
Abstract
Introduction
I
Recently, limited studies have demonstrated the effects of Er:YAG laser irradiations on both enamel demineralization and the bond strength of brackets. 13,14 However, no study has been published about an effective bonding procedure that both prevents demineralization around brackets and provides clinically acceptable bond strength through different combinations of Er:YAG laser irradiation with dissimilar adhesive systems. This study had two purposes. The first objective was to investigate the effects of different combinations of Er:YAG laser irradiation and adhesive systems on enamel demineralization around orthodontic brackets. The second objective was to evaluate the impact of these different bonding procedures on the shear bond strengths (SBS) of the brackets. For the purposes of this study, the first null hypothesis assumed that different combinations of Er:YAG laser parameters and adhesive systems had no impact on prevention of enamel demineralization. The second one was that these different bonding procedures did not cause differences in the SBS of the brackets.
Materials and Methods
The ethics committee of Suleyman Demirel University (05.12.2012-125) approved this in vitro study. A total of 162 noncarious maxillary and mandibular premolar teeth extracted for orthodontic purposes were used. The teeth were examined under a stereomicroscope, and teeth with hypoplastic areas, cracks, and irregularities of enamel structure were excluded from the study. A total of 108 teeth were used for SBS testing, and 54 teeth were used for demineralization evaluation in this study. All teeth were stored in 0.1% sodium azide solution at room temperature, and the solution was changed weekly to prevent bacterial growth. For each evaluation, teeth were randomly allocated into three groups; control (no laser etching), 1 and 2 W laser groups according to the etching procedure. Then, these groups were divided into three subgroups based on the application of different adhesive systems (etch and rinse, all-in-one self-etching, two step self-etching). Consequently, nine study groups were adopted, as follows: G1: Acid etching + Transbond XT Primer (Etch&rinse adhesive) G2: Er:YAG laser (100 mJ, 10 Hz) etching + Transbond XT Primer G3: Er:YAG laser (200 mJ, 10 Hz) etching + Transbond XT Primer G4: Transbond Plus SEP (all-in-one self-etching adhesive) G5: Er:YAG laser (100 mJ, 10 Hz) etching + Transbond Plus SEP G6: Er:YAG laser (200 mJ, 10 Hz) etching + Transbond Plus SEP G7: Clearfil Protect Bond (CPB) (two-step self-etching adhesive) G8: Er:YAG laser (100 mJ, 10 Hz) etching + CPB G9: Er:YAG laser (200 mJ, 10 Hz) etching + CPB
All stages of the study were performed by the same researcher (S.C.).
Preparation of samples
Power analysis (G* Power, version 3.0.10, Kiel, Germany) indicated that for each group, 12 teeth/surfaces would give >80% power at an α = 0.05 level of significance. For the first part of this study, the buccal and lingual surfaces of 54 teeth were cleaned with fluoride-free pumice with a rubber cup, then washed and dried. All surfaces were covered with nail varnish except for two windows (∼4 × 4 mm) left on the middle third of the buccal and lingual surfaces. Then, all samples were stored in deionized water until the bonding of brackets.
For the SBS test, the roots of 108 premolar teeth were individually embedded vertically into self-curing acrylic at a 1–2 mm distance from the cement–enamel junction in such a way that the long axes of the teeth were perpendicular to the resin block. Then, the samples were stored in distilled water, and the buccal enamel surfaces of the teeth were pumiced, washed, and dried before the bonding procedures.
Etching procedures
The enamel surfaces of the teeth in G1 were etched with 37% phosphoric acid (Scotchbond, 3M ESPE, USA) for 15 sec, then rinsed for 15 sec, and dried thoroughly in moisture- and oil-free air to obtain an opaque white appearance. In the laser groups, the enamel surfaces were etched with a 2940 nm Er:YAG laser (LightWalker AT, Fotona, Ljubljana-Slovenia) for 15 sec. The laser parameters were as follows: energy per pulse of 100 or 200 mJ, pulse repetition rate of 10 Hz, average output power of 1 or 2 W, pulse duration of 100 μs (medium-short pulse mode), and energy density of 15.72 or 31.44 J/cm2. The levels for water and air were 60% and 40%, respectively. The laser irradiation was directed manually using a noncontact hand piece (H02-C) and delivered with a sweeping motion perpendicular to the enamel surface. The diameter of the tip was 0.9 mm.
Then, the teeth were air dried until a characteristic frosty opaque etched area was observed, similar to the acid etched group. After the etching procedure, the brackets were bonded according to the following bonding procedures.
Bonding procedures
Etch&rinse (Transbond XT Primer), all-in-one self-etching adhesive (Transbond Plus SEP) and two step self-etching adhesive (CPB) were used in this study. Detailed information about bonding materials were given in Table 1. A total of 216 0.018 slot size premolar brackets (Gemini, 3M Unitek, USA) were bonded with the light-cured composite (Transbond XT paste, 3M Unitek, USA), and any excess composite was removed carefully using an explorer. Subsequently, the resin was polymerized for 10 sec from each of the mesial and distal sides. After bonding, all samples to be evaluated for demineralization and SBS were kept in distilled water for 24 h at room temperature.
HEMA-MMA, Hydroxyethyl methacrylate-methyl methacrylate (HEMA-MMA) copolymers; MDPB, methacryloyloxydodecylpyridinium bromide; GMA, glycidyl methacrylate; UDMA, urethane dimethacrylate; TEGDMA, triethylene glycol dimethacrylate.
pH cycling
After the bonding procedure, samples were exposed to pH cycling to obtain caries-like lesions. The teeth were immersed in demineralization and remineralization solutions at 37°C for 6 and 17 h per day, respectively. This cycling began with a demineralization solution (pH = 4.5) consisting of 2.2 mmol/L CaCl2, 2.2 mmol/L NaH2PO4, and 0.05 mol/L acetic acid. Then, the samples were washed with deionized water and immersed in the remineralization solution (pH = 7.0), consisting of 0.15 mol/L potassium chloride, 1.5 mmol/L calcium (CaCl2), and 0.9 mmol/L phosphate ions (NaH2PO4,). 11,12 Both the demineralization and remineralization solutions were changed daily. The teeth were cycled separately in individual glass containers throughout the 14-day process, then stored in deionized water until the micro-CT scanning.
Micro-CT analysis
The brackets were debonded using bracket-removing pliers before micro-CT analysis, and each tooth was scanned individually by micro-CT (SkyScan 1172, SkyScan, Kontich, Belgium). All samples were scanned with X-rays at 100 kV and 100 mA, and rotated over 360 degrees with rotation steps of 0.5 degree with the help of a 0.5 mm thick aluminum and copper filter. Collected data were used to reconstruct a three-dimensional (3-D) image with a resolution of 2000 × 2000 pixels and a pixel size of 9.998 μm. The scanning results of each sample were reconstructed using the reconstruction software NRecon (SkyScan, Kontich, Belgium). Then, the reconstructed 3-D images were viewed and processed using the data analysis software CTan (SkyScan, Kontich, Belgium). In the reconstructed 3-D image of each sample, cross-sectional images showing the whole lesion on the buccal or lingual surface of the tooth were located. Then, the region of interest was drawn for each of the sampled images. In the second stage, with the help of the binary page, the thresholding of the lesion density was determined. Finally, the lesion depth in each of the selected images was measured through custom processing.
Three-dimensional modeling of a sample obtained by micro-CT analysis showing the formation of lesions is illustrated in Fig. 1a,b.
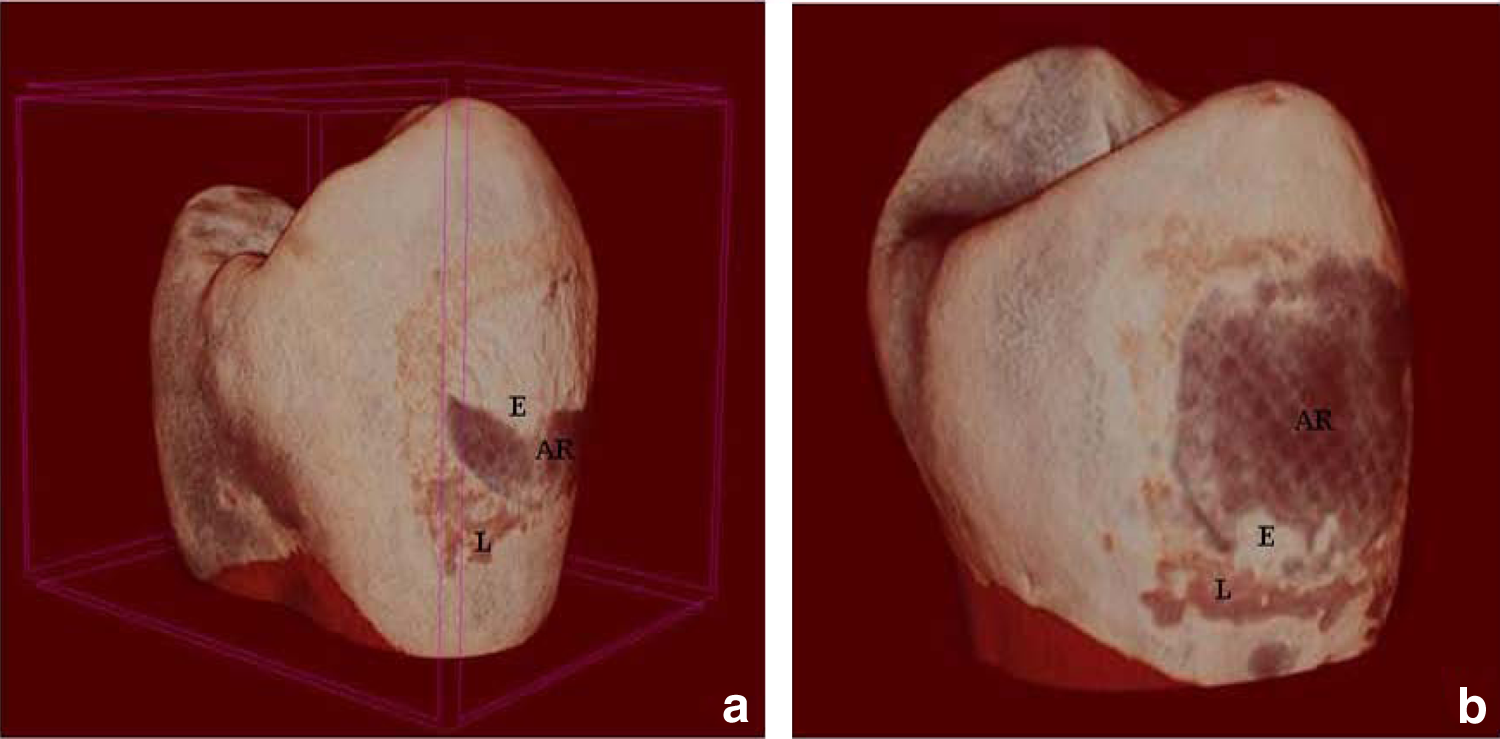
Three-dimensional modelling of a sample obtained with micro-CT analysis showing the formation of lesions (
Thermal cycles and SBS test
The samples were thermocycled (Dentester, Selubris Technica, Turkey) for 500 cycles between 5° and 55°C, using a dwell time of 20 sec to imitate the heat and humidity conditions of the oral cavity. Then, an Instron universal testing machine (Elista, Turkey) was used with a knife-edge blade located at the buccal–bracket interface parallel to the axis of the teeth at a crosshead speed of 0.5 mm/min. The failure load was recorded in Newtons (N) and converted to megapascals (MPa), dividing the force by the bracket base area of 9.61 mm2. After debonding the brackets, the buccal surfaces were examined at ×10 magnification using a stereomicroscope (S4E, Leica Microsystems, Germany).
The remaining adhesive was assessed according to the modified Adhesive Remnant Index (ARI) scores. 15
Statistical analysis
The records were statistically analysed by using SPSS (version 17.0; SPSS Inc, Chicago, IL). The Kolmogorov–Smirnov test was applied to test for normal distribution. ANOVA and post-hoc multiple comparison tests were used to compare the lesion depth and SBS values among the groups. The Kruskal–Wallis and Mann–Whitney U tests were used to analyze the distribution of the ARI scores. All tests were performed with a significance level of p < 0.05.
Results
Demineralization evaluation
The mean lesion depth (LD) values and the intergroup comparisons of the control, 1 W, and 2 W Er:YAG laser groups, and comparisons of all study groups are shown in Table 2. In the control groups, the lowest LD was found for G7. There were no significant differences in the mean LD values between G1 and G4. However, the differences between these groups and G7 were statistically significant (p < 0.05).
Significant at p < 0.05, letters indicate the comparisons of all study groups, and the same letters show no significant differences.
LD, lesion depth; ns, nonsignificant.
In the 1 W laser groups, the results of LD showed much the same changes. In other words, the lowest LD was found for G8. There were no significant differences in the mean LD values between G2 and G5. However, the differences between these groups and G8 were statistically significant (p < 0.05).
In the 2 W laser groups, the lowest LD was found for G9. However, the differences between the LD values among the groups were not statistically significant (p > 0.05). According to our results, the highest mean LD was found in G2 and the lowest was found in G7 among all the groups, and the differences among the groups were not significant except for G7 and G8.
SBS evaluation
The descriptive statistics of SBS values, intergroup comparisons of control, 1 W, and 2 W Er:YAG laser groups, and comparisons of all study groups are demonstrated in Table 3.
Significant at p < 0.05, letters indicate the comparisons of all study groups, and same letters show no significant differences.
SBS, shear bond strength; ns, nonsignificant.
In the control groups, the highest mean SBS was found in G4 and the lowest was found in G7. There were no significant differences in the mean SBS values between G1 and G4, but the differences between these groups and G7 were statistically significant (p < 0.05).
In the 1 W laser groups, the highest mean SBS was found in G8 and the lowest was found in G2. However, there were no significant differences in the mean SBS values among the groups.
In the 2 W laser-etched groups, the highest mean SBS was found in G9 and the lowest was found in G3. The differences between the mean SBS values of G3 and G9 were statistically significant (p < 0.05), whereas the differences between G3 and G6 and between G6 and G9 were not significant. According to the SBS values of all study groups, the highest mean SBS was found in G9 and the lowest was found in G7. The differences among the mean SBS values of study groups were not statistically significant, except for G7 and G9.
Modified ARI evaluation
The distribution of ARI scores, the intergroup comparisons of control, 1 W, and 2 W Er:YAG laser groups, and the comparisons of all study groups are shown in Table 4.
Significant at p < 0.05.
ARI, Adhesive Remnant Index; ns, nonsignificant.
In the control groups, the teeth in G1 had ARI scores between 4 and 5. Half of the teeth in G4 had ARI scores of 4, 25% had ARI scores of 3, and the others, except for one tooth, had ARI scores of 5. In G7, ∼60% of the teeth had ARI scores of 4, and 25% had scores of 5. One tooth had an ARI score of 2, and the remaining sample had an enamel crack. There were no significant differences in the distributions of the ARI scores of the control groups (p > 0.05).
In the 1 W laser-etched groups, half of the teeth in G2 had ARI scores of 4 and the other half had scores of 5. In G5, every type of scores was observed, but half of the teeth had scores of 3 or 4. One sample in this group had an enamel crack. In G8, except for the ARI score of 5, each type of ARI score was found. Half of the teeth had ARI scores of 3 or 4, and two teeth had enamel cracks. The differences in the 1 W laser-etched groups were statistically significant (p < 0.05).
In the 2 W laser-etched groups, half of the teeth in G3 had ARI scores of 5, and 25% of the teeth had scores of 4. Additionally, one sample had an enamel crack, and the remaining two teeth in this group had ARI scores of 3. In G6, most of the teeth had ARI scores of 3 or 4, whereas ∼17% of the teeth had ARI scores of 2, and the remaining two samples in this group had enamel cracks. In G9, most of the teeth had ARI scores of 1 or 2, and 25% of teeth in this group had enamel cracks. The differences between G3 and G9 and between G6 and G9 were statistically significant (p < 0.05).
The differences in all study groups were statistically significant (p < 0.05). Except for G1, G2, G3, G4, and G7, the differences between the distribution ARI scores of the other groups were not significant (p > 0.05).
Discussion
In orthodontic practice, the laser etching of enamel has become attractive in recent years because of the user-friendly procedure and the occurrence of acid-resistant enamel surfaces after laser etching. At this point, to determine which laser parameters and adhesive systems provide both adequate bond strength and demineralization prevention is challenging, considering the conflicting results obtained in most studies evaluating the bond strength of brackets after etching with an erbium laser. 8,9,13,16 –18
In our study, laser energy settings were chosen based on a previous study reporting Er:YAG that laser irradiation at 100–200 mJ and 10 Hz is suitable for enamel etching, providing significant protection against enamel demineralization. 11 In this study, the effectiveness of these parameters is examined using different adhesive systems. We aimed to find the most suitable bonding procedure for laser-etched teeth. Although Hossain et al. 19 reported that laser irradiation with or without water cooling appeared to be significantly effective in carious prevention, laser irradiation was performed with water mist in this study to prevent damage from overheating, such as cracks, carbonization, or melting of enamel. However, certain limitations of the previous demineralization studies 11,20,21 such as sample preparation for microscopic evaluation, were eliminated by using noninvasive micro-CT in our study.
According to the lesion depth results, CPB application was found to be most effective in preventing enamel demineralization compared with the control groups. This result may be because of the presence of fluoride in the material's composition, which indicates its capability to interfere with the development of enamel caries-like lesions. Contrary to our results, Paschos et al. 21 reported no statistically significant differences among the SEPs, CPB, and Transbond Plus for the non-fluoride-containing composite Transbond XT. In their study, all of these materials were stated to release fluoride. However, in the literature, no data are available about the amount of fluoride released by Transbond Plus. Moreover, laser etching and CPB combination was found to be more effective than the other 1 W laser etching procedures; however, 1 W laser irradiation with different types of adhesive systems did not create a positive effect on the prevention of enamel demineralization in this study. Consistently with many opinions, the formation of microspaces and microfissures under laser irradiation facilitated acid attack on the enamel surface, thus enhancing demineralization. 10,22 Our findings rejected the idea that laser etching might create remineralization microspaces by trapping free ions. 23 Lasmar et al. suggested that the use of an Er:YAG laser (Kavo Key Laser) at 80 mJ and 4 Hz caused less demineralization than acid etching when an etch&rinse adhesive system (Transbond XT Primer) was used; however, these parameters produced lower tensile stress strength than acid etching and demonstrated that the best results were obtained with a combination of laser and acid etching. 13
Because no prior studies had been published regarding lesion depth measurements around orthodontic brackets bonded to laser-etched enamel surfaces with one/two-step SEPs, our lesion depth results could not be compared precisely with other studies.
When the irradiation power of the Er:YAG laser was increased from 1 to 2 W, no significant differences were found among the groups, although 2 W laser etching and CPB showed higher lesion depth values than the control and the 1 W laser-etched with CPB application groups. According to our results, no positive effect on the prevention of enamel demineralization was found with increased laser irradiation. This result might be explained by the susceptibility of more irregular enamel surfaces roughened by increased irradiation energy to demineralization. This study indicated that different Er:YAG laser parameters of 1 W (100 mJ, 10 Hz) or 2 W (200 mJ, 10 Hz) for enamel conditioning could not prevent enamel demineralization when using different adhesives. Therefore, the first part of the null hypothesis was supported.
On the other hand, the second part of the null hypothesis was rejected based on the SBS results. Different combinations of Er:YAG laser irradiation and adhesive systems demonstrated significant differences in the SBS of orthodontic brackets. CPB application showed the lowest SBS values compared with the other two adhesives among the control groups. Our results were similar to the findings of studies showing that the SBS of brackets bonded with CPB was significantly lower than for brackets bonded with Transbond XT Primer and Transbond Plus SEP, 24,25 whereas other studies have reported the reverse findings. 26 –28 However, similarly to our findings, Dorminey et al. found that the differences were not significant between the SBS values of brackets bonded with Transbond Plus SEP and those bonded with Transbond XT Primer without laser etching. 29
Additionally, the results of this study indicated that Er:YAG laser etching at 1 W (100 mJ, 10 Hz) did not increase the SBS values of brackets bonded with Transbond XT Primer or Transbond Plus SEP. In contrast to our results, Hosseini et al. 16 reported significant differences between the SBS values of brackets bonded to Er:YAG laser (100 mJ, 10 Hz) etched or acid-etched enamel with Transbond XT Primer. They found that laser etching improved the SBS of brackets. 16 In the literature, conflicting results have been obtained from different studies evaluating the combination of etch&rinse adhesive (Transbond XT Primer) and laser etching, which are most likely related to the different study designs and various laser parameters.
In this study, the Er:YAG laser (100 mJ, 10 Hz) increased the SBS of brackets bonded with two-step SEP (Clearfil Protect Bond). Considering the protective effect against demineralization of this adhesive system, the Er:YAG laser (100 mJ, 10 Hz) could be preferred to improve the SBS of the brackets. It was also noted that this study was the first to evaluate the effect of different SEPs on the SBS of brackets bonded to laser etched teeth.
When the irradiation energy was increased to 2 W, higher SBS values of brackets bonded with Transbond Plus or Clearfil Protect Bond were observed, except for Transbond XT Primer application. However, the differences were not significant between the Transbond Plus and Transbond XT Primer applications, whereas they were significant for CPB and Transbond XT Primer. The Er:YAG laser (200 mJ, 10 Hz) greatly increased the SBS values of brackets bonded with Clearfil Protect Bond.
In this study, the evaluation of ARI scores demonstrated significant differences in bond failure sites among the groups, except for the control and Transbond XT Primer applications in the laser-etched groups. Both the control and Transbond XT Primer application groups with two different powers of Er:YAG laser showed bond failure between the enamel–adhesive interfaces, which caused fewer enamel fractures. This type of failure mode could be considered an advantage because it takes less time to remove the adhesive from the enamel surface in clinical practice. Although many authors 17,18 supported the opinion that the bond failure between bracket–adhesive resin interfaces is safe for enamel and diminishes the risk of enamel damage, our findings do not support this opinion. According to our results, the failure mode of bracket–resin interfaces is not safe for enamel, having caused enamel cracks. Moreover, more remnant adhesives were left on the enamel surface in proportion to the increased the Er:YAG laser irradiation energy in this study. These findings verified that the increase in laser irradiation could be attributed to increased SBS values. Consistent with the increased SBS values in Clearfil Protect Bond application from the control to 2 W laser groups, the remnant adhesives on enamel surfaces were significantly increased. However, these highest SBS values were close to the threshold that could damage the enamel surfaces. 30 Therefore, enamel cracks were observed in many samples in this bonding procedure. However, one or two samples showed enamel cracks in the other procedures, and these cracks might be linked to the greatly increased SBS values.
Conclusions
Our study showed for the first time that when the preferred adhesive system is two-step SEP for laser etched enamel, Er:YAG laser etching at 1 W (100 mJ, 10 Hz) would provide both adequate demineralization prevention and bracket bond strength.
Footnotes
Acknowledgments
This study supported by the Suleyman Demirel University Department of Scientific Research (Project number 3629-OYP-D2-13).
Author Disclosure Statement
No competing financial interests exist.