
Abstract
Introduction
O
Multiple randomized controlled trials have demonstrated the efficacy of low-level light therapy, or photobiomodulation therapy (PBT), for the prevention of HCT-associated OM. 4 Collectively, these studies have demonstrated reduced risk of severe OM, reduced overall grade of OM and duration of severe OM, reduced incidence of severe pain, reduced overall mean pain scores, and reduced proportion of patients requiring opioid analgesia. 4 The majority of studies have reported protocols in which the PBT is delivered intraorally as individual small “spots” via a laser probe (0.4–1.0 cm2 per spot), exposing oral mucosal sites from the lips to soft palate in a tedious and time-consuming manner that can pose logistical challenges, especially in children. 5 Furthermore, a significant proportion of OM occurs more posteriorly in the oropharynx and esophagus, sites that can greatly impact the ability to swallow and that can be primary drivers of resource utilization (e.g., need for opioid analgesics and total parenteral nutrition), but that cannot be reached by PBT intraorally, such that the overall clinical benefits of this preventive strategy are limited. A novel approach has been the use of larger light-emitting diode (LED) arrays to treat the at-risk tissues from an extraoral approach, enabling exposure of the oral, oropharyngeal, and esophageal mucosa while avoiding the need for intraoral manipulation, and requiring only minimal patient cooperation. 6,7 The objective of this study was to evaluate the feasibility of providing extraoral PBT for the prevention of OM in pediatric patients undergoing HCT.
Methods
Study design
This was a single center pilot feasibility and safety study conducted at Dana-Farber Cancer Institute/Boston Children's Hospital. The study was activated in March 2014 and closed to enrollment in October 2014. Using survey instruments and specific metrics, the study was designed to determine if it was feasible and safe for trained nurses to administer daily PBT to children undergoing myeloablative HCT, and to determine if it is feasible to collect daily OM assessment data. The PBT device was provided by THOR Photomedicine Ltd (Chesham, UK).
Patient eligibility
Patients between the ages of 4 and 21 that were scheduled to undergo myeloablative autologous or allogeneic HCT for any indication (e.g., malignant and nonmalignant conditions) were eligible for study participation. Eligible patients could not have received PBT within 4 weeks prior to enrollment, and could not receive any other agent intended for the prevention/management of mucositis (e.g., palifermin, cryotherapy). This study was approved by the Dana-Farber/Harvard Cancer Center Office for Human Research Subjects, and all patients and/or their parents provided informed consent.
PBT device
PBT treatments were delivered using a THOR Model LX2M unit (THOR Photomedicine Ltd, Chesham, UK). The THOR LX2M is a red and near infrared light emitting diode (LED) device that is United States Food and Drug Administration (FDA) approved for management of inflammation and tissue repair. The 69 Diode LED Cluster Probe is composed of 34 × 660 nm (red; 10 mW) and 35 × 850 nm (near infrared; 30 mW) LEDs for a total power output of 1390 mW, at an irradiance of 50 mW/cm2.
Study staff training
Training for the PBT device administration and OM assessments was conducted by one of the study's principal investigators (N.S.T.) directly to the primary study nurse (M.M.). The training included a detailed slide presentation outlining information about preparing the PBT device, administering the PBT device, conducting mucositis assessments, and completing case report forms. The primary study nurse subsequently trained nine nurses using the same training materials.
PBT administration
Light therapy was administered by trained nurses on an inpatient basis. Treatment began on the 1st day of conditioning and continued daily (including weekends and holidays) until day +20 or discharge, whichever came first. There were no pre- or post-treatment measures/precautions.
The control unit was plugged into the wall, the LED array was connected to the control unit, and the device settings were confirmed. The treatment probe was activated when appropriately positioned flatly against the face and neck of the patient in one of the six treatment sites (right face, midline face, left face, left neck, midline neck, and right neck; Fig. 1). The THOR 69 LED cluster was applied for 60 sec per location, for a total daily treatment time of ∼6 min (50 mW/cm2 × 60 sec = 3.0 J/cm2 per six sites). This protocol was modeled after previous published reports as well as recommended guidelines. 5,6,8,9 The unit was disinfected with antimicrobial wipes before and after each use. The PBT device was maintained in a soft case and was stored in a locked cabinet.

Administration of extraoral photobiomodulation therapy to one of the six designated anatomic sites. The subject's informed consent was obtained for use of this photograph for publication.
A daily treatment assessment was used to record each patient's tolerability and compliance with the device. This assessment included the sites where treatment was completed during daily PBT delivery, any reasons treatment at a site was not completed during daily PBT delivery, and the level of patient comfort during treatment.
OM assessments
Participants were assessed for OM at baseline (first day of conditioning), then daily beginning day −1 through day +20 (including weekends and holidays), including an assessment on the last day of therapy. Daily assessments were still performed even when PBT was not provided. In the event that oral assessments could not be performed on a given day (e.g., patient refusal), they were resumed as soon as possible. Assessments included collection of the World Health Organization (WHO) Oral Toxicity Score and the Children's International Mucositis Evaluation Scale (ChIMES). 10,11 The study nurses recorded the clinical data in case report forms that a research coordinator then entered into an electronic data capture database.
Feasibility end-points
Data for feasibility end-points to assess various aspects of the ease and tolerability of PBT were gathered from both study nurses and patients using assessment instruments. The 10 study nurses completed an end of treatment questionnaire for each case in which they conducted an OM assessment and/or delivered PBT. This assessment included the effectiveness of the protocol training, accessibility, and maneuverability of the PBT device, and administration of PBT (device settings, positioning of device, and delivery of therapy). An additional feasibility end-point was to accrue five patients within the first 3 months of study activation.
Statistical considerations
A descriptive analysis of the study end-points was performed. For each feasibility end-point involving the calculation of a proportion, a two sided 95% confidence interval (CI) was placed on the proportion. The prespecified protocol criteria defined feasibility as having the upper limit of the 95% CI exceed 75%. For each patient, the maximum ChIMES and WHO scores were determined, and then the median and range were calculated for the overall patient cohort. The incidence of OM was calculated as the number of patients with at least one occurrence of OM at or above a given grade, divided by the total of 13 patients. The duration of OM was calculated as the end date minus the start date of occurrence of OM at or above a given grade. Members of the Biostatistics Program and Clinical and Translational Investigation Program of the Division of Pediatric Hematology/Oncology, Dana-Farber/Children's Hospital Cancer and Blood Disorders Center, contributed to the study design, data management, and statistical analysis for this study.
Results
Patient characteristics
The study enrolled thirteen patients with a median age of 15 years (range, 4.8–21.6), from May 2014 through October 2014, who were scheduled to undergo myeloablative HCT at Dana Farber Cancer Institute/Boston Children's Hospital (Table 1). Patients underwent allogeneic (n = 12) and autologous (n = 1) HCT for a variety of malignant and nonmalignant conditions, with the most frequent diagnosis being acute myelogenous leukemia (AML). All patients undergoing allogeneic HCT received a calcineurin inhibitor-based GVHD prophylaxis regimen, with more than half (n = 7) receiving cyclosporine and methotrexate.
Patient with neuroblastoma was the only patient who underwent autologous HCT.
AML, acute myelogenous leukemia; MDS, myelodysplastic syndrome; ALL, acute lymphoblastic leukemia; CML, chronic myelogenous leukemia; TBI, total body irradiation; ATG, anti-thymocyte globulin; HLA, human leukocyte antigen; GVHD, graft-versus-host disease; CNI, calcineurin inhibitor; MTX, methotrexate; MMF, mycophenolic acid.
Delivery of PBT
There were a total of 355 attempted treatment administrations; six were refused by three patients and two were not administered because of a technical complication with the device (the safety lock mechanism was activated accidentally), resulting in 347 treatment administrations (97.7%; Table 2). The full schedule of daily PBT treatments (including all six exposed sites at every treatment) was completed in approximately half of patients (7/13, 54%). Overall, PBT was delivered completely (i.e., all six exposed sites) in 316/347 treatments (91%), and at least in part (i.e., at least one of the six sites) in all 347 treatments (100%). Reasons for incomplete PBT included the patient being asleep (n = 12 treatment administrations), not feeling well (n = 5), patient refusal (n = 4), patient wearing an oxygen mask (n = 7), facial edema (n = 2), and unknown (n = 1).
Days on protocol defined as from the first day of hematopoietic cell transplantation conditioning through day +20 or hospital discharge if prior to day +20.
Days received treatment defined as days with treatment during any of the on-protocol days defined previously.
Cumulative dose defined as single treatment dose multiplied by the number of treatment sites (up to 6 in total) for each treatment session.
OM assessments
OM assessments were conducted by 10 trained nurses, with each involved with treating at least two patients, and one nurse providing treatment to all 13 patients. Out of the 355 attempted assessments, WHO and ChIMES assessments were rejected twice, once each by two different patients. The assessments were completed for both WHO and ChIMES 72% (254/353) of the time. The WHO score was obtained in 73% (257/353) of assessments, and the ChIMES score was obtained in 81% (287/353) of assessments. Incomplete OM assessments (WHO = 96, ChIMES = 66) were universally attributed to evaluators accidentally skipping questions. One patient refused OM assessments at two separate visits.
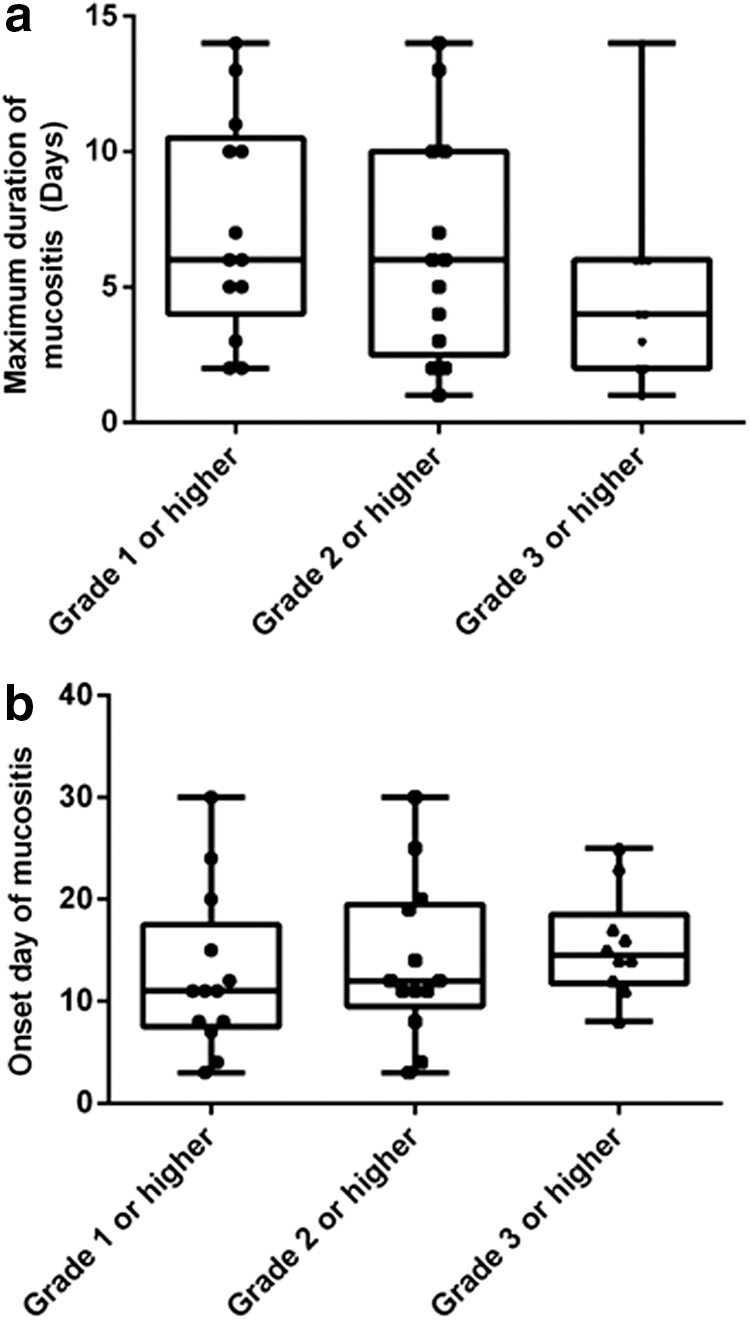
All patients experienced OM (WHO ≥1), with a median onset of day +11 (range, 3–30; Table 3, Fig. 2). Severe OM (WHO ≥3) occurred in 10 patients (10/13, 77%), with a median onset of day +14.5 (range, 8–25) and a median duration of 4 days (range, 1–14). The longest duration of OM experienced by a patient was 14 days; by site, the OM lasted the longest (11 days) in the right buccal mucosa, floor of month, and soft palate. The most frequently affected site was the floor of mouth (72/255, 28%).
Summary of World Health Organization (WHO) Oral Toxicity scores.
For the per-patient maximum ChIMES Percentage Scores, the median was 0.7 (range, 0.1–1.0). For the per-patient maximum ChIMES Total Scores, the median was 17 (range, 2–22).
Feasibility end-points
The 10 nurses completed an end of treatment questionnaire for each patient in whom they conducted an OM assessment and/or delivered PBT (Table 4). The study nurses reported that the training was effective (10/10, 100%), the device was accessible (10/10, 100%), the device was sufficiently maneuverable (10/10, 100%), and the device was sufficiently lightweight and administrable (10/10, 100%). In 2 of 355 treatment administrations, the device appeared to malfunction; however, the safety shutoff switch was accidentally activated and the study nurse did not know how to restart the unit. According to the prespecified protocol criteria that the upper limit of the CI on the proportions of these feasibility end-points exceed 75%, the external PBT protocol (delivery of therapy and completion of assessments) met the criteria for feasibility.
The emergency shutoff switch was inadvertently activated and the operator did not know how to restart the unit.
For each patient, only the highest score (highest level of discomfort) from all treatment administrations was reported. In all cases for which a score of >0 was reported, the pain was attributed to existing mucositis and not directly attributed to the device therapy (data not shown).
IQR, interquartile range; PBT, photobiomodulation therapy; WHO, World Health Organization.
The accrual-related feasibility end-point (five patients within the first 3 months of activation) was achieved and exceeded, with seven patients enrolled during this period. The median proportion of days with all data submitted was 100% (95% CI: 96.2–100%; Table 4), and data were reported for all 13 patients on ≥95% of days. Patients reported a median comfort score of “0” after delivery of PBT (range, 0–8, where 0 = no discomfort).
Discussion
In this study we demonstrated the feasibility of delivering daily external PBT for the prevention of OM in children undergoing HCT. Although the study was not designed to evaluate efficacy of the intervention, the therapy was found to be easy to deliver by trained nurses and was well tolerated by pediatric participants. These results suggest that with appropriate training and resources, this protocol could be implemented at other pediatric HCT centers, for example in the context of a multicenter trial.
All of the predetermined feasibility measures were achieved. The study nurses, responsible for delivery of external PBT, universally reported no difficulties in access and administration of the PBT device. In the instance when the device would not function because of a safety switch being activated, it was recognized that the study nurse training program did not highlight or address this device feature. Participants similarly reported high tolerability of (and in many cases enthusiasm for) external PBT, with 91% of planned treatments completed. With respect to data collection, the mean proportion of days with all data submitted greatly exceeded the goal of 75%, and the study accrued faster than expected. The pediatric HCT clinical staff at Dana-Farber Cancer Institute/ Boston Children's Hospital was highly supportive of this protocol, and we would anticipate similar outcomes at other pediatric HCT centers.
Despite demonstrating feasibility, this protocol presented some logistical challenges. When there was more than one subject on study it was very time consuming for the study nurses to administer the PBT therapy and to conduct the assessments. Although PBT administration required minimal subject participation, subjects had to be awake and alert during the OM assessments. If the subject was asleep, the nurse had to return at a later time to complete the assessments, adding more time to the daily protocol. Despite training, there were errors with the completion of study forms, which could be attributed in most cases to nurses inadvertently skipping required questions. There were 31 incomplete treatments for a variety of reasons such as patients being asleep, not feeling well, and being uncooperative. Although the training was found to be effective, it was not sufficiently complete. Failing to explain all of the device components and features, including the function of the safety switch, resulted in two missed PBT treatments despite an otherwise fully functioning device. A more comprehensive training module as well as providing the study coordinator's immediate contact information in case of any technical problems may have prevented any missed administrations.
This study's primary aim was to assess feasibility; therefore, the planned sample size and study design were understandably not sufficient for evaluation of the efficacy of the intervention. All participants received external PBT from the 1st day of conditioning until day +20 or discharge, and >91% of scheduled treatments PBT were completed at all six anatomic sites. Any grade OM (WHO ≥1) developed in all patients with a median onset of day +11 (range, 3–30). Severe OM (WHO ≥3) occurred in 10 patients (10/13, 77%), with a median onset of day +14.5 (range, 8–25) and a median duration of 4 days (range, 1–14). A meta-analysis by Vagliano et al. that collected data from 1841 pediatric patients (ages 0–18) undergoing allogeneic HCT under various conditioning regimens, including reduced intensity regimens, between 2002 and 2006 found that 57.0% of patients developed any grade mucositis and 27.6% developed severe mucositis, when no mucositis interventions were provided. 1 Although our small study population had a higher incidence of all grades of mucositis, all subjects underwent fully myeloablative conditioning regimens. Furthermore, the extraoral PBT device parameters were developed based on a series of assumptions that may not have been accurate. Therefore, careful dose modelling of extraorally delivered PBT for prevention of oral, oropharyngeal, and esophageal mucositis is indicated prior to the design of future clinical trials.
There is increasing evidence that supports the safety and efficacy of PBT for the prevention of OM. The Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC-ISOO) Mucositis Guidelines classify PBT as a “recommended” method for the prevention of HCT-associated mucositis. 12 Although the majority of publications have reported on intraorally delivered PBT, provided in a spot-by-spot manner throughout the oral cavity, a small subset has described extraorally delivered PBT, including the use of larger LED arrays which appear to induce the same biological activities as coherent laser light. 13 The potential advantages include fast and simple administration, and the avoidance of intraoral manipulation. Extraorally delivered PBT may be also more feasible in young children who have a smaller oral opening and behavioral challenges with intraoral delivery. Whelan and Hodgson have reported the effectiveness of LED-based PBT applied extraorally with purportedly good penetration through skin and soft tissue to the oral (and esophageal) mucosa. 6,7 Whelan et al. conducted a double-blind sham-controlled study of preventive LED PBT in pediatric patients undergoing myeloablative HCT. 7 The overall incidence of ulcerative OM was 53%, and there was a 48% and 39% reduction of treated left and right buccal pain, respectively, compared to untreated throat pain at day +7 (p < 0.05). Hodgson et al. conducted a randomized, double-blinded, placebo controlled trial of extraoral PBT (670 nm LED array with a power density of 50 mW/cm2 for 80 sec, resulting in an energy delivery of 4J/cm2 to the right and left face and anterior throat tissues with a total dose of 12 J/cm2/treatment) for the reduction of OM-related oral pain in children and adults undergoing HCT. 6 There was a statistically significant reduction in patient-reported pain (p < 0.05) at day +14 according to the WHO Oral Toxicity Scale criteria in the regular but not the low risk groups, and there were no statistically significant differences in any of the other measures.
Conclusions
In summary, this single center trial demonstrated the feasibility of delivering daily external PBT for the prevention of OM in pediatric patients undergoing HCT. As all of the feasibility end-points were met, we believe that these findings would likely extend to other pediatric HCT centers. The overall design of this protocol should be easily adaptable into a larger, multicenter trial designed to determine efficacy of this novel intervention for the prevention of OM.
Footnotes
Acknowledgments
The authors acknowledge Dr. Leslie Lehmann, Dr. Michelle Lee, Theresa Williams, and the Boston Children's Hospital Hematopoietic Stem Cell Transplant nursing staff for their work on this protocol, which contributed greatly to the success and rapid completion of the study. The authors also thank THOR Photomedicine Ltd (Chesham, UK) for providing the photobiomodulation therapy device utilized in this study.
Author Disclosure Statement
No competing financial interests exist.