
Abstract

To the Editor:
D
DD is characterized by symmetrical hyperkeratotic papules affecting seborrheic areas and extremities. Mild forms, usually located on the trunk, neck, and folds are the most common, and are often undiagnosed; skin signs may be associated with itch and a distinct odor, which may affect social life. 2 The existence of unsightly lesions could lead to discomfort and be a social handicap. Treatments for DD include topical retinoids, calcipotriene, and 5-fluorouracil; dermabrasion; photodynamic therapy; and oral retinoids, which need to be given for a long period of time. 1 Ablative lasers such as CO2 and Erbium:YAG lasers have also been used to treat these conditions, with variable results and side effects. 3
In 2009, Schmitt et al. described a successful treatment of two patients affected by DD using a 595 nm pulse dye laser (PDL). To their knowledge, the mechanism of action was unclear; however, no other subsequent studies have confirmed this finding. 4
We herein present the results after dye laser treatment in a case series of nine patients with DD who failed traditional treatment (e.g., keratolytics, topical corticosteroids, antibiotics, retinoids). Patients' characteristics are described in Table 1. They all signed informed consent for treatment and photographs.
HSV, herpes simplex virus.
All patients underwent treatment with a 595 nm PDL using purpuric settings (pulse duration 0.5 ms, spot size 10–12 mm, fluence 6.5–7 J/cm2). Treatments were repeated every 8 weeks (total of two treatments per patient). Postprocedure care instructions included cleansing with saline (once a day) and fusidic acid ointment (one or two times a day). In two cases, herpes simplex virus (HSV) flares were reported as side effects.
The time to achieve resolution ranged from 2 to 4 weeks after the second treatment.
The results are reported in Table 1, established by the physician with a clinical evaluation 3 months after the last treatment, considering the response excellent (Figs. 1 and 2), good, moderate, or poor.

Before and after treatment with excellent result.
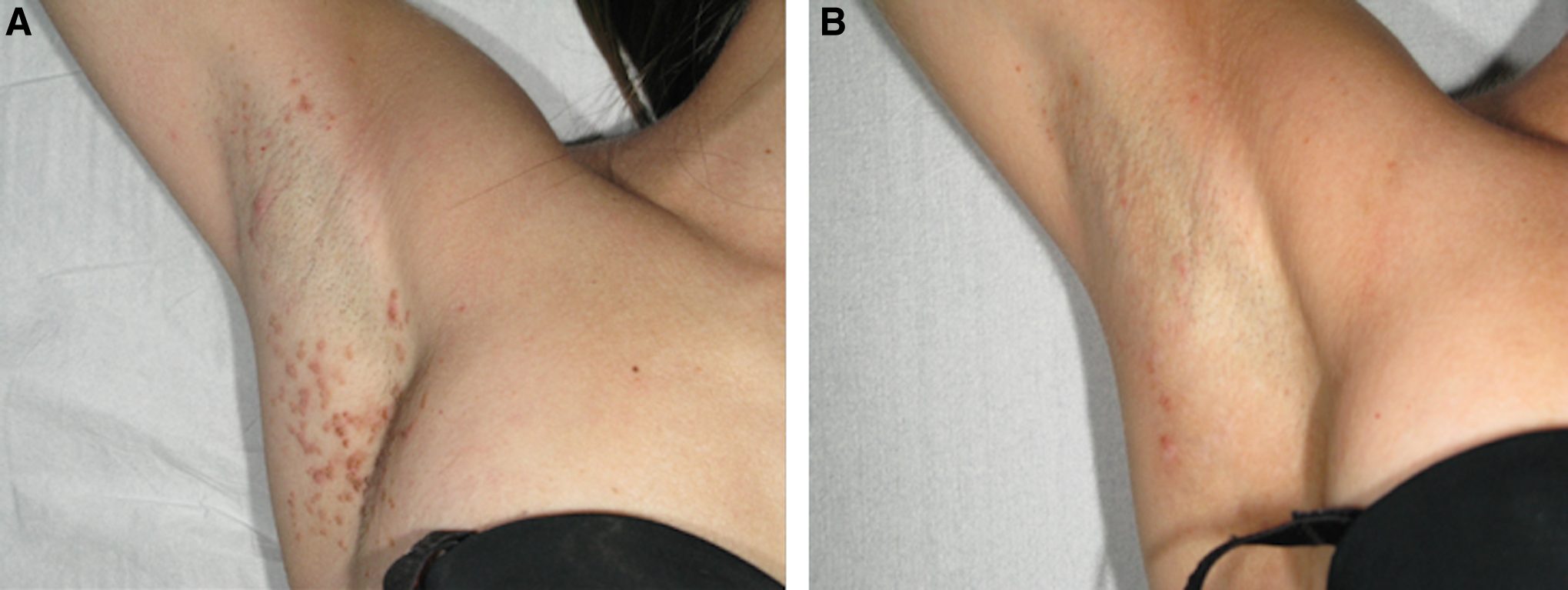
Before and after treatment with excellent result.
Only two patients relapsed after 3 months of follow up, two patients presented a few persistent lesions, and other four patients showed good and long-lasting improvement without any new lesions appearing.
The definitive mechanism for improvement in DD treated with PDL has not yet been clarified; but we propose herein a hypothesis that may be a starting point for further research.
Laser therapy is generally based on the concept of selective photothermolysis. PDL is a 595 nm laser used for the therapy of vascular lesions because of their high absorbion by oxyhemoglobin, although it has been used for many inflammatory diseases (i.e., cutaneous lupus erythematosus, psoriasis, eczema). It elicits mild capillary damage and edema of endothelial cells in dermal connective tissue. This damage may produce and release cytokines and growth factors, eventually leading to the stimulation of new collagen replenishment. 5
Omi et al. demonstrated an increased of inflammatory cells (neutrophils, monocytes, mast cells, lymphocytes) after 3 h even to 5 weeks after irradiation. Therefore, taking these data all together, we can state that PDL may stimulate cutaneous immunological response. 6
In conclusion, we speculate that the efficacy of PDL in an inflammatory disease, such as DD, could be the result of both the vascular components of the lesions, and of its immunomodulatory properties.
As the treatment is moderately painful, nonablative, and with few potential complications, PDL can be considered a safe and effective alternative to other therapies for DD, despite the cost of the device. In order to minimize side effects, antiviral and topical antibiotic may be added. Further studies with wider casuistics are obviously required to better understand the exact mechanism of PDL action in this and other inflammatory diseases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.