
Abstract
Introduction
L
With the recent advances and development of a wide range of laser wavelengths, researchers suggest that lasers could be applied for dental treatment, including periodontal, restorative, surgical, and orthodontic treatments. 3 –5 Low-level laser therapy (LLLT) is a light-source treatment that generates light with a single wavelength, and it acts through a nonthermal, photochemical reaction in the cells. It has been postulated that the photobiological action mechanism of LLLT is generated via activating of the respiratory chain. Primary photoacceptors are terminal oxidases (cytochrome c oxidase on eukaryotic cells) as well as NADH-dehydrogenases (for the blue-to-red spectral range), with a crucial role in cellular bioenergy. 6,7 The review of de Paula et al. 8 supports the hypothesis that LLLT can modulate the periodontal inflammatory process mainly by reduction of the prostaglandin E2 (PGE2) release. It seems that different pathways in inflammatory modulation take place. LLLT influences the expression of cyclooxygenase (COX)-2 and interleukin-1beta (IL-1β), as well as matrix metalloproteinase (MMP)-8, platelet-derived growth factor (PDGF), transforming growth factor (TGF)-β, basic fibroblast growth factor (bFGF), and plasminogen. 9 –11 Beneficial effects of LLLT were only observed when LLLT acted as a coadjuvant to traditional periodontal treatment. Therefore, LLLT is emerging as a useful tool to modulate the chain of biological processes triggered during orthodontic treatment. 12,13
During orthodontic treatment, oral hygiene may be more difficult to maintain, which may lead to plaque accumulation by facilitating gingivitis, gingival enlargement, an increase in the pocket probing depth, and bleeding on probing. 14 –16 In the literature, there are some reports about the periodontal effects of fixed labial orthodontic treatment, for example, 15,17,18 but there are few reports on the periodontal implications of lingual orthodontic treatment in adults, 19,20 and even fewer that consider inflammation and LLLT. Lingual orthodontic treatment retains more plaque, generating more gingival inflammation than buccal orthodontic treatment (the lingual surface is smaller than the buccal one; therefore, the bracket takes most of the space, remains closer to the gingiva, thus impeding plaque removal). 21 The use of LLLT can be a strategy to consider in these cases, modulating inflammation and maintaining periodontal health during fixed lingual orthodontic treatment. Therefore, the objective of the present work was to estimate the short- and medium-term effects of repeated doses of LLLT on periodontal status in lingual orthodontic patients.
Methods
Population screening
Twelve orthodontic patients (six females and six males; mean age 37 ± 9 years) scheduled for fixed lingual orthodontic treatment were selected. All patients were right-handed, had permanent dentition, showed healthy periodontium, and were free of dental plaque. Patients who were excluded met the following criteria: (1) smoking, (2) being pregnant or lactating, (3) receiving antimicrobials or anti-inflammatory drugs in the last 3 months or during this treatment, (4) had received periodontal treatment within the last 6 months, (5) had received extensive dental restorations or prosthesis, (6) had any systemic disease (cardiovascular, diabetes, HIV, or metabolic or endocrine diseases, among others) that could affect the periodontium, or (7) being left handed.
Power calculation was determined by the use of a statistical package SAS 9.01. The analysis indicated that 12 subjects (12 upper quadrants treated with laser, 12 upper quadrants untreated with laser) would provide 80% power to detect a true difference of 1 mm using probing depth (PD) increase in pockets as the primary outcome variable and assuming a standard deviation of 0.6 mm, using a paired test (because the two quadrants studied are the same person's) with a level of bilateral significance of 0.050. 22
The study protocol was approved by the Ethics Committee of the Hospital Clínico San Carlos in Madrid, Spain (dated June 2014; internal code: 14/204-E).
Prophylaxis and oral hygiene program
Fifteen days before the orthodontic treatment, patients received supragingival prophylaxis and oral hygiene instructions (OHI). After these 15 days, patients were examined to see if they met the study inclusion criteria. Removal of supragingival plaque was initially performed with ultrasonic instruments (SONICflex 2003, KaVo Dental, GmbH, Biberach, Germany).
Then, all patients were taught the Bass brushing technique as well as how to distinguish between the presence and absence of bacterial plaque on tooth surfaces. They were also taught how to use dental floss or interproximal brushes. Patients did not use mouth rinses during the course of the study.
The prophylaxis procedure was repeated at the follow-ups of 1, 2, 3, and 12 months, at which point OHI were again reinforced.
Clinical measurements
Before the insertion of a lingual orthodontic device and at the follow-ups of 1, 2, 3, and 12 months, clinical periodontal parameters, such as visible plaque index (VPI), bleeding on probing (BOP), and PD, were measured dichotomously at six sites per tooth (mesiobuccal, buccal, distobuccal, distolingual, lingual, and mesiolingual) on all teeth of the upper arch by one calibrated periodontist who was not involved in providing treatment during the study.
The VPI was evaluated before measuring the PD. The PD measurements, in mm, were performed using a manual periodontal probe (PCP 12, Hu-Friedy Instrument Co., Chicago, IL). The BOP was scored 20 sec after probing.
The examiner underwent calibration training at the beginning of the study. For that purpose, five subjects, not related to the study and each showing two pairs of contralateral teeth with PD >5 on at least one aspect of each tooth, were tested. The examiner evaluated PD of these teeth in these subjects twice within an interval of 48 h. Calibration was accepted if the percentage agreement between both measurements was >96%.
Gingival crevicular fluid (GCF) samples
GCF samples were collected before the insertion of the lingual orthodontic appliance, and at of 1-, 2-, 3-, and 12-month follow-ups, in the mesiolingual and distolingual sites of the maxillary first premolar and maxillary first molar teeth. GCF was collected with prefabricated paper strips (Periopaper, Oraflow Inc., Plainview, NY), which were placed into the sulcus until there was slight resistance. After keeping the strip in place for 30 sec, the absorbed volume was measured with a Periotron 8000 (Oraflow Inc., Plainview, NY). 23 The periopapers were then placed in sterile Eppendorf vials with a filter, and immediately stored at −80°C until analysis was performed.
Orthodontic treatment
All patients presented with a moderate lack of space with the correct anteroposterior and transverse relationship, justifying the nonextraction treatment management. The orthodontic treatment was performed with the new STb™ Lingual Straight Wire technique (Ormco Corporation, Glendora, CA) (Fig. 1).

Appliances used for orthodontic lingual treatment.
LLLT
Immediately after bracket placement, patients received laser radiation in quadrants 1 or 2 (with a sequence randomly determined by the computer). The laser used (Periowave™, Ondine Biopharma Corporation, Vancouver, Canada) was a continuous wave diode laser device operating at a 670 nm wavelength, 190 mW of output power [checked before each laser session by a power meter (UNO Laser Power Meter by Gentec-EO)], and 6.05 W/cm2 of irradiance, and equipped with a flexible fiberoptic cable attached to a custom-designed stainless steel autoclavable handpiece. To access to the periodontal pocket, this handpiece accommodated a disposable light-diffusing tip, which was partially inserted into the sulcus and gently moved along it to deliver the laser radiation, (being the target of irradiation GCF and sulcular epithelium), for no longer than 60 sec/tooth (30 sec for the buccal surface and another 30 sec for the lingual surface and its interproximal sites) (Fig. 2). Table 1 a detailed description of the laser system and laser parameters used in this study. The laser tip was discarded after each laser session. Laser treatment was repeated six times in 2 weeks (days 3, 4, 5, 10, 11, and 12) and once at the follow-ups of 1, 2, 3, and 12 months, with the same methodology. To avoid potential subjective confounders, on the contralateral quadrant (control side), the light-diffusing tip was partially inserted into the pocket, without applying laser radiation. The patient, operator, and dental assistants wore protective eyeglasses during the laser application.
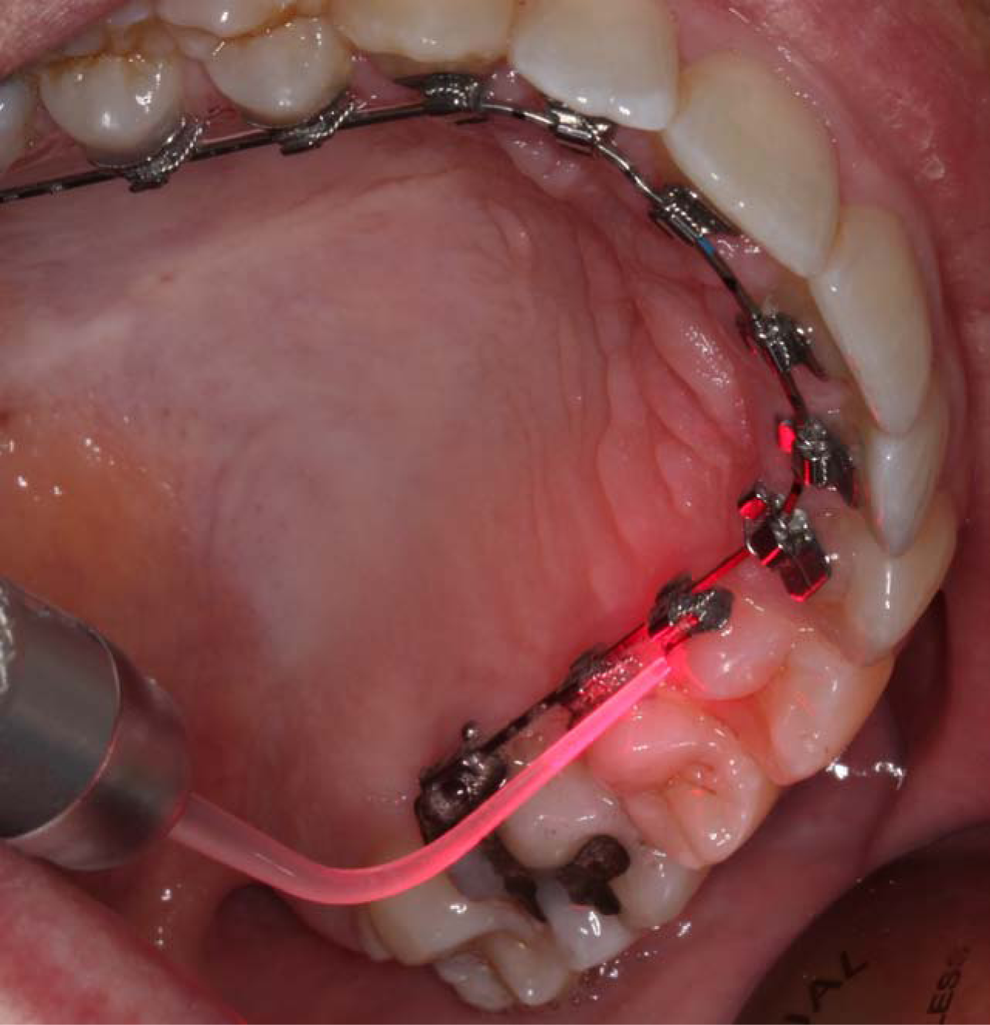
Light-diffusing tip inserted into the periodontal pocket delivering diode laser radiation. During the illumination cycle, the diffusing tip was slowly moved around the pocket.
Measurement of cytokines from GCF
By using enzyme-linked immunosorbent assay (ELISA), diluted GCF samples were analyzed. The levels of IL-1β and tumor necrosis factor alpha (TNF-α) in GCF were determined (in duplicate) with a human IL-1β ELISA KIT (cat. No: 850.006.192) and human TNF-α ELISA kit (cat. No: 950.090.192), respectively, which were both from Diaclone SAS (Besançon Cedex, France), according to the manufacturer's instructions. The results were calculated using the standard curves created for each assay. The cytokine concentrations were corrected for the GCF volume and defined in pg/μL. The detection limits were determined as 6.5 and 8 pg/mL for IL-1β and TNF-α, respectively.
Statistical analysis
Statistical analyses and calculations were performed with SPSS for Windows software (version 15.0; SPSS, Chicago, IL).
First, to assess the normality of data, we used the Shapiro–Wilk test. We used analysis of bifactorial variance (ANOVA) for repeated measurements to evaluate the PD, GCF, IL-1β, and TNF-α levels, (p < 0.05). Post-hoc pairwise tests were implemented as a paired t test with a correction according to the Bonferroni test (for each of the variables evaluated, contrasts between the Laser Group and the Control Group were conducted at each of the five evaluation times, then every p value obtained was multiplied by five to see if it was significant, <0.05). For the VPI and BOP values, the nonparametric Friedman test for repeated measurements was used. When the Friedman test was significant (p < 0.05), pairwise comparisons based on the Wilcoxon rank test were made, implemented with Bonferroni correction.
Results
Evolution of the periodontal index scores during the period of evaluation are shown in Figs. 3 and 4. VPI, BOP, and PD scores generally increased along the evaluation period in both groups. The scores increased more in the Control Group, mainly at the lingual side. A clear increase of VPI scores was observed until the follow-up at the 3rd month (increments of 4.67% and 6.22% from baseline at the lingual side in the Laser and Control Groups, respectively). In both groups, at medium term (at the follow-up at 12 months) values increased from those obtained at the follow-up at 3 months only on the lingual side (Fig. 3A). BOP scores slightly increased during early revision periods (Fig. 3B). At medium term, BOP scores showed a larger increase in all localizations, but mainly on the vestibular and lingual sides in the Control Group (increments of 5.92% and 6.54% from baseline, respectively) (Fig. 3B). In both groups, values of PD continuously increased at the lingual side until 3 months after the beginning of the orthodontic treatment, and they decreased in the following 9 months (probably because of a better adaptation of the periodontal tissue to forces applied), although values maintained the same intergroup difference (0.3 and 0.2 mm at the 3rd and 12th month follow-ups) (Fig 4). The GCF values were slightly elevated during the observation period, mainly in the Control Group, but there were no significant differences between the groups (Table 2).
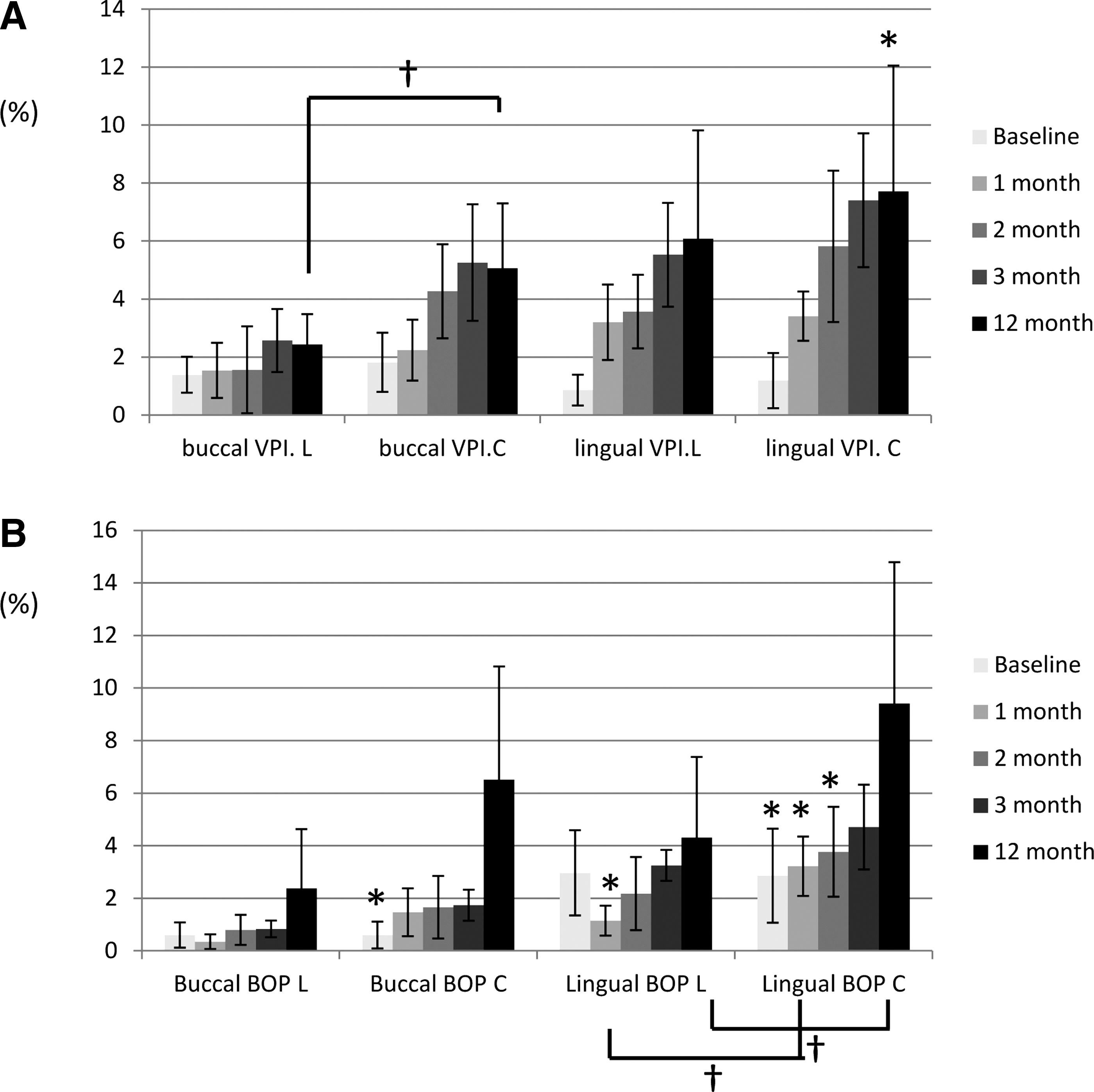
Periodontal scores (visible plaque index [VPI] and bleeding on probing [BOP]) at the buccal and lingual sides, mean scores ± SD; n = 12, at baseline and at 1, 2, 3, and 12 months after treatment with fixed lingual appliances. (L) Laser Group, (C) Control Group.

Probing depth (PD) (mm) at the buccal and lingual sides, mean scores ± SD; n = 12, at baseline and at 1, 2, 3, and 12 months after treatment with fixed lingual appliances. (L) Laser Group, (C) Control Group. *Statistically significant intragroup differences between marked values and those obtained at 3 month reevaluation (p < 0.05). †Significance of statistically significant intergroup differences (p < 0.05).
Values are shown as the mean ± SD of 12 patients.
Statistically significant differences were not found.
GCF, gingival crevicular fluid; LG, Laser Group; CG, Control Group.
Levels of IL-1β in the GCF were increased immediately after the placement of the orthodontic device (Fig. 5A). In the Laser Group, high IL-1β levels were observed at 1 month after the start of the orthodontic treatment, and they were maintained during the 2nd and 3rd months. The levels of IL-1β increased progressively in the Control Group, resulting in higher levels at the 2nd and 3rd months after the beginning of the orthodontic treatment, which were significantly different from the Laser Group levels during the same evaluated period (85.98 pg/μL in the Control Group compared with 59.93 pg/μL in the Laser Group at the 2nd month follow-up; 80.59 pg/μL compared with 61.26 pg/μL at the 3rd month follow-up) (Fig. 5A). At the 12-month follow-up, levels of IL-1β in GCF decreased and returned to starting values in the Laser Group. In the Control Group, they decreased further than in the Laser Group, but they reached values somewhat higher than baseline.
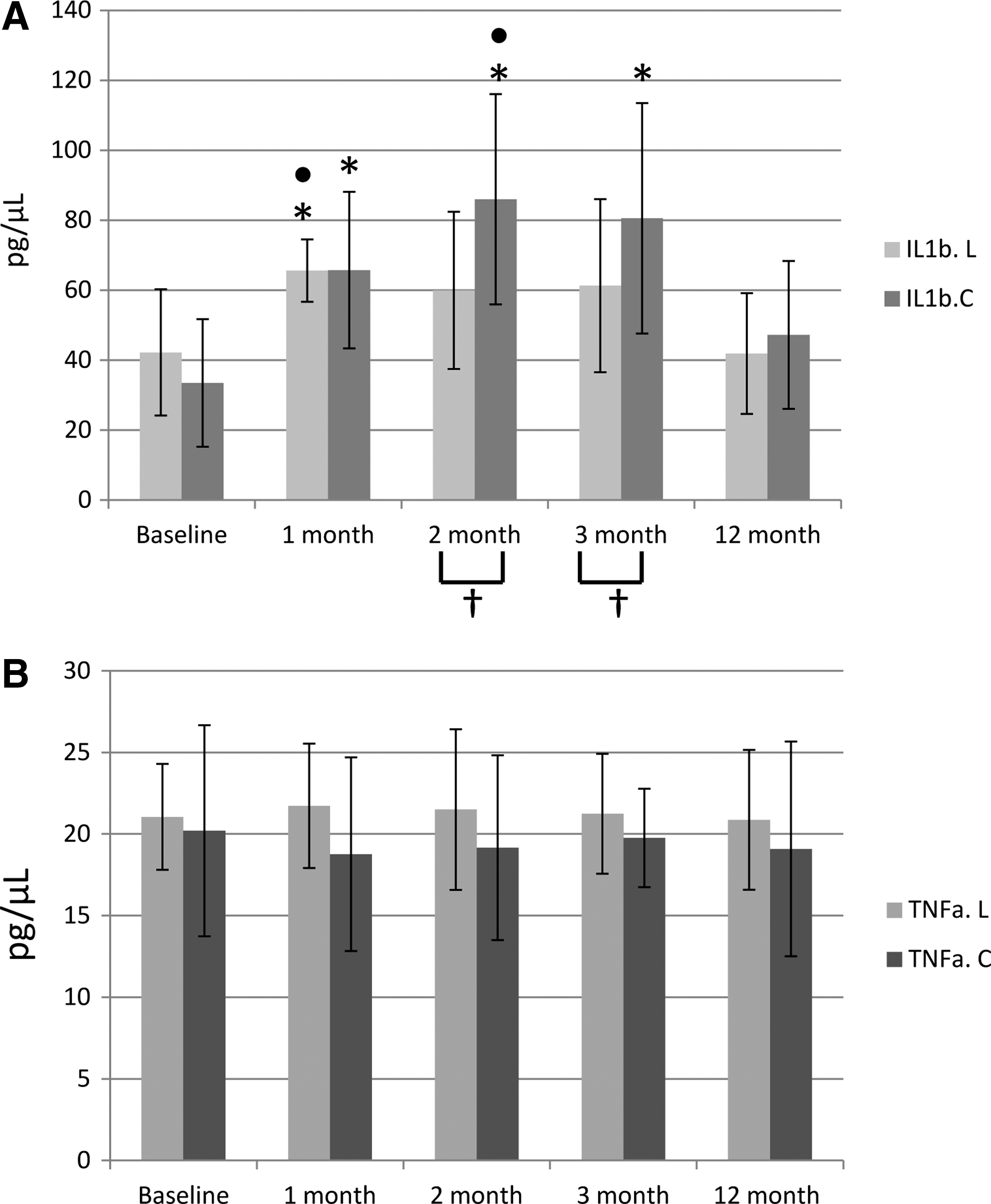
Effects of the fixed lingual orthodontic treatment and laser radiation in the interleukin-1beta (IL-1β) (
The levels of TNF-α remained constant throughout the study and did not show any intragroup or intergroup statistical significance (Fig. 5B).
Discussion
Previous studies showed that the greatest periodontal alterations were at 3 months after orthodontic bonding. 24,25 The present study was performed beyond this specific period of 3 months to detect the time when the maximum increase of the periodontal parameters took place. As patients showed a healthy periodontium and gingival recessions were not observed immediately before or during orthodontic treatment, PD scores were measured to evaluate gingival inflammation instead of clinical attachment level (CAL) scores.
Although split-mouth design has been the principal research tool in periodontal clinical trials to compare different treatment modalities, this design has the problem of being unable to truly separate the effects between the experimental and control groups. In the present study, laser radiation was directly delivered into the sulcus by a light diffuser tip configured as a periodontal probe generating a spot of <2 mm in diameter. Because a highly focused low-level laser radiation is employed here, the effects are exclusively local without affecting the surrounding tissues.
Demling and coworkers reported that the insertion of fixed lingual appliances without supportive dental prophylaxis induced a worsening of the periodontal index scores restricted to the lingual sites. 20 Lingual plaque formation after that lingual orthodontic treatment was in accordance with other clinical studies that evaluated plaque formation after buccal orthodontic treatment, demonstrating higher plaque levels during fixed orthodontic treatment, which were associated with an increase in PD and BOP. This effect was restricted to sites where the orthodontic device was placed (lingual in the study reported by Demling et al. and buccal in the studies of Glans et al.). 20,26 Gray and Mclntyre concluded that oral health promotion (OHP) for patients undergoing fixed appliance orthodontic treatment produces a short-term reduction (up to 5 months) in plaque, and improvement in gingival health. 27 Results from the present work show that the effect of the placement of the lingual orthodontic device was in part counteracted by both the photomodulatory action of LLLT and the practice of routine OHI, which blocked significant increases in the VPI, BOP and PD scores.
Analysis of specific biochemical indicators present in the GCF is a good option for evaluating the local cellular metabolism, reflecting the periodontal health status and bone remodelling process during orthodontic treatment. 28,29 Orthodontic forces represent a physical agent capable of inducing an inflammatory reaction in the periodontium. This reaction is necessary for orthodontic tooth movement; however, an excessive inflammatory reaction can delay this movement. Light continuous orthodontic force tended to maintain relatively high IL-1β levels for a longer period and, therefore, may reduce the frequency of reactivation. The relatively longer-lasting levels of induced cytokines are needed for continuous periodontal remodeling. 30 Studies in periodontics confirm that IL-1β is effective for evaluating the periodontal inflammation and can be used as a laboratory tool for assessing the activity of periodontal disease. 31 The periodontal benefits of LLLT have been described in previous studies in terms of greater reduction of PD, bleeding sites, and periodontal inflammation, decreasing IL-1β levels in the GCF 32,33 even in the 1st month of implementation. 32 In the present work, lingual orthodontic treatment increased the IL-1β levels in GCF and the LLLT counteracted this effect by modulating these levels, resulting in values statistically different between the Laser and Control Groups at the 2nd and 3rd months after lingual orthodontic bonding. Likewise, it is important to point out that the clinical values obtained for PD in the lingual side at the 3rd month follow-up correlated with IL-1β levels in GCF, coinciding with the time in which the greatest periodontal alterations are expected.
Karacay and coworkers studied the TNF-α levels in GCF after the placement of a hybrid retractor for moderate distalization of upper canines, applying a continuous force. These levels increased at 24 h and declined at 1 week. The reason for this decrease might be the adaptation of the tissues to light, continuous force at 1 week. 34 The application of heavy forces causes hyalinization tissue with rapid and increased production of TNF-α. 34,35 The possible adaptation of the tissue to the light continuous force, a healthy periodontium, and good OHI could impede the effect of LLLT on TNF-α modulation and could be responsible of the constant levels of TNF-α in GCF obtained.
Conclusions
LLLT did not exert major effects, but some small effects were significant at some follow-up times (as for clinical parameters: BOP, PD, and for IL-1β levels in GCF). In the model used, there was some increased normal range inflammation as a result of both the subgingival plaque accumulation (despite the low percentage accumulated) and the periodontal tissue remodeling that is incident to the orthodontic tooth movement. This “subclinical” inflammation cannot be excluded and could be responsible of these positive biostimulation effects.
According to the obtained results, additional treatment with LLLT slows the slight periodontal deterioration that is intrinsically caused by the lingual orthodontic treatment, and has a beneficial effect in controlling periodontal inflammation on a short-term basis, as assessed by the IL-1β levels in GCF. At medium term, LLLT diminished VPI, BOP, and PD scores, allowing for a faster recovery of the initial periodontal status.
Footnotes
Acknowledgments
This research was supported by a grant from the Eugenio Rodriguez Pascual Foundation, Madrid, Spain, and by the Spanish Research Project from Ministerio de Ciencia e Innovación (MICINN) (Ref.:MAT2014-51937-C3-1-P). The authors thank Di&B Spanish Enterprise for lending the Periowave™ System.
Author Disclosure Statement
No competing financial interest exist.