part of genetic abnormalities such as Noonan syndrome, or chromosomal abnormalities such as Turner syndrome, Klinefelter syndrome, and trisomy. 26 –28
Lymphangiomas are discovered, most of the time, in the first 2 years of life, mostly on the dorsal and lateral borders of the tongue. They rarely form on the palate, cheek, or lips. Often, their diagnosis is clinical. Conventional radiology is sometimes useful to assess the impact of lesions in the airways and on the backbone or to highlight mediastinal extension. The extension of lymphangiomas can also be detected by ultrasound, CT scans, or MRI. Ultrasounds 29 are considered to be an excellent diagnostic tool. They specify the seat and nature of the mass as well as its limits and relationships with adjacent organs, and can be used for postoperative monitoring and detection of recurrence. The CT scan is a well-respected radiological examination for tissue explorations of cystic lymphangioma. 30 MRI is the gold standard, but access is sometimes difficult and expensive. It allows a better delineation of the lesion in relation to adjacent organs and muscles. MRI remains the modality of choice for assessing the in-depth extension, which is undetectable during clinical examination. It also helps to assess the infiltration into underlying tissues 31,32
The histology of lymphangiomas is multiple, and with wide expansion nodes, dermal or epidermal, with regular endothelial cells without atypia. These structures differ histologically by venous malformations, greater muscular component (media), the shape of the vessels, which is more rounded, and, especially, the absence of erythrocytes. There are also macrophages, neutrophils, eosinophils, and a few red blood cells, but not tumoral cells. The liquid may be acellular. 33
A significant advance in the understanding of the pathogenesis of lymphangioma was made as a result of the discovery of a growth factor receptor lymphatic tissue. Vascular endothelial growth factor-C is the ligand for VEGFR-3 and VEGFR-2 in transgenic mice that induces the growth of lymphatic vessels in the skin, without influencing the development of blood vessels. 34
Surgical excision is considered by most surgeons to be the treatment of choice for lymphangioma, 35,36 with the approach being different according to each clinical type. Small lymphangiomas are treated by total excision of the lesion together with its base of normal mucosa. 37 –40 On the other hand, in cases of diffuse lesions, total excision with preservation of involved vital structures is not always possible, because the lesion extends into surrounding tissue and/or infiltrates vital structures, and radical excision may then result in serious complications. 18 From another standpoint, incomplete excision is frequently associated with recurrence. 35,37 –40
Laser use for oral surgery has become favorable because of its ability to coagulate and cut. Its main advantage is to seal blood vessels during surgery and vaporize the lymph content. In previous studies, laser is used with the aim of surgically excising or photocoagulating small lymphangiomas. Several authors have shown the possibility of successfully treating small lymphangiomas by means of different kinds of lasers (Argon, Nd:YAG, KTP, diodes, and CO2) 17,41 –47
The treatment of lymphangioma of the oral cavity by lasers is either by resection of the lesion or by photocoagulation for small localized lesions. These give good results, but it is difficult, if not impossible, to treat large and diffuse lesions successfully because it is impossible to excise the whole lesion. In our study, we used CO2 laser in a new procedure for the treatment of invasive (large and of extensive size) and unexcisable lymphangiomas. The new protocol was elaborated to avoid undesired oral mutilation. Torezan et al. 43 successfully performed their oral surgeries by means of CO2 laser, whereas Angiero et al. 45 used a diode laser (980 nm). CO2 laser was used in this procedure, but the difference with other reported protocols is in the procedure of the treatment. The cited authors excised or photocoagulated limited-size lymphangiomas. In our study, however, it was impossible to excise lymphangiomas because it could cause severe and permanent oral mutilation. Our aim using CO2 laser beam in the defocus mode was not to excise lesions. On the contrary, it was limited to generating heat for a long time (3–5 min) and to producing severe and deep tissue necrosis that would be slowly replaced by a fibrous healing process. Used in large defocus mode, the low output power was not able to either incise or excise tissues. Under these conditions, beam absorption by the tissue (mainly by water and organic content) was only able to generated heat. We used a long irradiation time (2–3 min) in order to allow heat to build up and penetrate progressively deeper into the tissue by cumulative effect. CO2 laser beam provoked severe and deep tissue necrosis. The healing period was long (1–2 months) because of the extent of necrotic tissue. Cellular and tissular mechanisms needed a longer time to remove and evacuate necrotic tissues, which caused the extended delay in the healing process. The fibrous replacement process was unavoidable, but it was our goal. The tissue overheating generated by the beam produces a replacement of lymphatic tissue with a new and more compact fibrous formation. By using this procedure, the lymphangioma disappeared and was replaced by a new and more desirable fibrous tissue. We did not notice any side effects (embolism, secondary infection of operated site, mutilation) during the postoperative period.
Conclusions
To conclude and within the limitations of this study, the use of CO2 laser under the specific irradiation conditions used for the treatment of oral lymphangiomas can be considered a helpful procedure. This defocus technique is suitable for large lesions, to avoid oral mutilation, as well as for localized lesions.
Footnotes
Acknowledgments
We thank Hani Ounsi and Ziad Salameh for their help with the redaction of this article.
Author Disclosure Statement
No competing financial interests exist.