
Abstract
Introduction
P
Periodontal pathogens are known to be involved in peri-implantitis infections. 4 –6 Consequently, the treatment of peri-implant disease is based on the reduction of the infection. 7 Reduction of the bacterial load present at peri-implant tissues and at implant surfaces is desirable. Several approaches to the detoxification of implant surfaces have been described with the objective of eliminating bacterial contents. Mechanical debridement, disinfection with chemotherapeutic agents, smoothing implant surfaces, and open flap surgeries with mechanical debridement and implant surface detoxification are the most common therapies found in the literature. 3 However, the aforementioned techniques may cause alterations to implant surfaces and could facilitate bacteria absorption and biofilm formation. 3
Zirconia is a biocompatible material that is sufficiently strong to be used as a substitute for titanium dental implants. 8 Zirconia abutments are better than metallic abutments because they present aesthetic improvements 9 and lower bacterial adhesion. 10 Blood flow in tissue surrounding zirconia abutments has been reported to be similar to blood flow in soft tissue around natural teeth. 11
An earlier review suggested the use of lasers in different fields of implantology. 12 Some lasers emit pulses on a microsecond scale, thus making them effective in transforming light into heat and promoting a photothermic ablative capability in tissue without heat propagation to surrounding tissues. 13 Several laser wavelengths have been reported reported in peri-implantitis treatment: the neodymium-doped yttrium aluminum garnet (Nd:YAG) laser (1064 nm), the the gallium aluminum arsenide (GaAlAs) diode laser (980 nm in wavelength), the carbon dioxide laser (CO2) (10600 nm), the erbium (Er):YAG laser (2940 nm), and the erbium chromium doped: yttrium, scandium, gallium, and garnet (Er,Cr:YSGG) laser (2780 nm). 2,3,14 –16 In vitro models have proven the efficacy of Er:YAG, CO2 and diode lasers in high or even complete elimination of bacteria-loaded titanium disks. 10
According to Romanos et al., a variety of therapeutic modalities also have been proposed for the management of peri-implantitis, such as antiseptics and/or antibiotics, laser therapy, guided bone regeneration, and photodynamic therapy. 2
The diode laser has been investigated as an adjunct to conventional scaling in the nonsurgical treatment of peri-implantitis. 17,18 Lasers can irradiate the entire surface, especially in irregular and rough areas where mechanical instruments cannot easily reach. 18 A literature review by Ashnagar et al. demonstrates the necessity of clinical studies to evaluate soft tissue to assess the efficacy of this treatment option, possible side effects of photo-thermic effects on surrounding tissues, and periimplant pockets. 3
The absorption peak, the device operation mode, and the tissue characteristics influence the thermal increase during laser irradiation. A classic pre-clinical study observed that a temperature increase to 50°C for 1 min induced vascular injury, and a temperature increase to 60°C resulted in blood flow cessation and bone necrosis. 19 An in vitro study concluded that the irradiation of implant surfaces with diode lasers might produce a temperature increase above the critical threshold (10°C) for bone safety after only 10 sec. 20 A temperature increase of 10°C could compromise bone vitality. 19 –21
The objective of this study was to investigate the effects of diode laser irradiation on the temperature and surface roughness of yttria-partially-stabilized zirconia (Y-TZP), machined titanium (TI), and sandblasted large grid and acid-etched titanium disks (SLA).
Materials and Methods
Specimen preparation and laser system
The standardized disks with 5 mm diameter and 2 mm thickness of zirconia (Y-TZP) (AS Technology Titanium Fix, Sao Jose dos Campos, SP, Brazil) were obtained from computer-aided design and computer-aided manufacturing (CAD-CAM) blocks. TI disks and SLA (AS Technology Titanium Fix, AS Technology, Sao José dos Campos, SP, Brazil) were used to determine three experimental groups (n = 10 per group).
Laser optical fiber (diameter 600 μm) was located parallel to the disk surface for 20 sec. The 808 nm diode laser (Thera Lase Surgery, DMC, São Carlos, Brazil) was used at 1 W in pulsating mode, 50 Hz, t on = 100 ms, t off = 100 ms, energy density = 28.29 J/cm2 in contact mode perpendicular, with 1W power on each disk (Table 1).
Means followed by different upper letters indicate statistical differences (p > 0.05).
One single operator previously calibrated uniformly irradiated each disk surface for 20 sec with manual grid movement.
Temperature and surface roughness evaluation
All measurements were performed at room temperature (23°C ± 1°C). The temperature was analyzed by a thermosensor attached to a digital thermometer (SmartMether, Novus, Porto Alegre, RS, Brazil) and fixed to the opposite side of the irradiated surface. The initial temperature was recorded immediately before the irradiation and final temperature was recorded immediately (1 sec) after irradiation. The temperature gradients (ΔT) were calculated (ΔT = final temperature − initial temperature) for each group. The medium ΔT (°C) and standard deviation were calculated for each group.
The surface topography was measured using a confocal light microscope (Leica Scan DCM 3D–Leica Microsystems Ltd, Switzerland) with objective magnification of 50×. All surface values were determined at a cutoff length of 0.2 mm in an area of 254.64 × 190.90 μm (768 × 576 pixels) (Sa in μm2 and Ra in μm) with Leica DCM 3D Dual Core profiler software (Leica Microsystems Ltd, Switzerland).
The mean Sa and Ra values were calculated from seven profiles from control (unirradiated) and test (irradiated) groups from zirconia disks (Y-TZP) and titanium disks (SLA). Superficial micromorphology images from the evaluated areas were obtained (50×).
It was not possible to evaluate the TI because the selected technique (confocal microscopy) did not allow for reading samples.
Statistical analysis
Data of temperature alteration (ΔT) was statistically analyzed by one way ANOVA at the 95% confidence level, and compared by Tukey post-hoc test (α = 0.05).
Data of roughness (Ra, in μm) and Sa (in μm2) was statistically analyzed by student t test (α = 0.05).
Results
Temperature alteration evaluation
Statistically significant differences among groups (p < 0.05) were observed using ANOVA. The initial temperature, final mean temperature (°C), ΔT (°C), and standard deviation obtained for each evaluated group are presented in Table 1.
The diode laser irradiation had a ΔT value of 10.3°C on zirconia disks. TI disks had a ΔT value of 38.6°C and 26.7°C for machined and SLA titanium disks, respectively. The ΔT values were higher for the TI groups than for the Y-TZP group.
Surface roughness (Ra, in μm and Sa, in μm2)
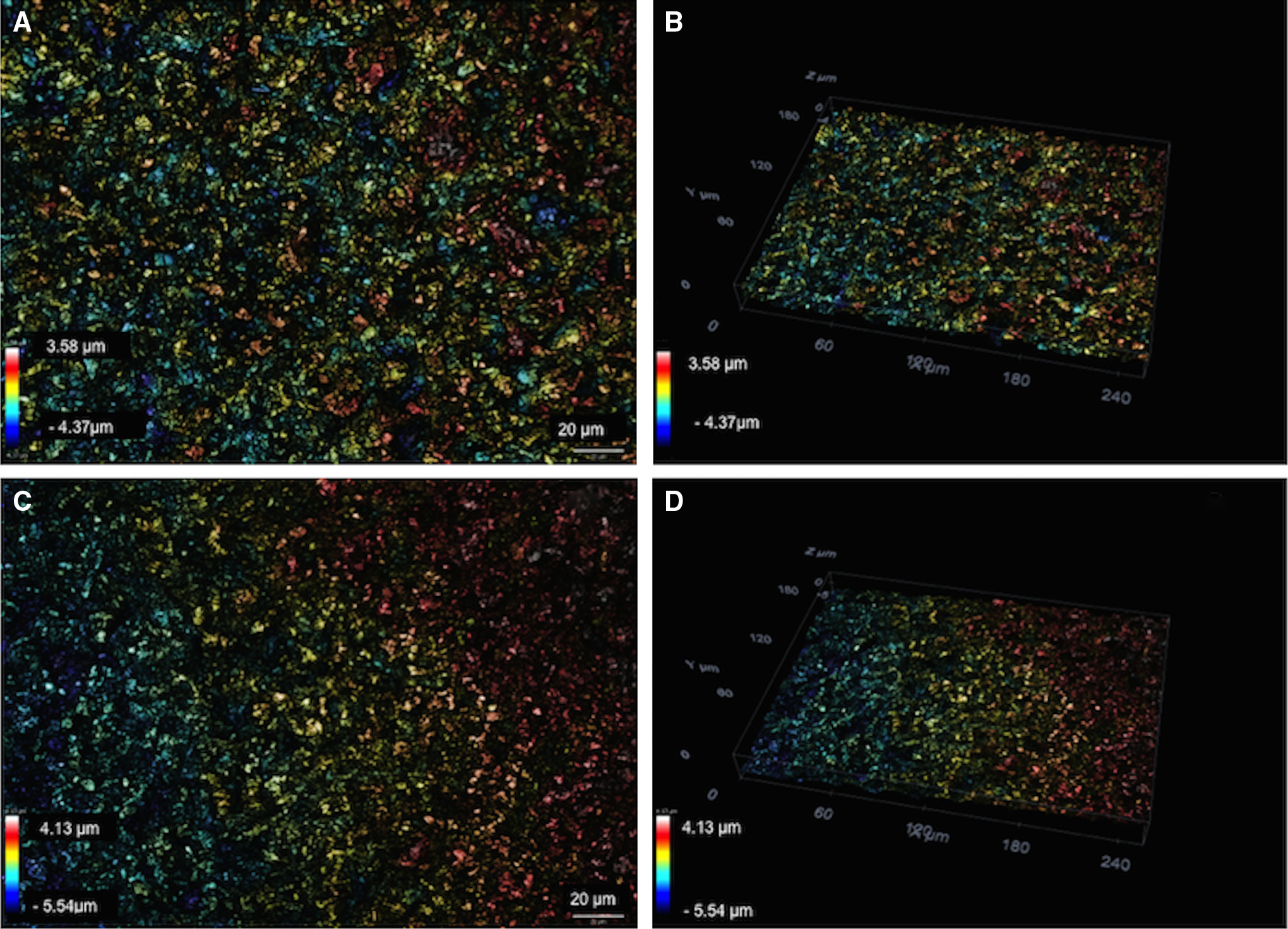
The roughness data did not show statistically significant differences in the “irradiation” factor (p > 0.05) of Y-TZP and SLA for both the Ra and Sa measurements.
The diode irradiation effects on the roughness values (Ra in μm) and standard deviations of evaluated groups are presented in Table 2.
Y-TZP, zirconia; SLA, sandblasted large grid acid-etched titanium.
The surface roughness values (Ra in μm) were not altered after laser irradiation (Table 2). The diode irradiation effects on the roughness values (Sa in μm2) and standard deviations of evaluated groups are presented in Table 3.
Y-TZP, zirconia; SLA, sandblasted large grid acid-etched titanium.
The roughness values (Sa in μm2) were not altered after laser irradiation (Table 3). The two-dimensional (2D) and three-dimensional (3D) images obtained from zirconia (Y-TZP) before and after diode irradiation are presented in Fig. 1.

Representative two-dimensional (2D)
The 2D and 3D images obtained from TI (SLA) before and after diode laser irradiation are presented in Fig. 2. There were no surface alterations, such as cracks or melted areas, with the selected parameters in the present study.
Representative two-dimensional (2D)
Discussion
TI has been used in oral implantology with high success rates. However, zirconia is a material that presents several advantages, such as low bacterial adhesion and biofilm formation, compared with other dental materials. 10 Therefore, TI and zirconia were chosen as the materials for this study. Although the machined TI is not currently used clinically, TI was included as a control to verify the effect of the surface treatment on temperature alteration. The findings indicate that the surface influenced the thermic conductibility, expressed by increased temperature of both zirconia and TI.
The 1 W diode laser interaction for 20 sec promoted a large increase in temperature on machined and sandblasted large grid acid-etched TI (26.7°C and 38.6°C, respectively) and a less- evident temperature increase (10.3°C) on the Y-TZP, demonstrating that temperature increase is material dependent. A previous report 22 evaluated the effects of the application of a diode laser (808 nm) to the radicular surface of extracted teeth and reported an increase of 1.6°C and 3.3°C with 1 and 1.4 W diode laser applications, respectively, for 30 sec.
Laser technology was used for the first time on soft tissue in 1988, and the development of laser devices has since increased. 23 A study of 45 patients by El-Kholey at al. compared the diode laser with traditional cold scalpel surgery in vivo and found no significant difference between the two methods in the duration of surgery, postoperative pain, time for healing, or success of the implants. 24 Geminiani et al. affirmed that the diode and Nd:YAG laser must be used with caution because of the penetration and possible bone damage. 19
The use of diode lasers on soft tissue surgery has been recently adopted in the field of dentistry. Device cost reduction contributed to the increased number of laser units installed for the purpose of soft tissue surgery. Lasers became “standard” tools for oral lesion excision; however, there is controversy about the control of the thermal damage to tissues. 25
Several methods are suggested for peri-implantitis, and clinicians must choose among a large number of different treatment protocols. 2,3 A systematic review to determine whether laser therapy is efficient for peri-implantitis concluded that the superiority of laser treatment could not be identified because of the heterogeneity and the low number of articles included. 26 Furthermore, despite the promising therapeutic results of peri-implantitis treatment, clinical studies of laser use have had short follow-up periods, and longitudinal studies with longer follow-up periods are required to determine clinical advantages. 3 Our data suggest that the diode laser did not alter the implant surface topography. However, the diode laser significantly increased the temperature. The effect of this irradiation on the disk surface is of significant importance to the study of cellular attachment and bone regeneration, and it should be addressed in further clinical studies.
Additionally, the evaluation of decontamination effects on zirconia surfaces demonstrated that, regardless of the implant material, the laser settings could be evaluated carefully, and both evaluated materials presented temperature changes >10-fold. This finding is important because recent pre-clinical and clinical data have shown that dental implants manufactured with zirconia demonstrated innovative clinical results comparable with TI and TI alloys. 27,28
The implant surface morphology should not be altered during the decontamination process. If superficial characteristics are altered because of inappropriate laser parameters, the reattachment of connective tissue to the implant surface can be affected. 14 The antibacterial effects of a diode laser (810 nm, 50 J/cm2) on Streptococcus sanguinis and Phorphyromonas gingivalis were observed by Hauser-Gerspach et al., without surface alteration on dental zirconia in vitro, in accordance with the findings of the present study on surface roughness. 10 The main disadvantages described are the increased thermal stress at peri-implant tissues, an aspect that can interfere with the process of osseointegration, and the possible structural changes of the implant surface. 13
Papadopoulos et al. compared the effectiveness of open flap debridement used alone with an approach employing the additional use of a diode laser for the treatment of peri-implantitis; no additional benefits with diode laser application were found. 27 Romanos et al. demonstrated negative effects for Nd:YAG laser irradiation compared with 980 nm diode irradiation of TI discs. 29
Because the thermal increase observed was >10-fold, special attention should be paid to the application time for the diode settings presented in this study.
Conclusions
Diode laser irradiation increased both zirconia and TI temperature without increasing surface roughness.
Footnotes
Author Disclosure Statement
No competing financial interests exist.