
Abstract
Introduction
Concussion and mild traumatic brain injury
C
Concussion and mTBI have been shown to reduce blood flow to the brain. 3,4
A correlation has been shown in studies between blood flow and brain function; impeded blood flow reduces the brain's ability to operate. 5 Estimates are that from 10% to 30% of concussion patients experience prolonged symptoms, described as postconcussion syndrome (PCS). Some PCS patients have persistent hypoperfusion in concussed areas of the brain as revealed by single-photon emission computed tomography. 6 Such hypoperfusion may impede neuronal function by starving cells of glucose and oxygen, thus impacting mitochondrial function and cell respiration.
TBI diagnosis and quantitative electroencephalography
The diagnosis of concussion is one of the main challenges faced by neurologists. Quantitative electroencephalography (qEEG) has been shown to be a viable tool for the diagnosis of concussion/mTBI based on several measurable factors. These measures include P300 brain speed, reaction time, and amplitude. Amplitude is a measure of the voltage levels of neural cells. Typical amplitude for healthy functioning cells as measured from the scalp can range from 10 to 100 microvolts (μV). P300 is an event-related potential (ERP) component of EEG elicited in the process of decision making. The signal is often used as a metric of cognitive function in decision-making processes. Reaction time is an overall measure of speed of brain response to stimuli and reflects the response efficiency of the brain at a given time. Improvement in these measures over time or treatment may indicate brain state changes, which favor repair of concussive damage. 7 Restoration of blood flow may improve delivery of glucose and oxygen needed to create excitatory postsynaptic potential triggered by stimulus response activity such as is posed by EEG event-related tests. In addition, direct photostimulation of mitochondria through the cytochrome C oxidase pathway may elicit higher ERP response.
TBI treatment options
Based on mTBI pathophysiology, the treatment goal is to restore blood flow and normal neuronal activity. Currently, the only treatments available for concussion/mTBI are rest, cognitive therapy, and, in some cases, hyperbaric oxygen therapy. Rest is simply allowing the body to run its course in the healing of the brain. Cognitive therapy has been met with mixed and limited results in chronic PCS. 8 Hyperbaric chambers have shown promise by delivering enhanced oxygen levels to the brain tissue. Although improved survival has been demonstrated with hyperbaric oxygen therapy (HBOT), improvement in PCS has not been shown. 9 Another emerging treatment option is near infrared (NIR) light therapy, which has been shown to stimulate blood flow in damaged peripheral tissue. 10 Applying this treatment to improve neural tissue blood flow is a natural inference from this observed mechanism of action.
Recent studies on TBI patients show that NIR light therapy may improve postconcussion symptoms. Results of in vitro studies, combined with human clinical studies, show improved blood flow and possible neurogenesis resulting from treatment.
11,12
Several studies demonstrate that NIR light wavelengths penetrate to significant depths through cranial tissues. One study showed the half-time of exponential decay of 800 nm NIR light corresponds to photon migration over a distance of 4 cm.
13
In another study of optical path length measurements on adult and newborn infant heads using phase-resolved optical spectroscopy, the investigators measured mean path lengths of NIR light of 26.48 and 19.96 cm, respectively.
14
Recent human case studies suggest that NIR light can help in the healing of acute concussions and chronic traumatic brain injuries.
15,16
Some subjects report antianxiety effects after treatment, lasting up to 2 days [Victoria Campbell, Campbell Consulting and Counseling (
Study Objectives
The objective of this study is to determine whether NIR light has an acute and generalized effect on brain state change as measured by P300 brain speed, amplitude, and reaction time. Specifically, the study looks for any acute brain state changes induced in healthy volunteers by a single NIR light treatment. Results may suggest mechanisms of action for NIR light in treatment of mTBI. Secondary objectives are to measure safety and any adverse events associated with NIR light treatment.
Materials and Methods
This study was performed under the Western Institutional Review Board (IRB), Olympia Washington, OHRP/FDA Parent Organization number: IORG0000432 IRB registration number: IRB00000533.
Thirty-one healthy volunteers between the ages of 16 and 65 years were recruited to participate. As pediatric sports-related concussion is a rising issue, inclusion of pediatric subjects was determined to be of interest in this study. Seven subjects were of age 18 years or younger. Patient consent forms were signed by all participants and by parent/guardian for subjects under 18 years. Exclusion criteria included recent diagnosis of mTBI or known cognitive impairments related to mTBI or dementia.
Subjects signed informed consents and filled out a medical history before the test. They then underwent a qEEG measurement using a 19-lead EEG cap. Data were captured on an EEG program developed by WAVi Brain Health Solutions, Boulder, Colorado. 17 Subjects were measured on event-related response tests, in which they heard a series of frequent low tones and rare high tones. They were instructed to click a mouse upon hearing the rare high tone. Each subject was presented with 60 rare tone reaction opportunities.
Subjects were then given a 20-min NIR light treatment using an LED treatment device (LumiWave Infrared Light Therapy Device, BioCare Systems, Inc., Parker, CO). 18 The device is composed of 784 NIR GaAIAs LEDs covering 360 cm2 on the head in a cap configuration of four 1 × 4 NIR light pod sets, each containing 49 LEDs. The configured device covered the occipital, left temporal, and right temporal lobes above the ear line, as well as the frontal and parietal lobes. The fluence rate was 1 J/cm2·min for a power density of 16.67 mW/cm2. Peak spectral wavelength at steady-state temperature (42.2°C) was 903 nm. The device delivered a total dose of 20 J/cm2 to the surface of the skull. The device is FDA cleared for treatment of musculoskeletal pain. Application of the device to the cranium represents an off-label nonsignificant risk under the study IRB. Subjects were then given a second qEEG test. Two to four months later, 18 subjects returned for a second round of qEEG measurements, this time with a 20-min rest period in place of the NIR light treatment. This set of EEG measurements served as a control arm.
One-way ANOVA was performed on change from baseline for treatment versus control groups for each of the EEG measures.
Results
There were 28 evaluable subjects in the treatment group and 18 evaluable subjects in the control group.
Reaction time
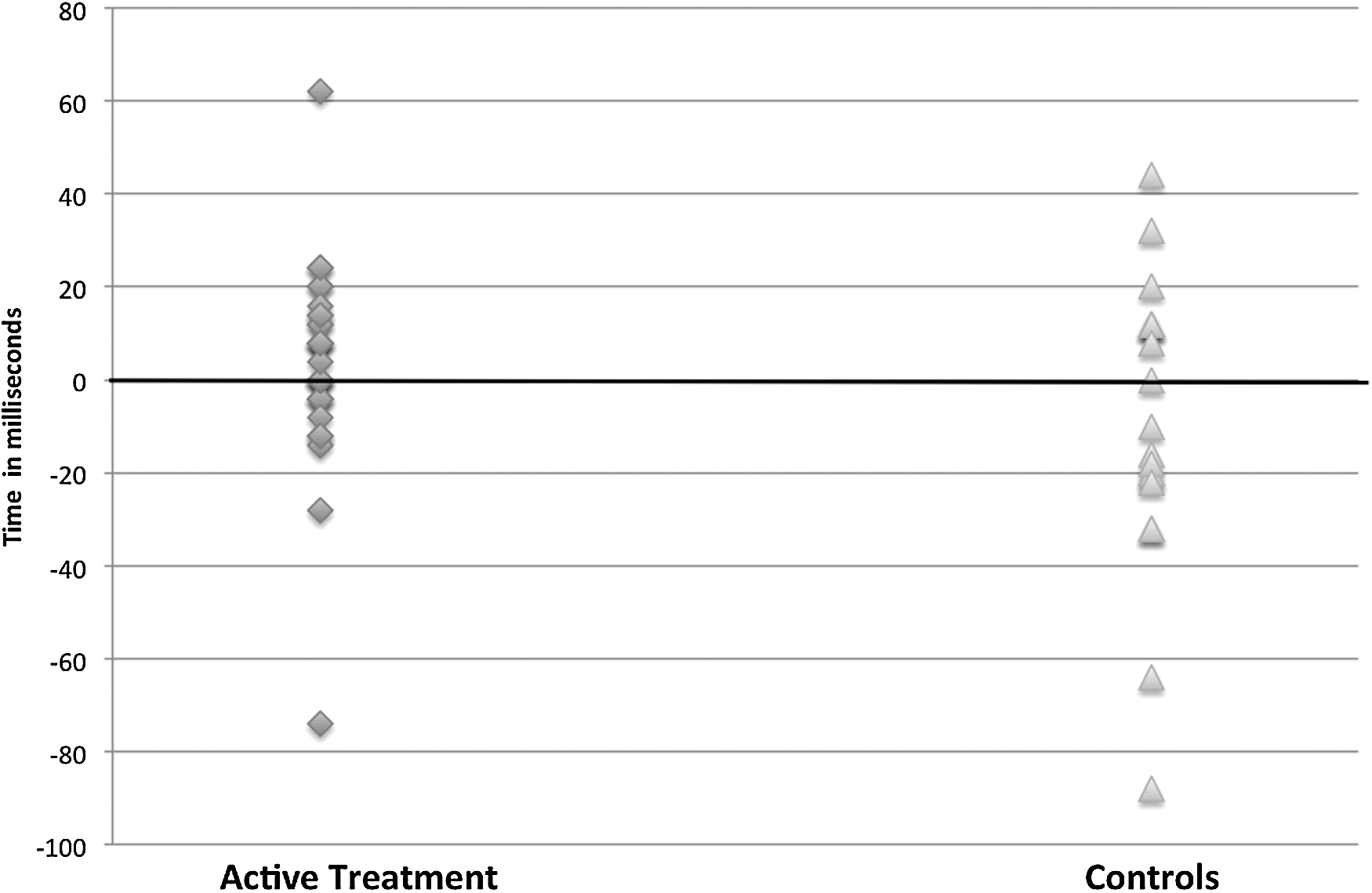
There was a statistically significant difference in mean change in reaction time between treated and control groups. A negative number indicates a faster reaction time. Mean change in the treated group was −10.62 msec (−2.31%) compared with +10.11 msec (+3.53%) for controls (p = 0.035). Data showed a faster reaction time for post-NIR light treatment subjects than for controls (Fig. 1).

Change in reaction time from before versus after treatment was calculated. The majority of subjects showed reduced reaction time after treatment, representing an improvement in speed of response to auditory stimulus. Change in reaction time after a 20-min rest period skewed toward an even result to slightly slower times.
Amplitude
Amplitude is a measure of voltage, expressed in μV, emitted by neural tissue. In this study, amplitude increased an average of 0.81 μV in treatment subjects and 0.22 μV in controls. This difference did not reach significance. However, subanalysis of 13 treated subjects and 8 controls, all displaying initially low amplitude (<10 μV), showed a positive treatment effect. The average initial voltage of the treated subjects was 6.56 μV. Eleven of these 13 subjects showed an increase in amplitude after NIR light treatment. The average voltage post-NIR light was 8.71 μV, representing a mean improvement of 2.15 μV, or 33%. The control group showed a mean 0.0 μV change from prerest to postrest period. Although the sample size was small, the data show a trend toward improvement of amplitude post-treatment, approaching statistical significance (p = 0.055) (Fig. 2).
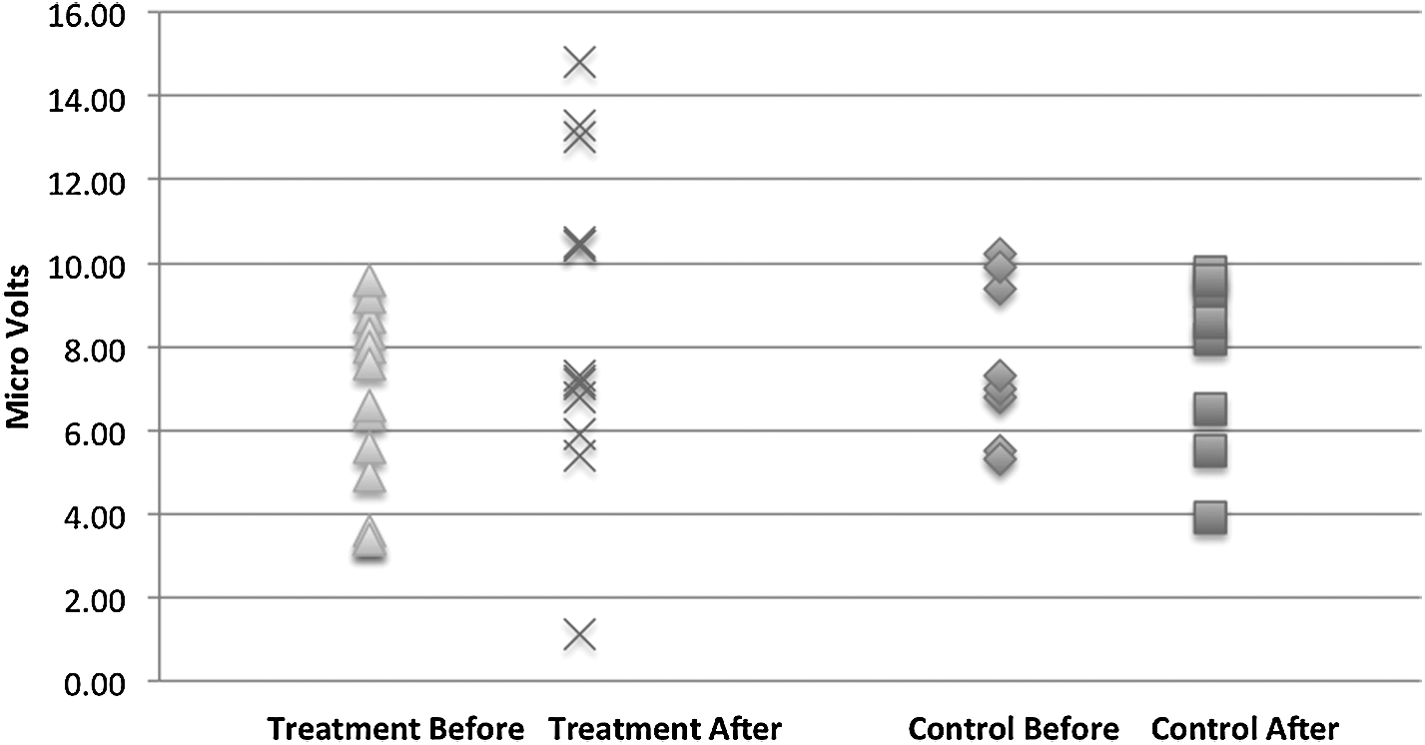
Change in amplitude measures voltage output of neural tissues, which can be impaired by trauma. The sample as a whole did not show significant changes in amplitude in response to either treatment or rest. However, a subset of subjects who displayed initially low amplitude did respond to treatment with increased voltage. The same subjects when tested before and after a rest period did not show a change.
P300
No statistically significant differences were found in P300 from pre- to post-NIR light treatment compared with controls. Mean change in P300 for the treatment group was +3.36 msec (+0.89%) compared with −8.95 msec (−2.62%) for the control group (p = 0.09). The standard deviations for the treatment group versus control group scores were 21.99 and 31.06, respectively. The data skewed slightly toward slower P300 post-NIR light treatment compared with controls (Fig. 3).
Changes in P300 auditory response latency did not change significantly from baseline after treatment. Changes skewed slightly toward slower latencies. Under the control test, change from baseline also did not skew significantly toward either faster or slower latencies. The variation in change responses was greater in the control conditions than in the treatment intervention.
Within-group analysis
Analysis was made of P300 and reaction times for self-paired, within-group changes (treatment group before vs. after and control group before vs. after). The P300 measures did not show a statistically significant difference in speed changes within groups. Mean P300 score for pretreatment was 374.21 msec. Post-treatment P300 score was 377.57 msec, with an average difference of +3.36 msec from pre- to post-treatment (p = 0.49). Mean prerest P300 score for the control group was 356.00 msec, whereas the postrest mean score was 345.89 msec, with a mean difference of −10.11 msec (p = 0.44).
Mean pretreatment reaction time was 380.52 msec, whereas post-treatment mean was 369.90 msec with a mean difference of −10.62 msec (p = 0.51). Mean prerest reaction time for the control group was 327.61 msec, whereas the postrest mean was 340.83 msec, with a mean difference of +13.22 msec (p = 0.55).
There were no statistically significant differences found in within-group test results, pre- versus post-treatment, or pre- and postrest period with regard to P300 or teaction time. Change in reaction time did significantly differ between treated and control groups, with the treated group showing statistically significantly faster reaction times after treatment than the control group. Subject age did not have a statistically significant impact on changes in measures.
Control group analysis, taken together with or separately from the treatment group, shows no learning effect on P300 or teaction time.
Safety
There were no adverse events registered across the 31 enrolled subjects in the treatment group, nor in the 18 control group subjects.
Discussion
A concussion initiates a complex cascade of metabolic events, leading to perturbation of delicate neuronal homeostatic balances. Starting from neurotoxicity, energetic metabolism disturbance caused by the initial mitochondrial dysfunction seems to be the main biochemical explanation for most postconcussive signs and symptoms. 19 An immediate consequence of brain trauma is abrupt, indiscriminant release of neurotransmitters and unchecked ionic fluxes, leading to increased potassium and calcium pump activity to restore membrane potential. 20 –22 This results in significant increase of glucose demand to manage the pump activity. At the same time, cerebral blood flow is significantly decreased in the damaged regions for up to 10 days in the acute concussion setting. This exacerbates the brain's ability to mobilize glucose and clear ions, leading to a period of depressed metabolism that limits mitochondrial function and causes a buildup of calcium, which, in turn, hastens cell death. 23 PCS describes a variety of chronic symptoms resulting from an initial mTBI event. Symptoms are driven by underlying anatomic, neurometabolic, and physiological sequelae. Diagnosis and treatment approaches focused on these underlying conditions will logically show the most promise for efficacy.
NIR light therapy
Cerebral blood flow is linked to neural activity. 24 NIR light has been shown to stimulate release of nitric oxide, an endogenous potent vasodilator resulting in increased blood flow. 25 This has been shown to occur in the absence of thermal effects, using lasers to deliver the NIR light. 26 Additional mechanisms appear to be at work. Karu showed that NIR light is absorbed by components of the cell respiratory chain, causing activation leading to changes in redox status of both the mitochondria and the cytoplasm. Radiation in the NIR range was shown to initiate a response in the cell membrane through effects on the calcium channels. This in turn has an effect on membrane permeability and ion transport. 27 This suggests a possible effect of NIR light on concussed neural tissue. Indeed, Ca++ waves are prominent in synaptic and extracellular processes that influence coherent neuronal firings measured by EEG. 28 The hypothesis of this study was that NIR light would affect EEG P300 readings of calcium channel-driven neuronal activity and related cell voltage, and would reduce reaction time through these and other mechanisms. Further, Lapchak and De Taboada demonstrated that transcranial NIR light treatment increases ATP content through cytochrome C photo acceptors in mitochondria in a rabbit model. This, in turn, can energize brain cell electrical activity. 29
Effects of NIR light on P300 and reaction time
Although the data from this study failed to show a meaningful effect on P300, the data do suggest that NIR light has an effect on reaction time that does not appear to be related to P300 ERPs in this acute setting with healthy volunteers. However, the increase in amplitude in treated subjects compared with that in controls suggests a possible mechanism for the reaction time effect. Direct activation of the cell respiratory chain, downstream from the typical mitochondrial initiation may be involved. 30 Additional investigation is warranted to determine whether longer term NIR light treatment of diagnosed concussion or chronic TBI will result in improved P300 activity.
Investigators have noted that light therapy has the most pronounced effect on poorly functioning cells and little, if any, effect on normally functioning cells. 31 For example, light therapy appears to stimulate healing of trophic skin ulcers, whereas the effect on normally healing wounds is insignificant. 27 The implication is that normally functioning cells are not accelerated in their activity by NIR light but are rather left in their normal functioning state. However, if a cell is operating suboptimally, then NIR light stimulates it to revert to an optimal functional state. This is thought to be accomplished through the already cited stimulation of cell respiratory chains, leading ultimately to altering Ca++ flux that, in turn, affects the levels of cyclic nucleotides, which modulates DNA and RNA syntheses and resulting cell proliferation. In this study, subjects displaying normal-range amplitudes showed little effect from a single NIR light treatment. However, subjects displaying subnormal amplitudes showed fairly large change in amplitude after treatment. Acute activation of neuronal energetic metabolism in suboptimally functioning cells through biostimulation of the cell respiratory chain, coupled with increased blood flow bringing additional glucose and oxygen, may explain this finding.
In this study, the NIR light treatment appeared to be safe, with no adverse events reported. The low energy of NIR light causes electrons to vibrate or “warp” in their orbits but does not provide sufficient energy to raise it to a higher energy state necessary to cause a molecular bond break. 25,32 Thus it is believed that the potential for photochemically induced damage is low.
Conclusions
NIR light shows promise as a potential treatment modality for mTBI. Elucidating the underlying mechanisms of action of NIR light on neural tissue is an important step in optimizing treatment regimens. This study demonstrated that reaction times improved with NIR light treatment. A possible related mechanism might be NIR light stimulation of neuronal energy metabolism, at least for tissues functioning suboptimally. Amplitude improvements in subjects displaying initially low-voltage readings suggest that cell respiratory activation may be stimulated by NIR light, resulting in an electrical brain state change favoring reaction time improvement. Evidence points to NIR light having no particular effect on already healthy cells and tissues. This would align with a treatment for symptomatic mTBI. However, neuronal coherence, as measured by P300, was not revealed as a component to improved brain activity in an acute setting. Beyond uncovering the mechanisms of NIR light effect vis-à-vis reaction time on healthy tissue in an acute setting, the next step suggested is to measure longer term NIR light treatment of diagnosed mTBI patients to determine whether the model of stimulating unhealthy tissue to return to normal functionality holds true in a clinical setting.
Footnotes
Acknowledgments
The authors thank WAVi Co. and Dr. David Oakley, PhD, for provision of qEEG units. The authors also thank BioCare Systems, Inc. for provision of NIR light therapy devices.
Author Disclosure Statement
F.G. and M.W. report that no competing financial interests exist. J.W. reports an employment arrangement with BioCare Systems, Inc., outside the submitted work. In addition, the company has materially related patents pending.