
Abstract
Introduction
H
When there is a large defect or impaired cell supply, cell transplantation, which requires progenitor cell sources, is needed, and cell expansion must provide a sufficient number of cells. Autologous cells from the host can be used; however, there are limitations on donor sites and the extended time required for cell expansion. Allogeneic or xenogeneic cells are not limited in quantity or expansion time; however, an immunological response should be expected, because of the differing genetic content and matching human leukocyte antigens (HLAs). 1 –3
Another method is new tissue engineering. Three requisites can be used to regenerate tissue in this manner. First, a scaffolding is required to support cells seeded in vitro. The architecture of the scaffold should be effective for cell response and tissue formation. 4 Second is the use of growth factors (GF) delivered through the scaffold as a drug delivery system to encourage cells for engineering tissues. The third approach is the use of cell sources. Primary cells are used for tissue regeneration. This process focuses on three types of stem cells, depending upon on the cell origin and experimental manipulation: embryonic stem cells (ESC), adult stem cells derived from embryos and adult tissue, and induced pluripotent stem cells (iPSC) derived from adult somatic cells by genetic manipulation. ESC and iPSC are pluripotent stem cells that can develop into all type cells, whereas adult stem cells are multipotent cells that can differentiate to specific types of cells. 3,5,6
Stem cells are immature, unspecialized cells with self-renewal features that provide a cell source for tissue regeneration, or to replace damaged, missing, or impaired tissue or organs. 3,5 Differentiation is a critical cellular stage for these cells that allows them to provide specialized cells to form different tissues or organs. GFs are useful in tissue engineering because they increase stem cell differentiation to other cells. Other factors also affect this procedure, such as cell type, extracellular matrices, and soluble factors (GF). 3
Mesenchymal stem cells (MSCs) are mesenchymal stromal cells regardless of their tissue origin. They were originally found in bone marrow; however, they can be harvested from other adult tissue. 7 Pittenger et al. 8 revealed that these multipotent stem cells can differentiate into osteogenic, chondrogenic, and adipogenic cell lines. 3 MSCs can be isolated from many pre, peri- and postnatal tissues or organs. Prenatal sources consist of first and second trimester fetal blood, liver, and bone marrow and second trimester spleen, lung, metanephros, dermis, pancreas, and thymus. However, the umbilical cord, umbilical cord blood, amniotic fluid are the major perinatal MSC supply. Many postnatal organs can be sources of MSCs, including the skin, adipose tissue, blood vessels, and dental pulp. 3,9,10
There are several ways to promote proper cell expansion, such as the use of GFs in culture media, 11 and photobiomodulation (PBM). GFs stimulate and guide stem cells to proliferate and differentiate to proper cell numbers and types. Soon after the first laser was introduced, it was used in medical applications. 12 Photomedicine embraces the study and application of light (coherent or noncoherent) with respect to health and disease. 13 –15 It has been used in dermatology (UVA therapy), surgery, interventional radiology, optical diagnostics, cardiology, and oncology (photodynamic therapy). Photobiostimulation therapy promotes cell growth, regeneration, and healing of tissue by means of light sources such as light-emitting diodes (LEDs) and low-level lasers (LLL), or those that emit light in the visible red to near infrared (NIR) range and are known as PBM. 16
Several basic in vitro and in vivo studies have discussed the effects of PBM. This effect can be either inhibitory or stimulatory for pain control, as an anti-inflammatory, or for metabolic or immunological effects. 17 PBM affects the activity of endogenous enzyme photoaccepters for initiation of cell signaling pathways. It alters cell and tissue metabolism and cell proliferation. Cytochrome C oxidase enzyme has been identified as one of the major endogenous photoacceptors; however, the mechanism of the therapeutic laser remains unclear 16 with regard to its cellular and molecular effects. It appears to improve tissue engineering in keeping with stem cells.
Different coherent or noncoherent light sources are used for PBM. Although the diode laser is most frequently used for laser therapy, the He-Ne, Argon, Nd:YAG, and Er:YAG lasers have different wavelengths, power requirements, energy densities, and types of exposure, and have been successfully used for cell activation. 18 LEDs offer advantages such as low price, acceptable efficacy, high switching rate, and long life. 19,20 PBM has various biostimulatory effects on wound healing, 21 –24 extracellular matrix synthesis, 25 and promotion of cellular proliferation and differentiation in tissues such as bone, 26 –29 nerves, 30 and skin. 31 –36
Studies in this area are few and contradictory. The present study reviewed the articles to develop an understanding of the effect of PBM on MSCs to help design more accurate studies in the field of PBM.
Materials and Methods
PubMed and Science Direct electronic databases were searched for articles about the effect of PBM on MSCs. The keywords used were
The articles selected were characterized as in vitro or in vivo experimental studies and clinical trials that evaluated the effects of irradiation from LLLs and LEDs on MSCs. The initial selection included a review of articles; those that did not reflect the purpose were excluded. All articles that evaluated all lasers types except from other light sources such as Xenon flash lamps were included. Articles that assessed the phototherapy effect on other stem cell types, such as dental follicle stem cells, were excluded. This article only focuses on the photostimulatory effect on the MSCs. The abstracts of other studies were analyzed. At the end of the selection process, after reading the full texts, articles that matched inclusion criteria were reviewed. Figure 1 shows the process of studies selection.
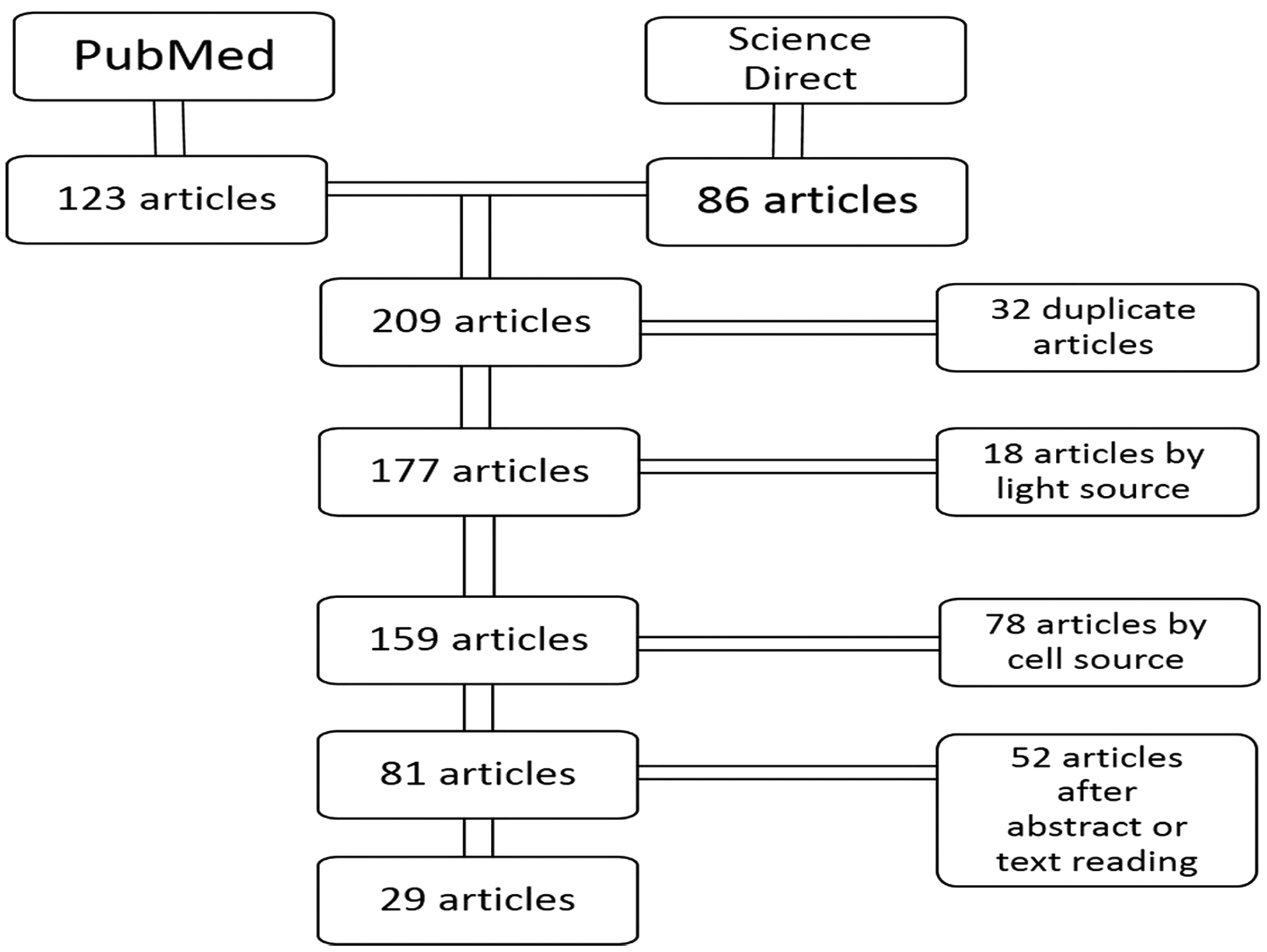
The process of studies inclusion/exclusion.
Results
The initial search uncovered 210 articles. After evaluation of the titles and abstracts, 32 articles were duplicated between databases, 18 and 78 articles were excluded because of unassociated light sources and cell types, respectively. Thirty articles were finally included. The data from the studies describe the parameters of the light sources. Diode lasers were the most commonly used laser type in the reviewed studies, which can be distinguished by specific laser such as GaAs, 37 GaAlAs, 29,38 –41 InGaAlP, 42,43 He-Ne, 44,45 and Nd:YAG. 35,46 Laser type was not available in two studies. 47,48 Laser wavelength in both of these was 400–405 nm.
Discussion
Advances in biomedical technology have increased applications for regenerative treatment. PBM of therapeutic light sources such as LEDs or LLLs are some of these technologies. Light energy allows cellular and molecular stimulation of target tissues. The result is regenerative treatment 20,39,49 –51 through the effect of chondroblast, neuroblast, and fibroblast proliferation or collagen synthesis and nerve regeneration.
PBM, by visible or NIR light, causes physical or chemical changes in cells. Although some mechanism of laser biostimulation was discovered, it is not exactly known. 47 Different mechanisms have been discussed, such as light absorption by mitochondrial enzymes with localized heating, and photon absorption by electron transport chain enzymes in the mitochondrial respiratory chain by flavins and cytochrome C. 38 Karu et al. 52 suggested that irradiation by LLL intensifies formation of a transmembrane electromechanical proton gradient in mitochondria. One possible mechanism is the absorption of laser energy by intracellular chromospheres, which is converted to metabolic energy. Karu et al. showed that He-Ne energy increased adenosine triphosphate (ATP) levels.
In this review, we found that the visible red light wavelengths were used more than the infrared wavelengths in experimental studies. Some studies compared the red and infrared wavelengths and obtained different results. In most studies, the visible spectrum (600–700 nm) was effective for cellular biostimulation. de Villiers et al. 49 found an increase in cellular viability and proliferation on human adipose-derived MSCs (hADSCs) using a diode laser (Table 1). Mvula et al. 50 reported that proliferation of ADSCs significantly increased after exposure to a diode laser at 636 nm wavelength (5 J/cm2).
MSCs, mesenchymal stem cells; LLLT, low-level laser therapy; hMSCs, human MSCs; rMSCs, rat MSCs; VEGF, vascular endothelial growth factor; BMSCs, bone marrow MSCs; LLLI, low-level laser irradiation; ADSCs, adipose-derived MSCs; hADSCs, human ADSCs; CSCs, cancer stem cells.
The diode laser was the most predominant light source used. While He-Ne, Er:YAG, and ND:YAG were used as other coherent light sources, LED sources were used as noncoherent light sources (Table 2). Leonida et al. 35 applied Nd:YAG laser to bone marrow MSCs and found that after 7 days of proliferation, the scaffold of the laser-treated group increased significantly over that of the control group. Peng et al. 51 used an LED (620 nm) to irradiate bone marrow MSCs (BMSCs) with and without osteogenic supplements. They found that in the group without osteogenic supplements and under red LED (0, 1, 2, 4 J/cm2) increased proliferation of cells could be expected. In the group with osteogenic supplements, alkaline phosphatase activity and differentiation increased and proliferation decreased with LED irradiation.
hADSCs, human adipose-derived mesenchymal stem cells; LLLT, low-level laser therapy; ERK, extracellular signal-regulated kinases; BMSCs, bone marrow mesenchymal stem cells.
The studies reviewed used laser doses of 0.7–9 J/cm2. The power used for visible light was 30–110 mW and that used for infrared light was 50–800 mW. One study investigated effect of the Ga-Al-As laser (810 nm) with an energy density of 3 and 6 J/cm2 for differentiation of BMSCs to neurons and with an energy density of 2 and 4 J/cm2 for differentiation to osteoblasts. 39 PBM increased proliferation in all doses except for 6 J/cm2. Cellular differentiation increased at all doses. Soleimani et al. 39 suggested that the effect of low-level laser therapy (LLLT) on proliferation and differentiation is dose dependent.
Other parameters for irradiation, such as the effect of light source and period of irradiation on MSCs, were different in different studies. The minimum time point used was immediately after irradiation and the maximum was 4 weeks after laser treatment. MSCs were often derived from bone marrow, adipose tissue, dental pulp, and periodontal ligaments. In most studies, proliferation and differentiation were assessed, but the evaluation techniques differed. Most studies showed a positive effect for LEDs and lasers on cell proliferation and differentiation.
Farfara et al. 47 evaluated the effect of LLLT on BMSCs in mice with Alzheimer's disease. They concluded that the application of lasers improved maturation of MSCs and increased phagositosis of Aβ protein by elevating the activation state. de Oliveira et al. 38 used a Ga-Al-As laser on human MSCs (hMSCs) and rat MSCs (rMSCs) in a study of nutritional deficiency, to examine the effect of LLLT on adhesion, proliferation, gene expression of vascular endothelial growth factor (VEGF), and type 2 receptor of VEGF (VEGFR2). They reported that low nutritional support significantly decreased proliferation. At lower doses (0 and 7 J/cm2) proliferation increased and at higher doses (3 and 9 J/cm2) adhesion increased. They suggested that different specimens and laser doses could cause different results. Kim et al. 45 showed that He-Ne is an effective biostimulator of wound healing using adipose-derived mesenchymal stem cells (ASCs) to stimulate secretion of GF in the wound bed.
The main effect of photobiostimulation therapy in clinical or in vitro activity is proliferation. This effect activates the mitochondrial respiratory chain and cell signaling by laser irradiation. 53 Red/NIR LED irradiation leads to heating at the molecular level by ATP production. 54,55 It appears that laser phototherapy inhibits apoptosis, which increases survival of ASCs and produces GFs in the wound bed at the functionally appropriate dose and wavelength. 23,56,57 It is possible for PBM to increase cell response by elevating the mitochondrial membrane potential and ATP and cyclic adenosine monophosphate (cAMP) levels. 56
Two studies on animal brain tissue found that ATP content increased in response to temperature elevation by red/NIR LED. PBM also increased differentiation of stem cells. 54,55 A few studies investigated cell differentiation caused by laser irradiation. Almost all showed a positive effect for PBM on differentiation; however, some found no significant difference between the irradiated and control groups. One study found that at 647 nm, red light transformed MSCs to osteoblasts; 58 however, Kim et al. 45 found that differentiation of ASCs was not noticeably different between the laser-treated (632 nm) and control groups. Stein et al. 59 found that LLLT (632 nm) promotes proliferation and differentiation of human osteoblast cells. Leonida et al. 35 evaluated the effect of an Nd:YAG laser (1064 nm) on MSCs. After 7 days, significant proliferation was observed in the laser-treated scaffold and, after 14 days, an exponential increase was observed in the laser-irradiated group.
Visible NIR wavelengths were commonly used in the studies. The most effective result was for visible wavelengths (600–700 nm), but some articles reported cell proliferation at 780 nm 60 and 860 nm. 61 Anwer 46 suggested that mitochondrial activity increased at lower wavelengths. There was a large range of wavelengths used that produced a variety of results. It appears that biostimulation is dependent upon factors such as output power, 62 energy density, 63,64 and cell type. 65 Hawkins, 33 Mvula, 50 and Anwer 46 found that PBM increased cell viability and proliferation. Most in vitro studies indicated that different cell cultures do not respond in the same way to lasers. 66
The positive effect of PBM on proliferation of MSCs in some studies suggests that lasers alone do not cause significant cell differentiation. One study showed that noncoherent red LED of BMSC specimens with osteogenic supplements increased differentiation, but proliferation increased in the group without osteogenic supplements. 27 One theory is that there is a reciprocal relationship between proliferation and differentiation in MSCs. 66 This theory also suggests that the induction of osteogenic differentiation by red LED occurs during proliferation. It theorizes that light alone cannot activate cell signaling pathway and could be an adjunct tool in osteodifferentiation. 27 It appears that more study is required, especially for in vivo and clinical trials.
Conclusions
A review of articles has shown that PBM increases proliferation of MSCs. These results depend upon factors such as energy density, power output, frequency of radiation, type of light source, and type of cell or medium culture. It appears that standardization of parameters in PBM by experimentation is required to obtain the favorable results that allow for more accurate comparisons.
This review found that doses of 0.7–4 J/cm2 and visible wavelengths from 600 to 700 nm were the most appropriate for PBM to increase cell proliferation. Although contrary results have been mentioned in studies, most agreed that PBM had positive effects of biostimulation of bone tissue and increasing cell proliferation and differentiation and was a helpful tool in regenerative treatments.
Footnotes
Author Disclosure Statement
No competing financial interests exist.