
Abstract
Keloids are scars that grow beyond the boundaries of a cutaneous injury, inflammation, surgical incision, or burn. They are the result of an overgrowth of dense fibrous tissue that usually develops after healing of a skin injury, and do not usually regress spontaneously. In addition to symptomatic relief, cosmetic concern is the primary reason patients seek medical intervention. Therapeutic options such as occlusion dressings, intralesional corticosteroids or interferon injections, silicone gel application, cryotherapy, irradiation, and ablative lasers have been used in various combinations. We present the results from two patients who underwent UVA1 laser therapy.
Introduction
K
Case Reports
Case 1
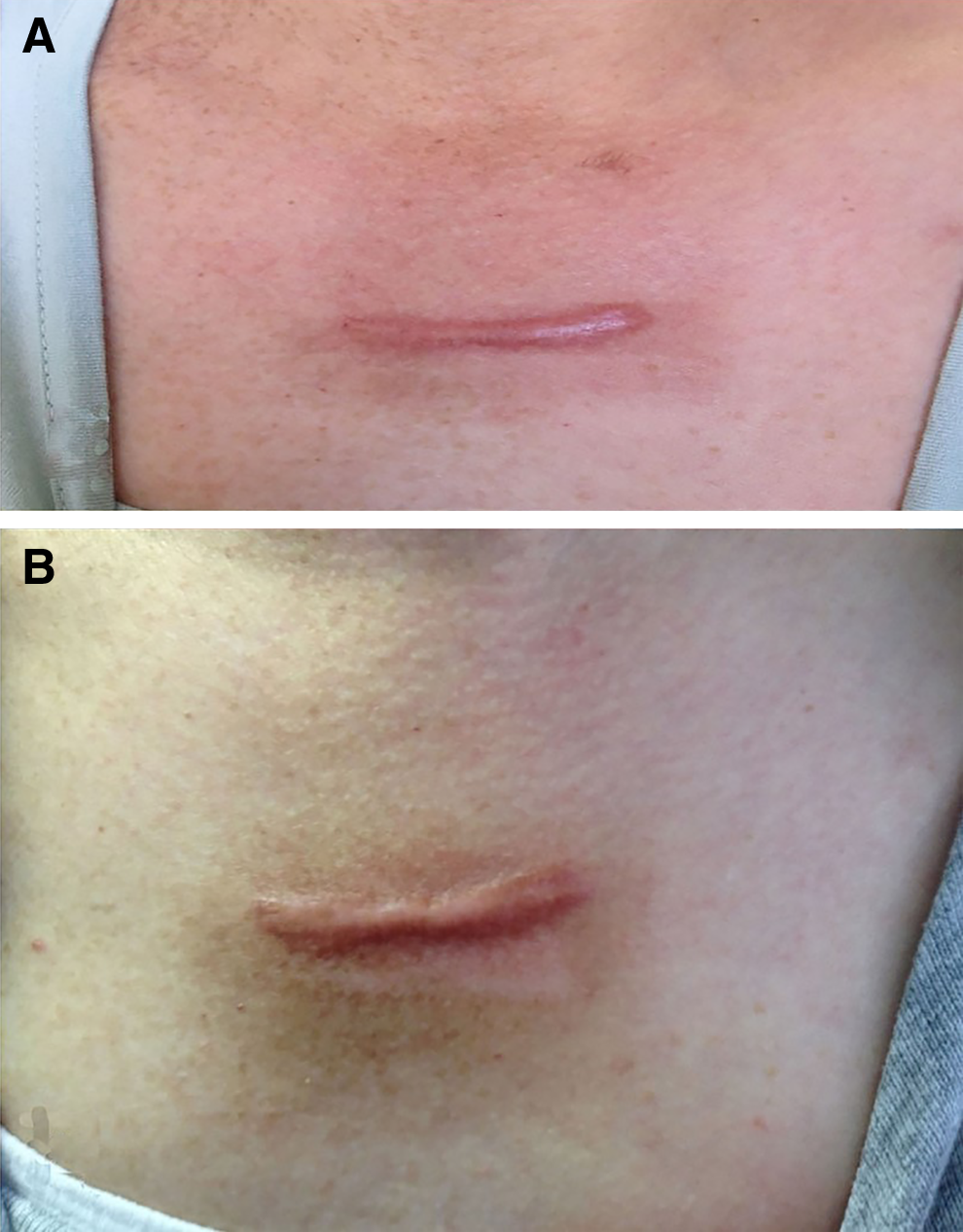
A 52-year-old healthy female with Fitzpatrick phototype III presented for the treatment of a keloid scar on the V-region of her chest (Fig. 1A). She had been treated with intralesional injections of triamcinolone acetonide 3 years earlier. The keloid was 4.2 cm in diameter and extended 3 mm above the skin surface. The VSS score of the lesion was 7 just before treatment. The patient was treated with a UVA1 355 nm laser (Alba 355) at 140 J/cm2 three times a week as described by Zerbinati et al. 7 for the first 3 weeks, and then at 160 J/cm2 for 3 weeks, 180 J/cm2 for 2 weeks, 230 J/cm2 for 2 weeks, and 250 J/cm2 for 2 weeks. At the end of the treatment period, we observed softening, flattening, and decreased vascularity of the irradiated keloid, which was 3.7 cm in diameter and extended 1.7 mm above the skin surface (Fig. 1B); the VSS score after treatment was 4 (Table 1). The patient tolerated the treatment regimen well, and her complaint of itching and tenderness decreased significantly.
Case 2
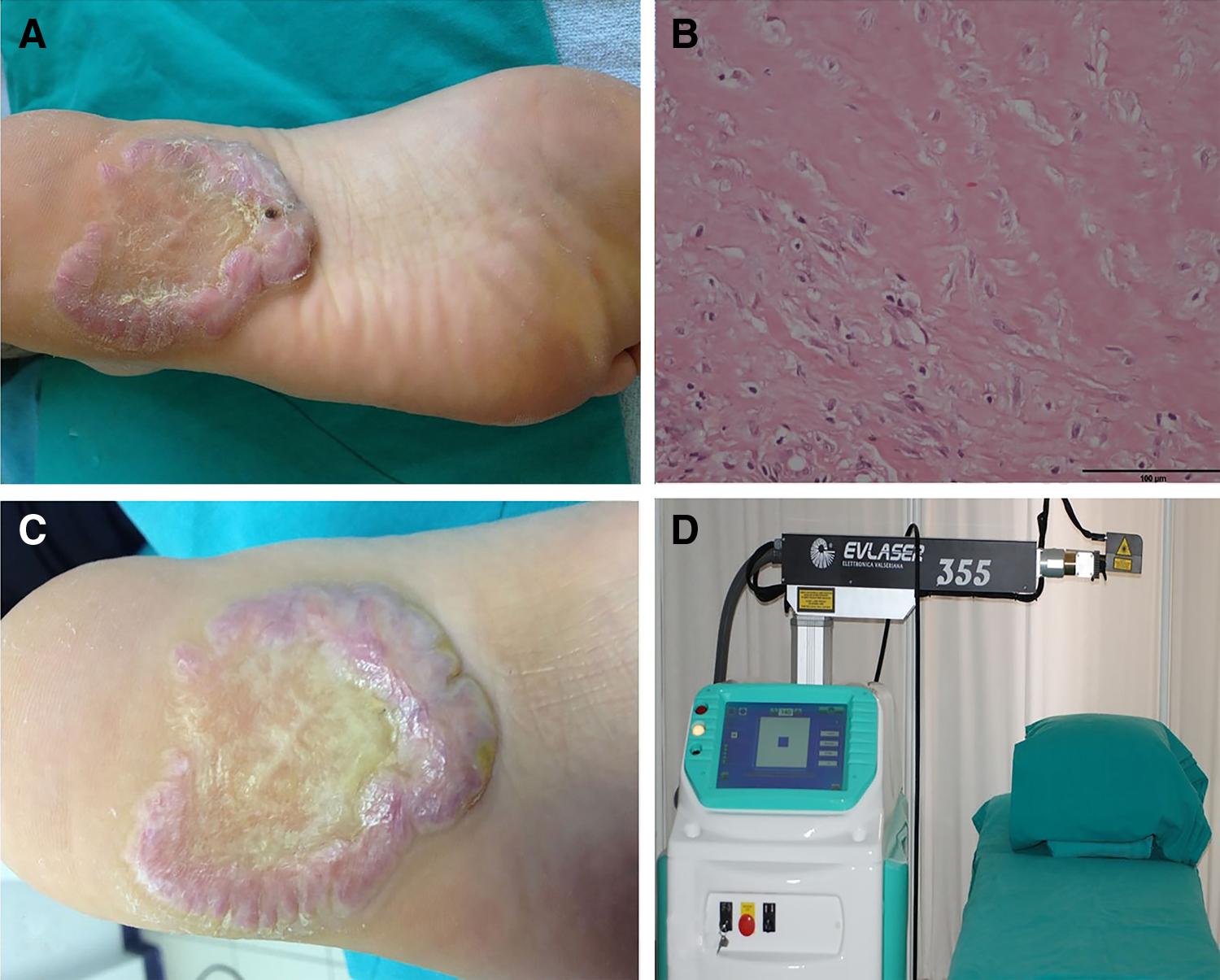
A 38-year-old male with Fitzpatrick phototype II presented with a painful, solid, raised lesion on the plantar area of his right heel that had been present for 8 years. The patient had previously undergone minor surgical excision of a callus at the site of the lesion. Following the procedure, an even larger lesion appeared in the same area. The patient was treated with intralesional triamcinolone acetonide 12 times and then with 5-fluorouracil 5 times a month at different times. Despite this treatment, significant recuperation was not observed. A cutaneous examination revealed a single well-defined, elliptical, stony, hard, tender, and dense erythematous keloidal growth under the right heel of the patient's foot (Fig. 2A). The keloid was 6.5 cm in diameter and extended 7 mm above the skin surface. The VSS score was 10 just before treatment. A biopsy was performed. Histopathological analysis indicated fibrotic tumors characterized by a collection of atypical fibroblasts and excessive deposition of extracellular matrix components, leading to disorganized, thick, hyalinized collagen fibers with a prominent mucoid matrix (Fig. 2B). The patient was diagnosed with a keloid. We applied increasing dosages of a UVA1 laser according to the following protocol: 160 J/cm2 three times a week for the first 2 weeks and then 180 J/cm2 for 2 weeks, 230 J/cm2 for 3 weeks, and 250 J/cm2 for 6 weeks. After 3 months of therapy, the keloid was 5.5 cm in diameter and extended 4 mm above the skin surface. The erythema of the lesion was diminished and the VSS score was reduced to 5 (Fig. 2C and Table 1).
Discussion
Several treatment modalities have been shown to be useful for the management of keloids; however, no single modality is completely effective. 1,8 UVA1 irradiation has been reported to be effective for the treatment of morphea and systemic sclerosis through the induction of collagenase I [matrix metalloproteinase I (MMP-1)] production by fibroblasts and decreased synthesis of procollagen. 9 The efficacy of UVA1 for the treatment of morphea and other conditions such as keloid scarring may be partly the result of this action.
In keloidal tissue, transforming growth factor beta (TGF-β) is overproduced and poorly regulated through normal autocrine signaling mechanisms. Most cells involved in wound healing express TGF-β in an inactive form that strongly promotes the chemotaxis of fibroblasts to the site of injury. 9,10 Moreover, growth factor (GF)-β and platelet-derived growth factor (PDGF) play critical roles in fibroblast proliferation and collagen production. 9,10 At the same time, keloid fibroblasts exhibit increased numbers of growth factor receptors and respond more intensely to growth factors such as TGF-β and PDGF. 9,10 The upregulation of interleukin (IL)-1 after exposure to UVA radiation (340–450 nm), which plays a direct role in the subsequent production of IL-6, is thought to mediate the upregulation of collagenase in fibroblasts. Interferon gamma may have an inhibitory effect on collagen production and is increased by UVA1 exposure. UVA radiation decreases the activity of propyl hydroxylase, which stabilizes the triple helical structure of collagen. UV radiation may also impair the cross linking of collagen fibers. UVA exposure leads to the production of hydrogen peroxide. Hydrogen peroxide increases the expression of collagenase/MMP-1 messenger RNA in human dermal fibroblasts. 10 The longer the wavelength used, the greater the depth of penetration by UV light. Therefore, treatment with UVA1 (340–400 nm) is more effective than treatment with UVA (320–400 nm) for sclerotic skin diseases, because of the greater depth of penetration. 10 UVA1 photons exert their effects via the induction of collagenase messenger RNA expression, the depletion of skin T cells, cytokines (IL-1 and IL-6), and neovascularization. 10
UV radiation (355 nm), which requires less energy for the ablation of the stratum corneum, has a greater impact on lipoid structures without producing lesions in the epidermis. 7 Our patients were treated with a new UVA1 355 nm laser (Alba 355; Elettronica Valseriana, Casnigo, Italy) (Fig. 2D) that administers energy in the UVA1 spectrum. This new laser system was successfully used to treat psoriasis by Zerbinati et al. 7 and Nistico et al. 11 This solid-state laser uses an active medium and a neodymium-doped yttrium orthovanadate (Nd:YVO4) crystal that is energetically pumped by another laser with a wavelength of 808 nm. The light emitted by the Nd:YVO4 crystal, at a wavelength equal to 1064 nm, is pulsed through an acousto-optic crystal called a Q-switch, which produces a frequency of 20–50 kHz and transforms the laser light into ultrashort pulsed light (25 ns). This pulse rate is >40 kW, and it is sent to crystals to duplicate and triplicate the 1064 nm wavelength-producing second (532 nm) and third (355 nm) harmonic wavelength delivery. 7
In our analysis, an improved VSS score was observed in keloid patients treated for up to 12 weeks at three sessions a week with high-dose UVA1 laser therapy. We did not observe any side effects; however, long-term side effects cannot be ruled out. The biggest challenge in applying high-dose UVA1 therapy is that the treatment is time consuming; a single treatment takes ∼45 min, and patients must be treated three times a week for 3 months. Therefore, high-dose UVA1 therapy should be attempted in combination with other treatment options to reduce the overall UVA1 dose/time. Further study with a greater number of patients is required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.