
Abstract
Introduction
P
Low-level laser therapy (LLLT) is a promising, innovative physical method for controlling postoperative discomfort and promoting tissue regeneration after surgical procedures without producing adverse effects. 4 –6 LLLT works through a mechanism of “photobiostimulation,” which stimulates soft tissue healing, reduces inflammation, provides nonpharmacological pain relief, improves the tensile strength of the wound, and increases the speed of healing. 4 However, the exact biological mechanisms by which photobiostimulation operates are not fully understood. It has been suggested that LLLT is able to reduce pain through neuropharmacological effects produced by the synthesis, release, and metabolism of biochemical substances that include increases in β-endorphin and nitric oxide production, inhibition of C-fiber afferent-nerve depolarization, axonal sprouting and nerve cell regeneration, decreases in bradykinin levels, increases in acetylcholine release, or ion channel normalization. 7 –12 Boschi et al. 5 reported the anti-inflammatory effects of LLLT to be caused by the dose-dependent inhibition of interleukin (IL)-6, monocyte chemotactic protein (MCP)-1, IL-10, and tumor necrosis factor (TNF)-α, which stimulates phagocytic activity, increases the number and diameter of lymphatic vessels, decreases blood vessel permeability, and restores microcapillary circulation, thereby normalizing vascular wall permeability and decreasing edema.
The literature includes clinical studies as well as case reports examining the use of photostimulation to relieve postoperative discomfort and promote wound healing after dental surgery. 13 –16 Paschoal et al. 14 reported that LLLT did not significantly decrease postoperative pain or accelerate tissue repair in adolescents following premolar extraction when compared with a control group that received no LLLT. Similarly, López-Ramírez et al. 15 concluded that the application of a low-level laser did not show beneficial effects in reducing pain, swelling, or trismus after removal of impacted mandibular third molars. By contrast, Ferrante et al. 16 reported that LLLT was useful for the reduction of postoperative discomfort after third molar surgery. With regard to the literature on the pediatric population, there are a few case reports 13 showing LLLT to reduce postoperative discomfort following dental procedures; however, no published study has compared the effects of photobiostimulation on postoperative discomfort in children following primary tooth extraction. Therefore, this study aimed to evaluate the effectiveness of LLLT in controlling postoperative pain associated with tooth extraction in pediatric patients. Postoperative complications and analgesic usage were also evaluated.
Materials and Methods
The study protocol was approved by the Ethics Committee of Kocaeli University (#349/2014), and written informed consent was obtained from parents and patients prior to treatment. Based on data from a pilot study, a minimum sample size of 34 subjects was calculated using the G*Power software program (Ver. 3.1.9.2; power 0.80, α = 0.05, β = 0.20). Allowing for the possibility that children/parents might subsequently drop out of the study for various reasons, the first 40 children 6–12 years of age applying for routine dental treatment at the Kocaeli University Paediatric Dentistry Clinic who met the inclusion criteria and agreed to participation were selected for the study.
All patients required symmetric bilateral primary molar extractions in the maxilla or mandible with similar levels of operative difficulty. When the root, crown, and remaining bone structures were similar sizes on a radiographic examination, the case was considered to entail a similar degree of operative difficulty. Teeth were included in the study if at least two thirds of root formation was complete and if abscess/infection did not exceed one third of the inter-radicular area. Because anxiety may affect the perception and rating of pain, anxiety levels of children and parents were evaluated prior to the study using Corah's Dental Anxiety Scale (DAS), 17 and children and parents who scored ≤12, indicating moderate or no anxiety, and children who did not have tooth extraction experience previously, were also included in the study. Finally, children without a history of prolonged bleeding, platelet disorders, hypersensitivity, and allergic reactions to analgesics or contraindications to laser therapy as well as children without acute pain were included in the study. Children whose parents did not provide a telephone contact number or who were unavailable for supervision during the postoperative period were excluded from the study.
The study was conducted using a randomized, controlled crossover, blind design. All extractions were performed at the same time of day (1.30–2.30 p.m.) with an interval of 1 week between procedures. Maxillary teeth were anesthetized using infiltration anaesthesia, and mandibular teeth were anesthetized using inferior alveolar nerve block anaesthesia. Prior to injection, the injection site was dried, and topical anaesthetic (Hurricaine, Beutlich, 1541 Shields Drive Waukegan IL) was applied with a cotton tip applicator to the area for 60 sec. Local anaesthesia was achieved using articaine hydrochloride with 1/100,000 epinephrine (Ultracaine D-S forte, Hoechst Canada Inc., Montreal Quebec, Canada).
A total of 98 extractions were performed. All molars were extracted by the same investigator with a minimum of surgical trauma through luxation and avulsion. No complications occurred during any of the procedures. Postoperative instructions on diet and oral hygiene were given to the patients and parents. No suggestions regarding postoperative pain were mentioned to children or parents during or after the extraction procedures, and no medication was prescribed.
Postoperative laser application was performed by another investigator with 5 years of experience in using the diode laser device. In each patient, one post-extraction site was treated with laser irradiation immediately following extraction (LLLT group, n = 49), whereas the contralateral site received no irradiation (control group, n = 49). The extraction site (left or right) and the treatment procedure at the first appointment (LLLT or control) of a patient were chosen randomly using R 2.11.1 software (R Foundation for Statistical Computing, Vienna, Austria). Randomization and allocation of the groups were performed only by a person who did not perform the extraction or application of the LLLT. Patients and their parents were blinded to the groups by going through the same procedures for both teeth, but without activation of the laser in the control tooth.
LLLT was applied only once immediately after primary tooth extraction. LLLT was performed using a diode laser device (Cheese Dental Diode Laser; GIGAA LASER, Wuhan Gigaa Optronics Technology Co., China) with a continuous wavelength of 810 nm placed in a 400 μm hand piece. After checking for bleeding, the dentist placed the laser probe 1 cm from the target area, and 300 mW (0.3 W) of laser energy was applied to three different points (vestibular, lingual, and occlusal) for 60 sec each (0.3 W × 60 sec = 18 J per point). 16 The total LLLT energy for 180 sec was calculated as 4 J/cm2. 18 The operator and patients wore appropriate eye protection during laser and simulated laser application. The output power of the equipment was measured using a power meter three times during the study (Vega Power Meter, Ophir Photonics, 3050 North 300 West North Logan, USA).
Postoperative pain was measured subjectively through children's evaluations and objectively through data provided by parents. Children were asked to evaluate their pain levels using the Wong–Baker FACES® Pain Rating Scale (PRS) 19 (Fig. 1), which consists of a set of cartoon faces with varying facial expressions ranging from a smile/laughter to tears, and children were asked to select the facial expression that best represented their discomfort. Children and parents were trained to use the scale by an investigator blinded to the study groups, who first modelled use of the scale and then asked each participant to “think of the last time she/he felt something painful” and to select the facial expression that best represented his/her experience of discomfort. Parents were asked to evaluate their children's pain levels using a 10 cm visual analogue scale (VAS) 20 (Fig. 1), with 0 cm indicating no pain and 10 cm indicating the worst possible pain. Following the extraction procedures, both scales were given to parents so that they could implement the scales at home. On the first three evenings following treatment, the same investigator who provided the training telephoned parents at the same time each evening to record reported pain levels and whether or not children had experienced any complications or had received any analgesics. The VAS was first implemented by parents, after which the PRS was implemented by children with the help of their parents. Pain scale ratings were classified as follows: 0, “no pain”; 0.1–2.0, “mild pain”; 2.1–4.0, “moderate pain”; 4.1–6.0, “severe pain”; 6.1–8.0, “very severe pain”; and 8.1–10, “worst possible pain.”

The visual analogue scale (VAS) and the Wongs–Baker FACES® Pain Rating Scale (PRS). Each have end-points where 0 = no pain, 10 = worst possible pain.
Statistical analysis was performed using the SPSS software program (SPSS 20.00; SPSS, Chicago, IL). Data were analysed using χ2 and Wilcoxon signed rank tests. The Spearman's rank correlation coefficient was used to make pairwise comparisons between the parental ratings and the children's ratings.
Results
A total of 40 children were included in this study; however, 3 patients were subsequently excluded (1 presented with varicella during the course of the appointments, and parents of 2 others could not be reached for data collection). Finally, the study was conducted with 98 teeth in 37 children [13 girls (35.1%), 24 boys (64.9%)] 6–12 years of age (mean age: 8.08 ± 2.046). In 25 children, one molar was extracted per side, and in 12 children, two molars were extracted per side. Nine children had maxillary teeth extracted, and 28 children had mandibular teeth extracted (Table 1). None of the patients showed any adverse reactions to the treatment.
On the first evening following treatment, 21.62% of children in the control group and 16.21% in the LLLT group received analgesics. On the second and third evenings, only 5.40% of children in both groups received analgesics. Amounts of postoperative analgesics did not vary significantly by group, gender, or number/location of extracted teeth (p > 0.05) (Table 2).
Fisher's exact test, no significant difference (p > 0.05).
Correlation is significant (p < 0.01).
Pain ratings provided by parents (VAS) and children (PRS) showed significant correlation, with p values of <0.01. The correlation coefficient ρ varied between 0.768 and 1.00 (Table 2).
Figures 2 –4 show the VAS and PRS scores for postoperative pain on the first, second and third evenings, respectively. For both the VAS and PRS scales, the number of “no pain” scores increased from the 1st to the 3rd day in both the LLLT and control groups. Only one rating of pain as the “worst possible” was given (on the first evening, in the control group) and “severe” or higher pain ratings were given only on the first evening in the LLLT group and on the first and second evenings in the control group. Whereas the LLLT group had more “no pain” responses than the control group on the first evening, the control group had more “no pain” responses than the LLLT group on the second and third evenings according to both VAS and PRS. Whereas mean pain scores reported by parents (VAS) were higher for the control group than for the LLLT group on both the first and second evenings following treatment, mean pain scores reported by children (PRS) were higher for the control group than for the laser group on the first evening only. Median PRS and VAS values also differed between the two groups on the first evening only (Table 2). No significant differences were found in postoperative pain ratings of either parents or children by gender, age, or number or location of extracted teeth (p > 0.05).
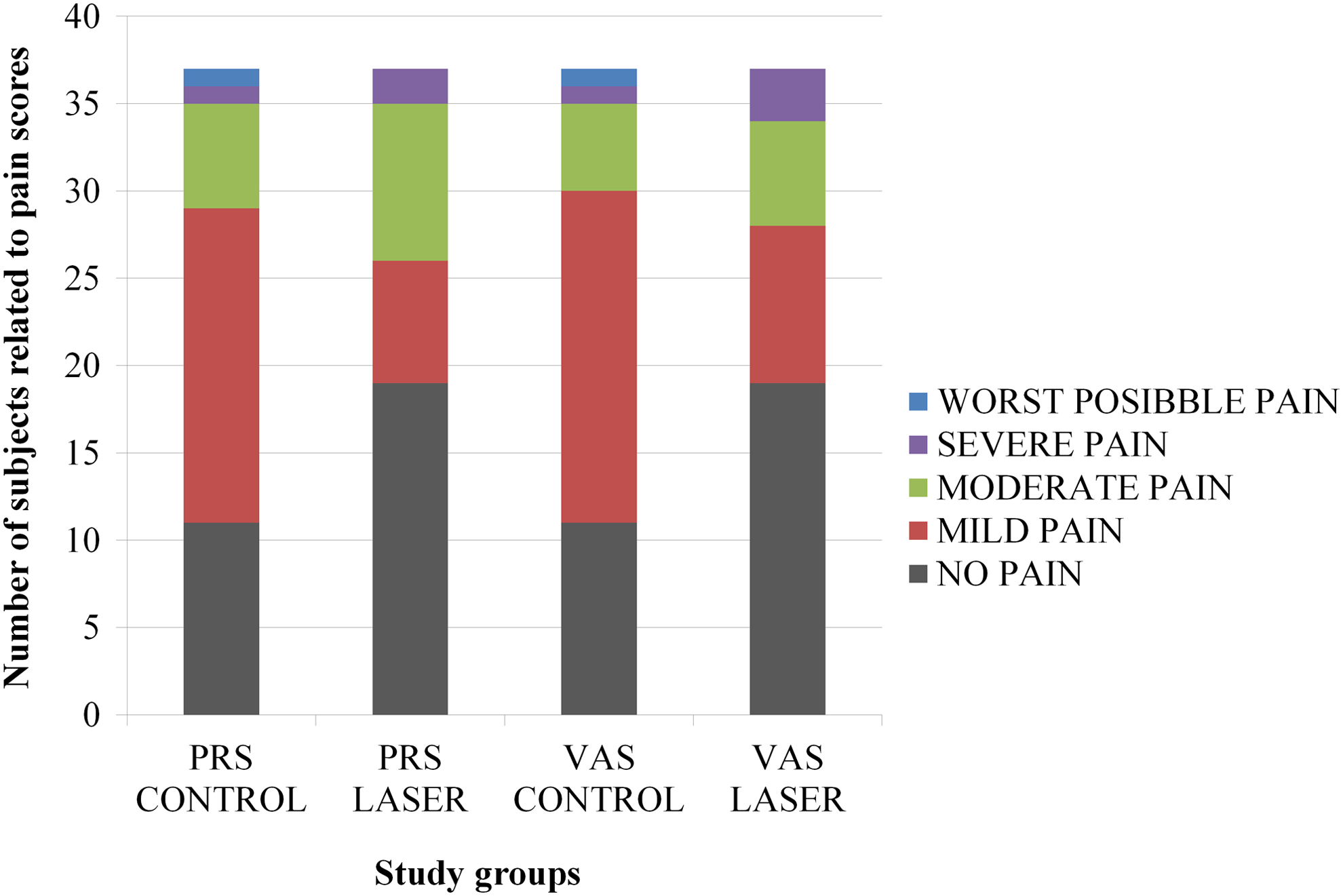
Post-extraction pain ratings on the evening of the treatment day, day 1. Children's self-ratings on the Wongs–Baker FACES® Pain Rating Scale (PRS) (n = 37) and parental ratings on the visual analogue scale (VAS) (n = 37) (control, extractions without laser application; laser, extractions with laser applications).

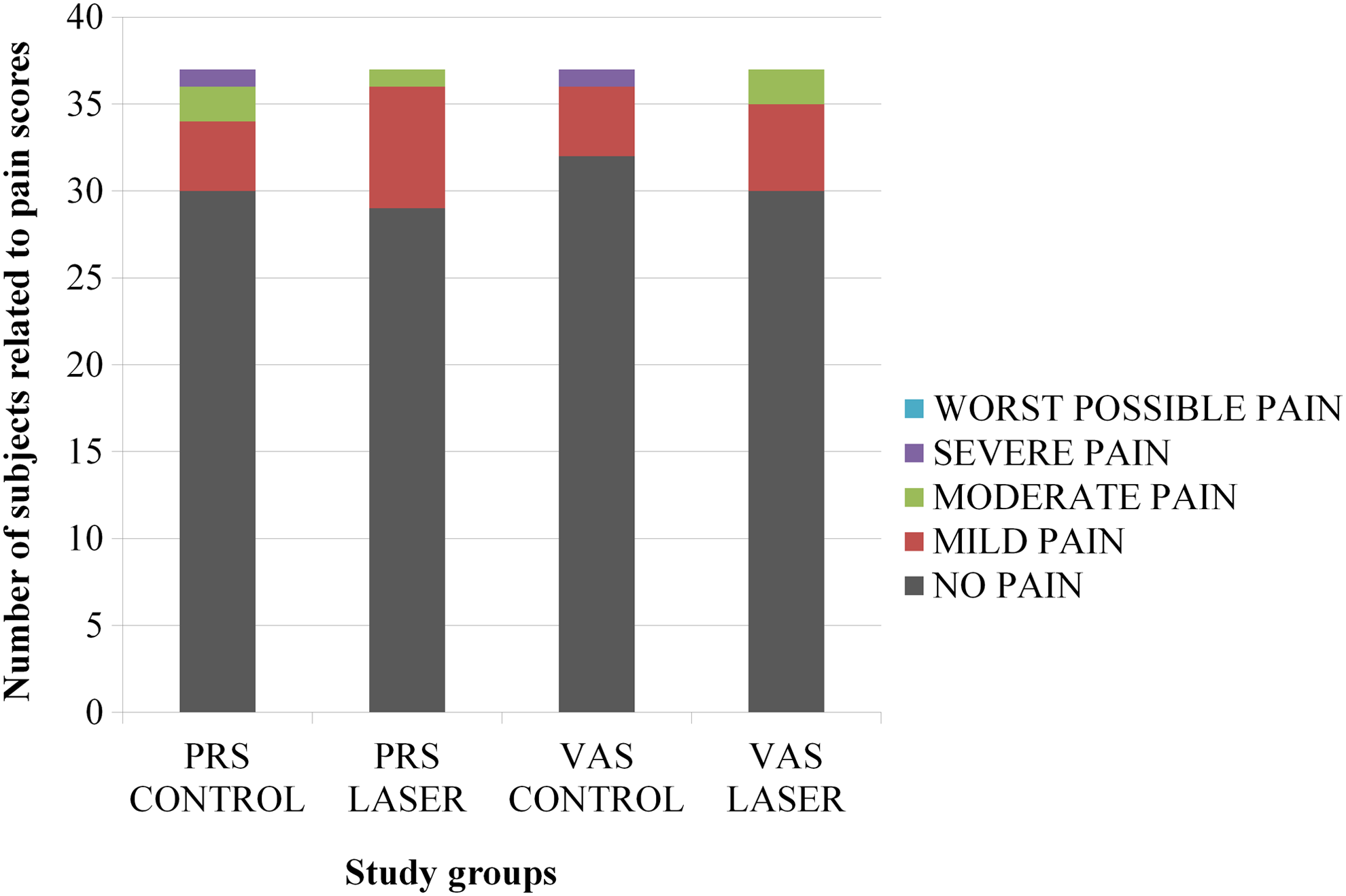
Post-extraction pain ratings on the evening of the treatment day, day 2. Children's self-ratings on the Wongs–Baker FACES® Pain Rating Scale (PRS) (n = 37) and parental ratings on the visual analogue scale (VAS) (n = 37) (control, extractions without laser application; laser, extractions with laser application).
Post-extraction pain ratings in the evening of the treatment day, day 3. Children's self-ratings on the Wongs–Baker FACES® Pain Rating Scale (PRS) (n = 37) and parental ratings on the visual analogue scale (VAS) (n = 37) (control, extractions without laser application; laser, extractions with laser applications).
There were no significant differences between the two groups in terms of other postoperative complications. None of the patients reported complications severe enough to require clinical treatment; no patients reported swelling, infection, or hematoma; and only two patients in the LLLT group and one patient in the control group reported lip biting after mandibular tooth extraction. There were no associations between reporting lip biting and higher pain ratings.
Discussion
This study revealed that LLLT did not significantly reduce postoperative pain associated with primary molar extraction in either the maxilla or mandible. These results are compatible with some studies in the literature, 14,15 but inconsistent with others. 16,21 However, all these previous studies evaluated extractions of third molars 15,16,21 or other permanent teeth, 14 whereas, to the best of our knowledge, no clinical study has evaluated the efficacy of LLLT after primary molar extractions in children, making it difficult to compare data between the present study and previous studies. A case report by Paschoal et al., 13 in which LLLT was applied after extraction of a supernumerary tooth in a 10-year-old boy, reported the patient's pain responses to vary between 2 and 3 (VAS) during the first 12 h postoperatively and between 0 and 1 thereafter, and that no pain medication was required. The authors concluded that the application of LLLT after surgical procedures reduces postoperative pain in children.
A slight positive effect of LLLT was observed in the present study in that more parents and children in the laser group than in the control group reported “no pain” on the first evening following extraction; the only report of “worst pain” was on the first evening from one child/parent in the control group; the only reports of “severe pain” on the second evening were from children/parents in the control group; and the rate of postoperative analgesic usage was higher in the control group than in the LLLT group. However, the differences between the two groups were not statistically significant. This may be attributed to the fact that laser treatment was applied immediately as well as 24 and 48 h postoperatively in the study by Paschoal et al., 13 whereas in the present study, LLLT was applied only once immediately after primary tooth extraction, because it was thought that children and parents were likely to be too busy to attend additional treatment sessions.
LLLT is defined by several parameters, including power (between 10−3and 10−1), wavelength (300–10,600 nm), pulse rate (0–5000 Hz), pulse duration (1–500 ms), total irradiation time (10–3000 sec), intensity (power/area)(10−2–100 W/cm2), and dose (power × irradiation time/irradiated area) (10−2–102 J/cm2). 22 –26 Differences in these parameters make it difficult to compare the findings of previous studies. Despite the fact that the LLLT protocol used in the current study was adapted from previous studies 16,18 that demonstrated LLLT to reduce postoperative pain following the extraction of impacted mandibular third molars, the current study found that LLLT application did not significantly reduce postoperative pain following primary molar extraction. Markovic et al. 18 compared the use of single session low-power laser irradiation and the nonsteroidal anti-inflammatory drug diclofenac on postoperative pain after surgical extraction of lower third molars, and concluded that the use of low-power laser irradiation after surgical extraction reduces postoperative pain. They attributed this success to the dose-dependent effect, and suggested that output doses of laser energy <4 J/cm2 would not significantly influence the postoperative pain intensity. In the present study, although 4 J/cm2 energy was given, the decrease in pain intensity was not statistically significant. This may be for several reasons. One of them is the difference between the evaluated extraction sites in the two studies. Although in a third molar surgery, extraction wounds are generally closed primarily by interrupted sutures, in the present study, the extraction area was left for secondary healing. Laser–tissue interaction depends not only on the parameters of the laser used, but also on the optical properties of the tissue. 27 The exact percentages of laser light reflected, scattered, transmitted, and absorbed by tissue are unclear, but may be expected to vary among individuals and to be dependent on tissue thickness and molecular composition. 25,28,29 In the present study, although the bleeding was controlled after extraction before laser application, it may not be sufficient, as suturing of the wound, and the given energy dose, may be affected negatively because of the low transmission and strong scattering of light by blood. 30 Moreover, because of the reasons mentioned, making comparisons between studies conducted with adults and with children or with laser applications for different indications could be misleading.
Although the literature includes numerous studies evaluating dental pain in adults, there are relatively few studies on dental pain in children. There are several reasons for this, including a mistaken belief that children do not perceive pain, or that they cannot communicate pain, or that the procedures themselves are not painful. 31,32 However, a study by Acs et al. 33 concluded that children do experience post-extraction pain, and that some children experience pain of sufficient intensity to require an analgesic for post-extraction pain relief. According to Staman et al., 31 ∼19% of children undergoing dental extractions reported postoperative pain. This is in line with the present study's finding that 22% of the control group described pain following primary tooth extraction as “moderate” to the “worst possible” pain. Moore et al. 34 found that a higher rate (33%) of children reported moderate or higher levels of pain following extractions; however, their study evaluated pain after extraction of both primary and permanent teeth, whereas both Staman et al. 31 and the present study evaluated pain following primary-tooth extraction only. In addition, the present study found similar rates of pain reported by boys and girls, which was consistent with the results of the previous studies. 31,35
Previous studies have indicated that children reporting pain following extraction often require analgesics. Both Staman et al. 31 and Primosch et al. 36 reported the rate of analgesic usage following extraction to be higher (52% and 30%, respectively) than the rate of reported pain (40% and 19%, respectively). However, in the current study, both rates were similar, with 22% of children reporting “moderate” to “worst possible,” pain, and 22% using analgesics on the first evening following extraction. Staman et al. 31 suggested that the disparity between reported pain and analgesic usage could be the result of parents' heightened levels of anxiety in association with tooth extraction, causing them to give their children pre-emptive analgesics. The similar rates of postoperative pain and analgesic usage found in the present study may be explained by the fact that this study screened both children and parents for anxiety using a DAS, and children whose parents showed higher levels of anxiety were excluded from the study, which might have prevented any unnecessary, pre-emptive analgesic usage.
Children's physical, psychological, and cognitive development play important roles in how they experience pain, making pain assessment in children a particularly complex process. 37 In order to improve the reliability of reported pain scores, the present study measured postoperative pain using subjective evaluations of children and objective evaluations of parents. Whereas Primosch et al. 36 evaluated post-extraction pain in children using parental reports only, Jensen 28 also evaluated post-extraction pain in children using reports of both children and their parents, and, in line with the findings of the present study, found good agreement between children's self-ratings and the assessments of their parents. In the present study, in order to avoid children biasing their parents' rating, parents' scores were recorded first. The fact that children were not blinded to their parents' evaluations represents a limitation of this study, because children may have been unconsciously influenced by their parents' scores. In order to reduce the risk of such bias, different scales were used for parents and children. However, it has previously been reported that parents, especially mothers, can be relied upon to provide objective assessments of their children's pain levels. 38 Moreover, in order to reduce the risk of parents overestimating their children's pain levels because of their own fears regarding dental treatment, the present study excluded children whose parents showed high levels of anxiety on a DAS screening conducted prior to treatment.
In the present study, the crossover design was used; therefore, the patients were their own control and this eliminated the bias in information collection also. In addition to this; although the researchers who evaluated post-extraction pain in children did not separate primary tooth extraction for mandible or maxilla, and, moreover, in a study by Sammons et al., 39 reported that the jaw location of the teeth did not affect the postoperative pain, the present study was conducted using only bilateral extractions on the same jaw to standardize the degree of surgical difficulty.
The use of analgesics and/or local anaesthetics administered intraoperatively during dental rehabilitation may delay pain responses in some patients, who may then report a greater intensity of pain when they return home following the procedure. 40 Al-Khateeb and Alnahar 41 reported that patients undergoing uncomplicated tooth extraction experienced the highest intensity of pain the evening following extraction and that more than half of the patients used analgesic drugs. In the present study, extractions were performed at the same time of day (1.30–2.30 p.m.) to achieve standardization, and pain severity and analgesic usage were recorded on the first, second, and third evenings following extraction.
In the present study, although LLLT was, in general, found to be ineffective in reducing postoperative pain following primary tooth extraction, LLLT may still prove beneficial for some individuals. Considering the complexities involved in pain reduction and wound healing with photobiostimulation, and the study group consisting of the low-anxiety children, additional research is need to determine how different laser parameters, extraction sites, and individual characteristics influence the effectiveness of LLLT in children.
Conclusions
Within the limitations of this study, postoperative LLLT applied intraorally using an 810 nm diode laser was not found to have a significant effect on postoperative pain in children following primary molar extraction, regardless of gender, number of extracted teeth, or jaw location.
Footnotes
Author Disclosure Statement
No competing financial interests exist.