
Abstract
Introduction
T
In order to investigate the effect of the simultaneous application of BMSCs and LLLT on the healing rate of the osteochondral defects, an in vivo examination was conducted to compare the herapeutic effects of BMSCs alone and with low level laser on the healing rate of full-thickness articular cartilage defects histologically.
Materials and Methods
Animals
Ten adult male New Zealand white rabbits aged 10 months and weighing 2 ± 0.35 kg (mean ± standard deviation) were used. All animals were randomly coded and housed separately in large, well-lit standard cages and had ad libitum access to standard diet and tap water.
The experiment began after a 2-week period of adaptation. All protocols in this study were approved by the animal regulations and ethics committee of the AJA University of Medical Sciences (approval no. 68862).
Bone marrow sampling
Intramuscular injection of ketamine hydrochloride (50 mg/kg) and xylazine (10 mg/kg) was used for anesthetizing the rabbits. After shaving and disinfecting the region, 2–3 mL of bone marrow was aspirated from the humerus of the animals using an 18-gauge needle on a 10 mL syringe containing heparin (3000 U/mL) with the same code as the animal. All the procedures were carefully performed under sterile conditions.
MSC preparation
The coded bone marrow aspirates were suspended in 5 mL Dulbecco's Modified Eagle's Medium (DMEM) supplemented with 100 IU/mL penicillin (Sigma, USA), 100 IU/mL streptomycin (Sigma, USA) and 10% fetal bovine serum (FBS). Then the cells were cultured at 5 × 106 cells/cm2 in 75 cm2 culture flasks, in an atmosphere of 5% CO2 and 37°C. After 1 week, cells attached to the bottom of the flasks were washed by phosphate buffered saline (PBS) (Gibco, USA) and the culture medium was replaced with fresh DMEM. The flasks were incubated with a medium replacement of two times a week, until the cultures became confluent. At 60–70% confluence, second passage cultures of MSCs were washed with PBS and trypsinized with trypsin/ethylenediaminetetraacetic acid (EDTA) solution 0.2%. Finally, the cells from third passage were suspended in collagen type I (Koken, Japan) as a scaffold, at a density of 5 × 106 and moved for surgery. Morphological characteristics of cultured BMSCs in this study are illustrated in Fig. 1.

Note the fibroblastic-like appearance of the cultured bone marrow mesenchymal stem cells (BMSCs) as seen in these microscopic views (×100 magnification).
Surgical procedure
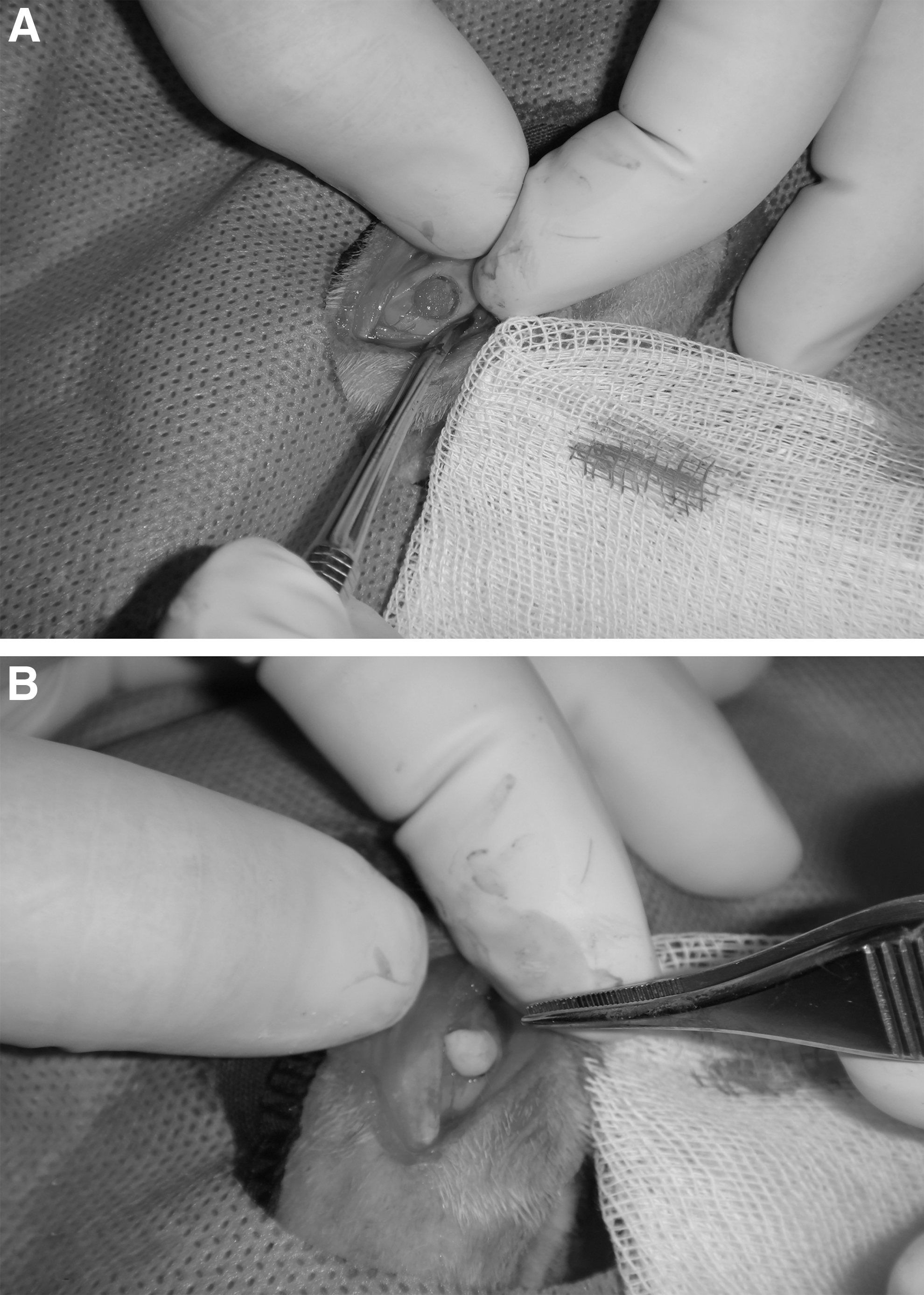
Animals were intramuscularly anesthetized using a mixture of ketamine and xylazine. After shaving and disinfecting the knee region, a 3 cm medial parapatellar incision was made in one knee and the patella was dislocated laterally. A full-thickness defect (4 mm in diameter, 3 mm in depth) was made on the articular surface of the patellar groove of the distal femur using a 4 mm diameter corneal trephine (Fig. 2A). After that, coded BMSCs/scaffold composite (4 mm thickness) was transplanted to the defect site of the animal with the same code and inserted by press fitting method (Fig. 2B).
Subsequently, the patella was repositioned and the wound was carefully closed in layers and the defect site was marked on the skin. The animals were allowed to move freely. This procedure was performed by an experienced person in both knees of all animals.
Photobiomodulation
As an experimental group, a knee in each rabbit was randomly selected for laser therapy. Laser therapy was initiated at the time of surgery and continued every other day for 3 weeks.
The animals were relaxed by administration of one-half dosage of anesthesia drugs during laser irradiation. A gallium-aluminum-arsenide (Ga-Al-As) diode laser device (THOR LX2, THOR International Ltd, UK) was used in this study. The laser specifications were: power density of 430 mW/cm2, energy density of 8.5 J/cm2, power output of 30 mW, wave length of 810 nm, continuous mode irradiation, and duration of 20 sec per session (Table 2). The laser was applied to two points around the marked point with the laser probe (each one for 20 sec) in contact with the skin, so the distance from the probe to the scaffold was ∼5 mm. The other knee served as control group and did not receive laser treatment.
Histomorphometric evaluation
After 3 weeks, all the animals were euthanized and the knee joints were removed, coded, and fixed in 10% buffered formalin solution (Fig. 3).
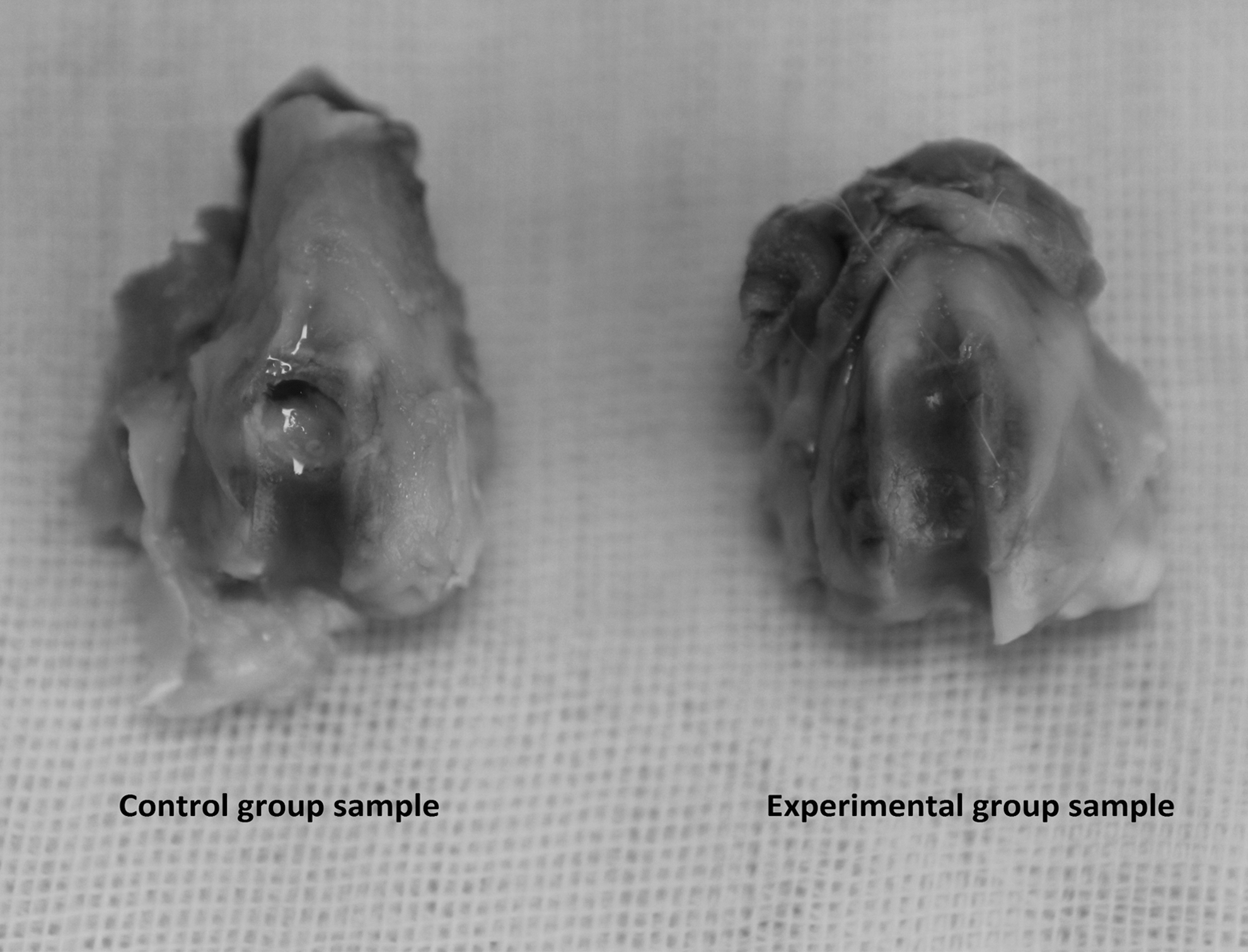
Gross appearance of knee joint in both group samples harvested at 3 weeks after surgery. Note the better filling of the osteochondral defect in the experimental group sample compared with the control group sample.
Then the specimens were decalcified by soaking in EDTA solution and then embedded into the paraffin wax. Histological sections were prepared sagittally and then stained with hematoxilyn and eosin. All the sections were evaluated by an expert person using a fluorescent microscope and a light microscope (Nikon, E 8400, Tokyo, Japan) with ×40 magnification. Photomicrographs were taken from different areas of the defects and the percentages of new cartilage formation, new bone formation, other tissue (such as connective tissue) formation, and measure of inflammation were calculated using Iranian histomorphometric analysis software (I HMMA_ver. 1, Sbmu, Iran).
Statistical analysis
All data were statistically analyzed using SPSS software (version 19.0.0; IBM, Chicago, IL). The means and standard deviations (SD) of new cartilage formation, new bone formation, other tissue formation, and inflammation were calculated for each group of defects. Considering a normal distribution of values, a one way ANOVA test was used to compare the data between two groups. p Values <0.05 were considered to be statistically significant.
Results
Clinical observations
All the animals normally recovered after the surgical procedure. The surgical zone repaired itself normally and no complication was observed during the study. Therefore, 20 samples were subjected to histological evaluation.
Histological analysis
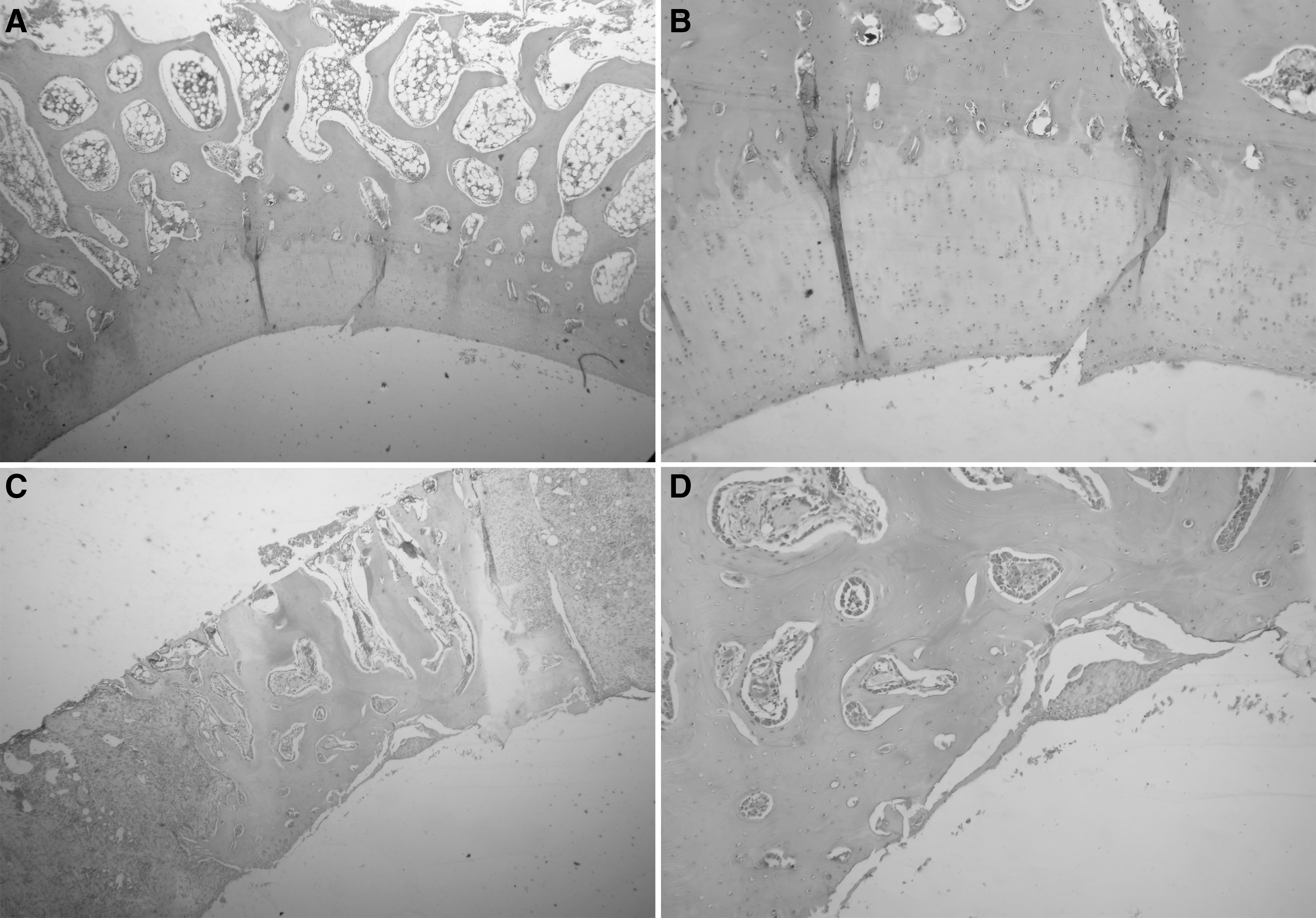
Three weeks after the surgery, histological analysis showed no blank spaces in the sample sections and all defects were filled with cartilage, bone, or other tissues (such as connective tissue) with different percentages (Fig. 4). The mean new cartilage formation was 11.19 ± 9.14 (SD)% in the experimental group, and 9.47 ± 7.28% in the control group, which had no statistically significant difference between both groups (p = 0.64). The newly formed cartilage in all samples was detected as hyaline type one. However, the new bone formation of the experimental group (47.40 ± 4.88%) was significantly higher than that of the control group (33.26 ± 15.34%) (p = 0.01), and, therefore, the other tissue formation was significantly higher in the control group (57.26 ± 17.69%) than in the experimental group (41.96 ± 8.56%) (p = 0.02). From the inflammation standpoint, it was 10 ± 14.14% in the experimental group, and 16 ± 20.65 percent in the control group, of which the difference between both groups was not statistically significant (p = 0.45). These findings are summarized in Fig. 5.
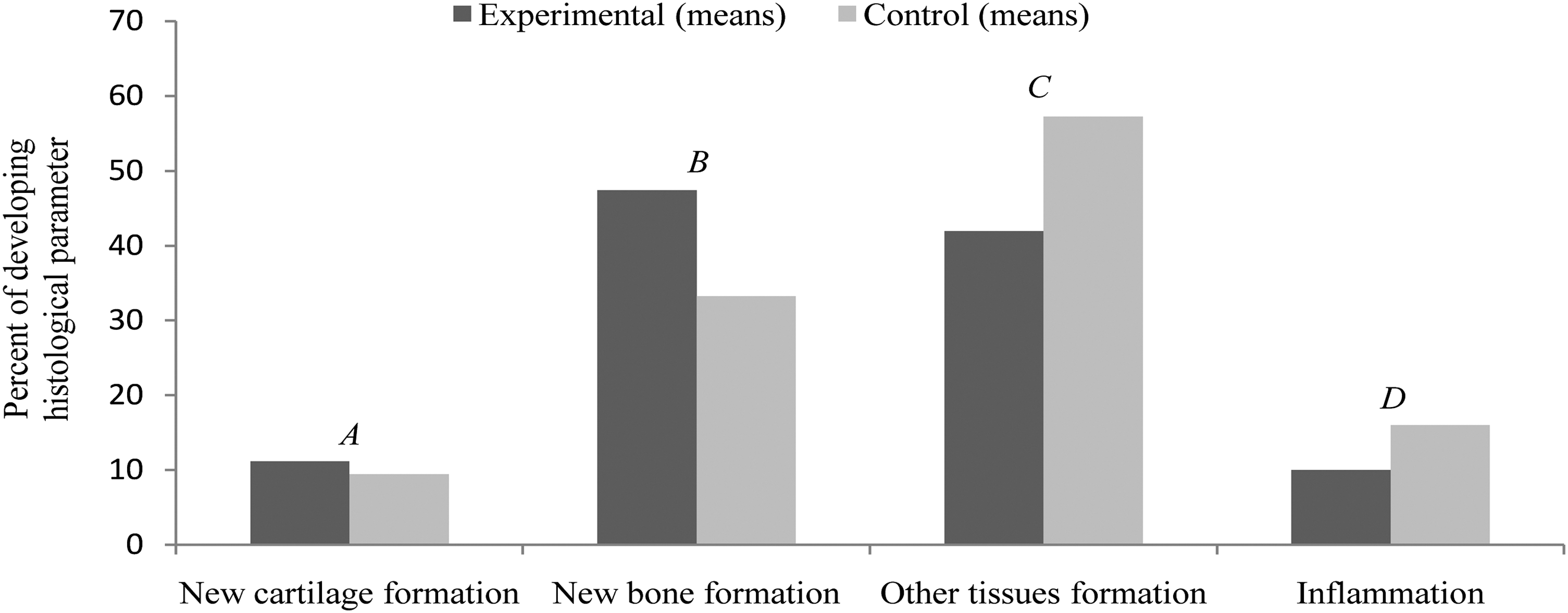
Comparative evaluation of developing various histological parameters between experimental and control groups during healing period. The difference between two groups in A and D was nonsignificant (p > 0.05), whereas a significant difference between two groups was shown in B and C (p < 0.05).
Discussion
In the current study, the combination effect of the application of BMSCs and photobiomodulation on the healing rate of full-thickness articular cartilage defects was compared with the application of BMSCs alone. A circular defect (diameter: 4 mm, depth: 3 mm) was artificially made on the articular surface of the patellar groove of the femur. Data revealed a mean cartilage thickness of 0.44 ± 0.08 mm in this region and, therefore, this limits the size and depth of the defects that can be made. The most common depth of experimental osteochondral defects reported in the literature is ∼3 mm, which means that >80% of the defect volume is located within the subchondral bone. 31 Partial-thickness defects in which damage does not extend into the subchondral bone, never repair spontaneously. This is because of the absence of a suitable source of cells for repair, and indicates the importance of the subchondral bone marrow as a pool for undifferentiated mesenchymal cells. However, the amount of BMSCs recruited is limited. 12,32 Shapiro et al. stated that chondrocytes from the residual adjacent cartilage did not participate in the healing of full-thickness articular cartilage defects. 33
According to the results of this study, using BMSCs along with laser therapy, was slightly more advantageous than the application of BMSCs alone, regarding the amount of new cartilage formation (p > 0.05). In all samples, the newly formed cartilage was detected as the hyaline type. This nonsignificant difference between two groups from the new cartilage formation standpoint may be the result of the nonoptimal cumulative dosage of the laser therapy; however, a more probable reason could be the short period of the study.
Nevertheless, significantly more new bone formation in the experimental group was recorded (p < 0.05), and a significantly more formation of other tissues in the control group (p < 0.05). This may indicate that considering the duration and conditions of this study, photobiomodulation led to considerable differentiation of BMSCs to osteoblasts. This result is in contrast to findings of a recent study by Fekrazad et al., who showed that there is no synergistic effect when combining LLLT and BMSCs on bone regeneration in rabbit calvarial defects during 3 weeks compared with the use of BMSCs alone. 34
The lower amount of inflammation seen in the experimental group may be related to the highly anti-inflammatory capacity of the infrared laser; 35,36 however, the difference between both groups was not statistically significant (p > 0.05).
Wakitani et al. first demonstrated the successful repair of a large, full-thickness defect by the transplantation of allograft chondrocytes isolated from the articular cartilage, embedded in collagen gel in the rabbit. 37 Favorable effects of collagen on facilitating cartilage repair were shown by a number of investigations. 32,38 –41 Kubo et al. showed that the use of collagen type I gel alone in cartilage defects causes an increase in cell proliferation by enhancing cell migration, but may not affect chondrocytic differentiation. 1 In the present study, commercial collagen type I matrix was used as a carrier for MSCs (because collagen type II matrix is not available because of its scarcity in tissue) transplantation. According to the findings of this study, in most cases, bone tissue rather than hyaline cartilage was formed. The formation of a bone repair tissue could be because of the use of collagen type I matrix as a microenvironment for transplantation of MSCs.
Hyaline articular cartilage naturally contains plenty of collagen type II, as well as hyaluronic acid (HA) macromolecules. The effect of both type II collagen scaffold and HA-synthetic hydrogel matrix has recently been emphasized in the MSC cartilage differentiation process. 11,42
Further, there could be two strategies with respect to the use of MSCs-mediated tissue regeneration. One route would be to use the undifferentiated cells, allowing them to undergo differentiation in an in vivo microenvironment. The disadvantage of this approach is that unwanted cell differentiation may occur at the transplantation site. In this regard, it has been advocated that phase-specific usage of growth factors that sustain the BMSCs-derived progenitor cells along the chondrogenic lineage are also required. 1 The alternative approach is to transplant fully differentiated cells. Such a strategy could guarantee the administration of the specifically differentiated cells into the repair site. 43 However, It is recently proposed that paracrine activities by MSCs might be more important than their differentiation in stimulating repair responses. 44
On the other hand, in vivo animal experiments on laser-induced regeneration of hyaline articular cartilage have shown promising results in the treatment of cartilage injuries. The main advantage of laser-induced regeneration is triggering of the intrinsic mechanisms of cartilage repair, which lead to filling the defects with hyaline-like tissue. 45 A Ga-Al-As diode laser (810 nm, 8.5 J/cm2) was used in this study, which is a type of infrared light irradiation. Morrone et al. showed the biostimulation effect of Ga-Al-As laser on cultured human chondrocytes without cell damage. 46
Kamali et al. indicated a significant enhancement of the stiffness of repairing tissue in osteochondral defects in rabbits, using a Ga-As (890 nm) laser irradiation with an energy density of 4.8 J/cm2. 47 Cressoni et al. showed that 830 nm Ga-Al-As laser irradiation at two different energy densities (5 and 15 J/cm2) on the epiphyseal cartilage of rats, led to an increase in thickness of the epiphyseal cartilage and in the number of chondrocytes. 48 Calatrava et al. also reported hyaline cartilage formation and high anti-inflammatory effect, following the use of an infrared laser (904 nm, 8 J/cm2) on experimental lesions of articular cartilage in rabbits. 35 Because the number of studies in this field is not large enough, and the outcomes of these studies are different in some cases, it seems that further research is needed. Because of the different nature of the cultured environment relative to the body's biologic environment, both experimental and clinical studies should be taken into consideration.
Conclusions
Regarding this research, although the combined use of BMSCs and photobiomodulation could promote the healing of osteochondral defects compared with the use of BMSCs alone, much of this improvement was the result of new bone formation rather than new cartilage formation. In order to better stimulate osteocartilaginous repair, the findings of this study suggest the recruitment of other appropriate scaffolds inducing stem cells toward chondrogenesis.
Footnotes
Acknowledgment
This work was supported by Laser Research Center in Medical Sciences, AJA University of Medical Sciences and Department of Regenerative Medicine Royan institute, Tehran, Iran. The authors thank Sima Bordbar (Royan Institute, Tehran, Iran), for her technical assistance.
Author Disclosure Statement
No competing financial interests exist.