
Abstract
Introduction
W
Three types of lasers have been widely employed in wart removal: carbon dioxide (CO2), erbium-doped yttrium aluminum garnet(Er:YAG), and pulsed dye laser (PDL). 3,4 CO2 laser ablation has been associated with side effects such as production of smoke containing HPV particles, which are hazardous to both the doctor and patient. 5 –7 The Er:YAG laser was employed in an attempt to reduce the side effects of the CO2 laser, but still produces fumes necessitating the use of a smoke evacuator and facial mask by both doctor and patient. These ablative lasers are also expensive, time-consuming, and have limited indications. While they target water in wart tissue, PDL targets hemoglobin in the vessels, which explain the occurrence of purpura after treatment.
The long-pulsed neodymium-doped yttrium aluminum garnet (Nd:YAG) laser is rarely used for wart removal because it requires prior paring of the wart keratinous surface. 8 However, this laser is less expensive, has more indications, and does not produce smoke. The present study aimed to assess the safety and efficacy of a new protocol for palmoplantar wart removal using long-pulsed 1064-nm Nd:YAG laser without prior paring of the wart surface, but instead with prior application of a moisturizing cream in 240 consecutive Yemeni patients. This new protocol was based on results of previous studies of the optical properties of psoriatic skin. These studies demonstrated that the application of a lipophilic liquid could maximize the selective penetration of all optical wavelengths into psoriatic skin. The regular reflectance of the wart surface decreased on applying the cream as it provided a better match of the refractive index between the layers of skin. 9 Since there is a great similarity between the histology of psoriasis and warts, we hypothesized that application of a moisturizing cream over the wart's surface will decrease reflectance and increase penetration of the laser into the deep wart tissue. The novel aspect of our study is the prior application of a moisturizing cream to the surface of the warts, which has three advantages. First, it prevents the development of fire and smoke, which are hazardous to both the patient and personnel. Second, it helps deliver the laser energy to the deepest layers of the wart tissue, thus increasing the success rate. Third, it saves the time needed for paring the wart surface, and consequently reduces the total time needed for wart removal.
Patients/Methods
Patients
Over a 4-year period (2011–2014), 240 Yemeni patients(142 males, 98 females; age 5–67 years) with a total of 2929 lesions presenting to the Dermatology Department of University Hospital in Sana'a, Yemen, with recalcitrant or untreated palmoplantar warts were included in this study. The exclusion criteria were previous treatment during the last 6 months, history of hypertrophic scars or keloid, and active bacterial or viral infection at the site of laser treatment. Written informed consent was obtained from the patients or their parents before initiation of the study, which was approved by the ethics committees at Sana'a University.
Treatment protocol
The study employed a 1064-nm long-pulsed Nd:YAG laser (Quanta System, Solbiate Olona, Italy). All patients underwent 1–3 sessions of laser treatment with the following parameters: wavelength 1064 nm, pulse duration 20 msec, spot size 4–6 mm, and fluence 200–250 J/cm2. The sessions were conducted at 4-week intervals.
Ten to 20 min before laser treatment, infiltration anesthesia was administered to achieve pain-free treatment, with lidocaine plus adrenalin in nonacral areas and pure lidocaine in acral areas. Warts were cleaned with alcohol and were not pared before treatment. Instead they were covered with a thin film of a moisturizing cream (water/oil or oil/water emulsion), applied manually with the tip of a cotton swab, to prevent fume development and enhance laser penetration to the deepest layers of the warts. Sufficient amounts of the cream were reapplied during the procedure.
During each laser session, one or multiple courses of slightly overlapping laser pulses were applied to each wart, covering the wart itself and a 1-mm margin on the surrounding skin. This margin is important because HPV DNA has been observed in clinically and histologically normal skin and mucosa. 10 The treatment was stopped when graying of the wart and a 1- to 2-mm margin of normal-appearing tissue was observed.
After the first session, patients were advised to apply fusidic acid cream over the treated areas thrice daily to prevent secondary bacterial infections. 11 A hemorrhagic bulla often developed at the site of laser treatment, which was punctured to relieve discomfort. The resulting hemorrhagic crust that developed over the subsequent few days was shed after 4–8 weeks, depending on the thickness of the treated skin. After another 2–4 weeks, complete scar-free healing was achieved.
Follow-up protocol
Treatment outcome was monitored by comparing color digital photographs taken before and immediately after each treatment and 1, 4, and 16 weeks after the last treatment. The occurrence of complications was also recorded during follow-up visits. Clearance was defined as the complete absence of a clinically apparent wart, along with the presence of normal skin and dermatoglyphics, and treatment failure was defined as a persistent lesion after three treatments.
Statistical analysis
Data were analyzed using SPSS software version 19.
Results
Overall, 97% of 240 patients achieved complete clearance of all warts, with 90% of patients cured after one session, 4% after two sessions, and 3% after three sessions (Fig. 1, Table 1). The average number of sessions required was 1.3 (range, 1–3), and 75.8% of patients only required a single laser session.
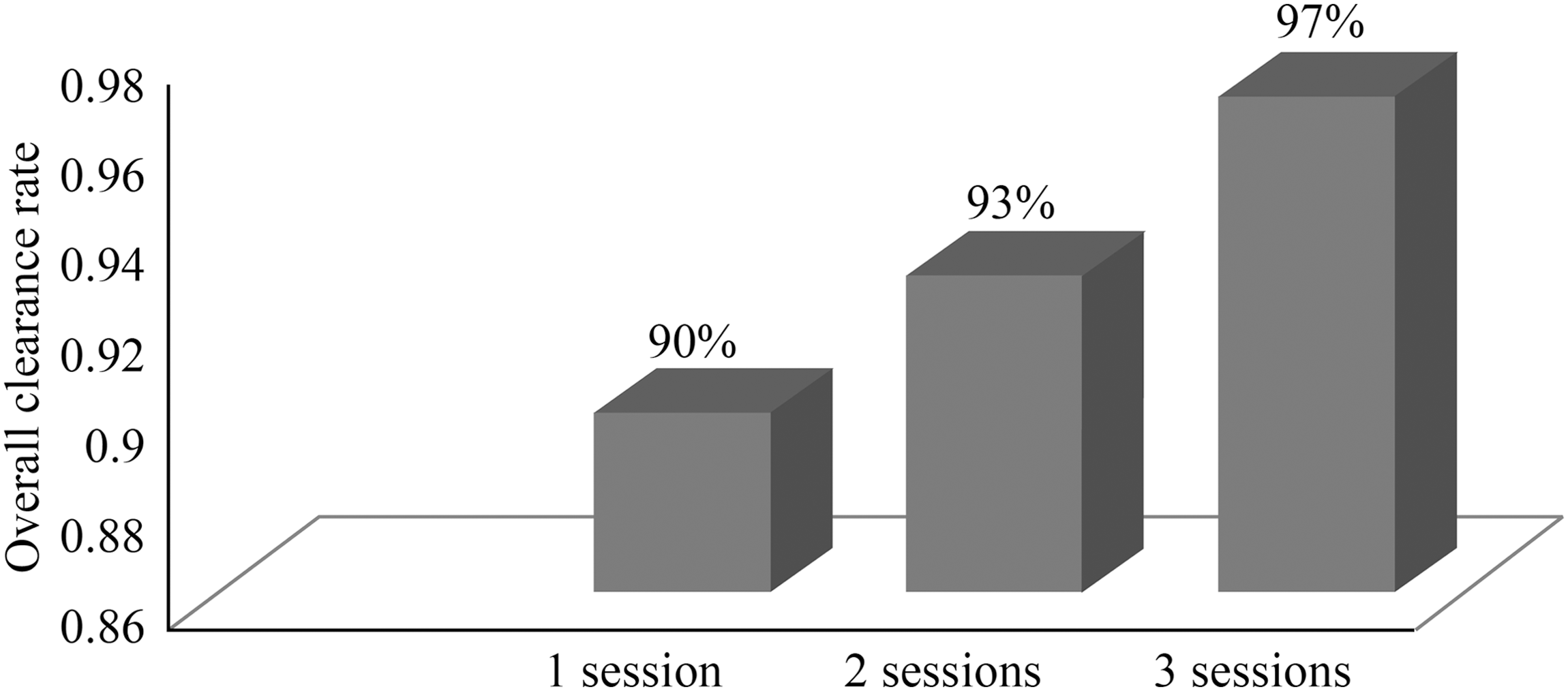
The overall wart clearance rate in relation to the number of treatment sessions.
The clearance rate after three laser sessions decreased linearly with the number of warts (Fig. 2, Table 1). In addition, the smaller the diameter of warts, the higher the clearance rate achieved (Fig. 3, Table 2). The location of warts also influenced treatment outcome. Warts located in the interdigital spaces were particularly difficult to eradicate due to their lower accessibility (Fig. 4, Table 3). Palmoplantar warts also became more difficult to eradicate as they aged (Fig. 5, Table 4).
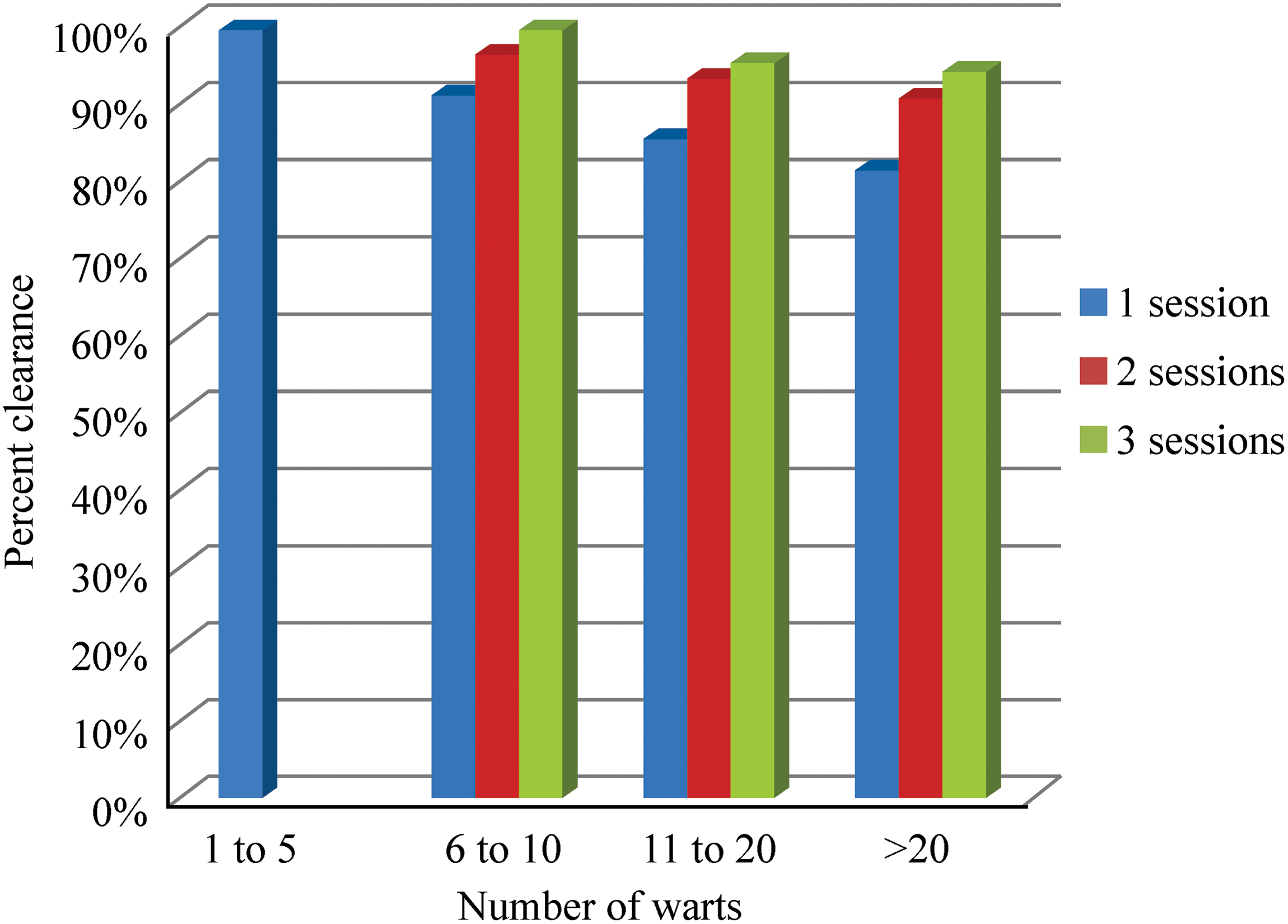
The impact of the number of warts on treatment outcome.
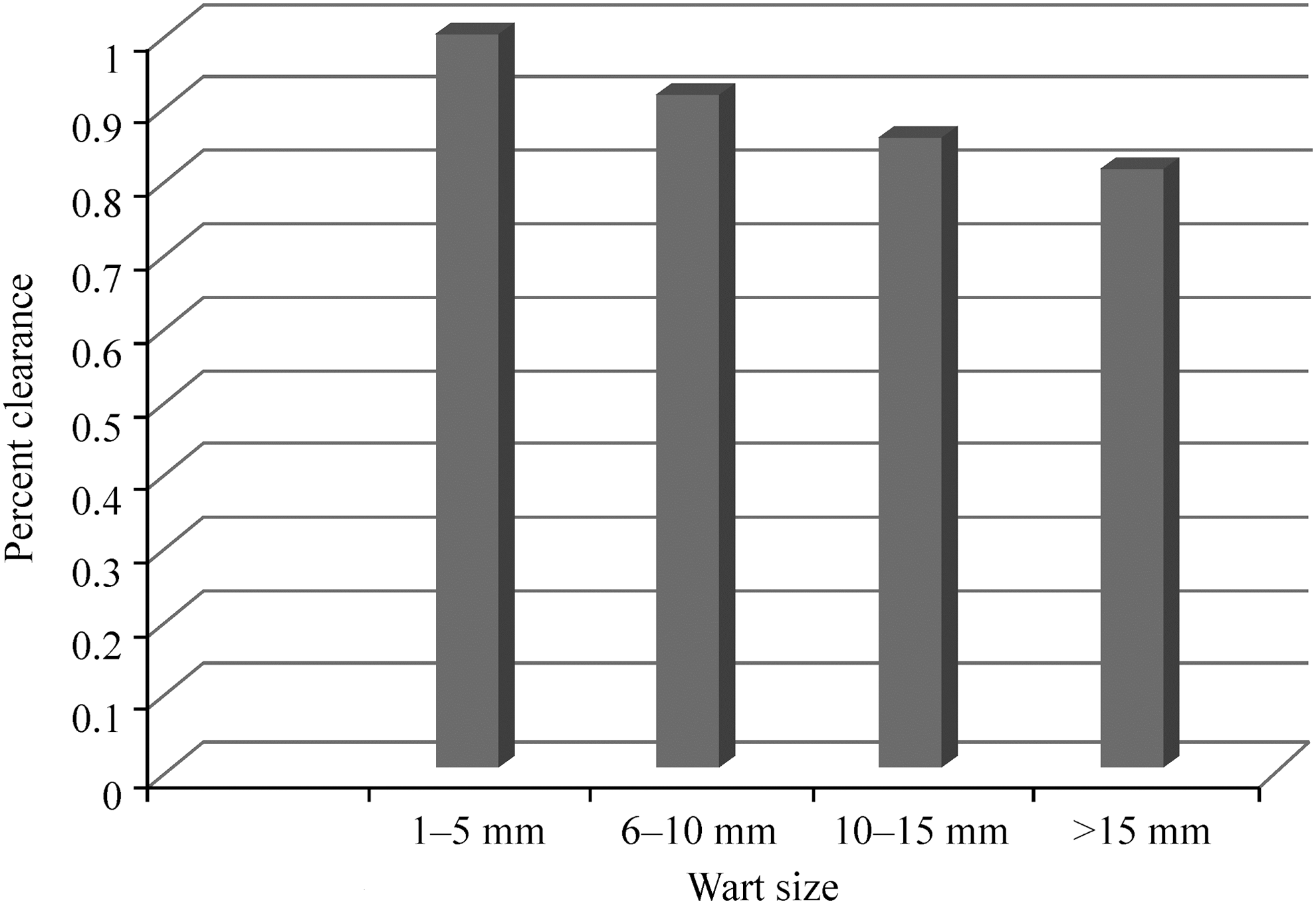
The impact of wart size on treatment outcome.
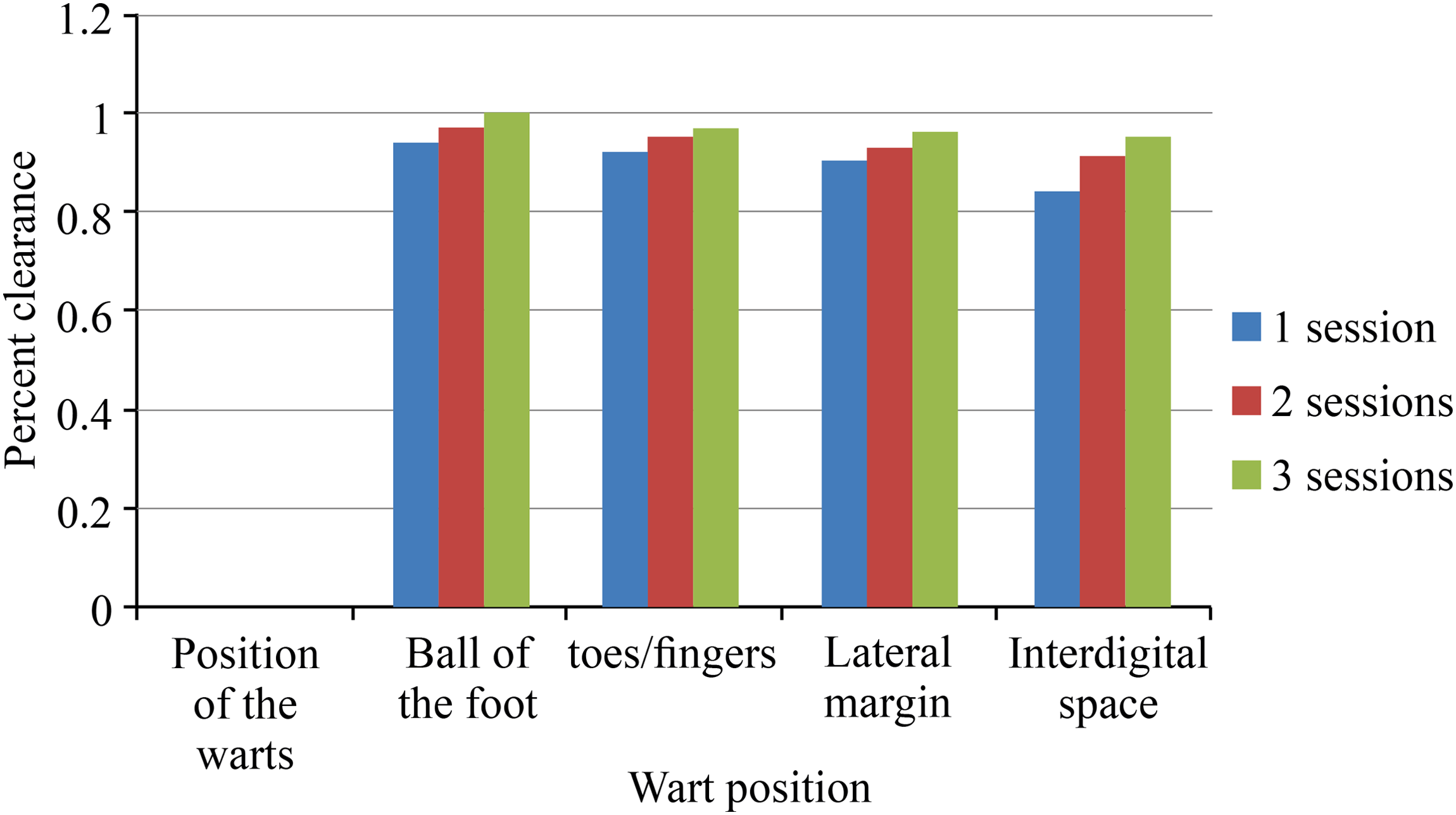
The impact of wart location on treatment outcome.
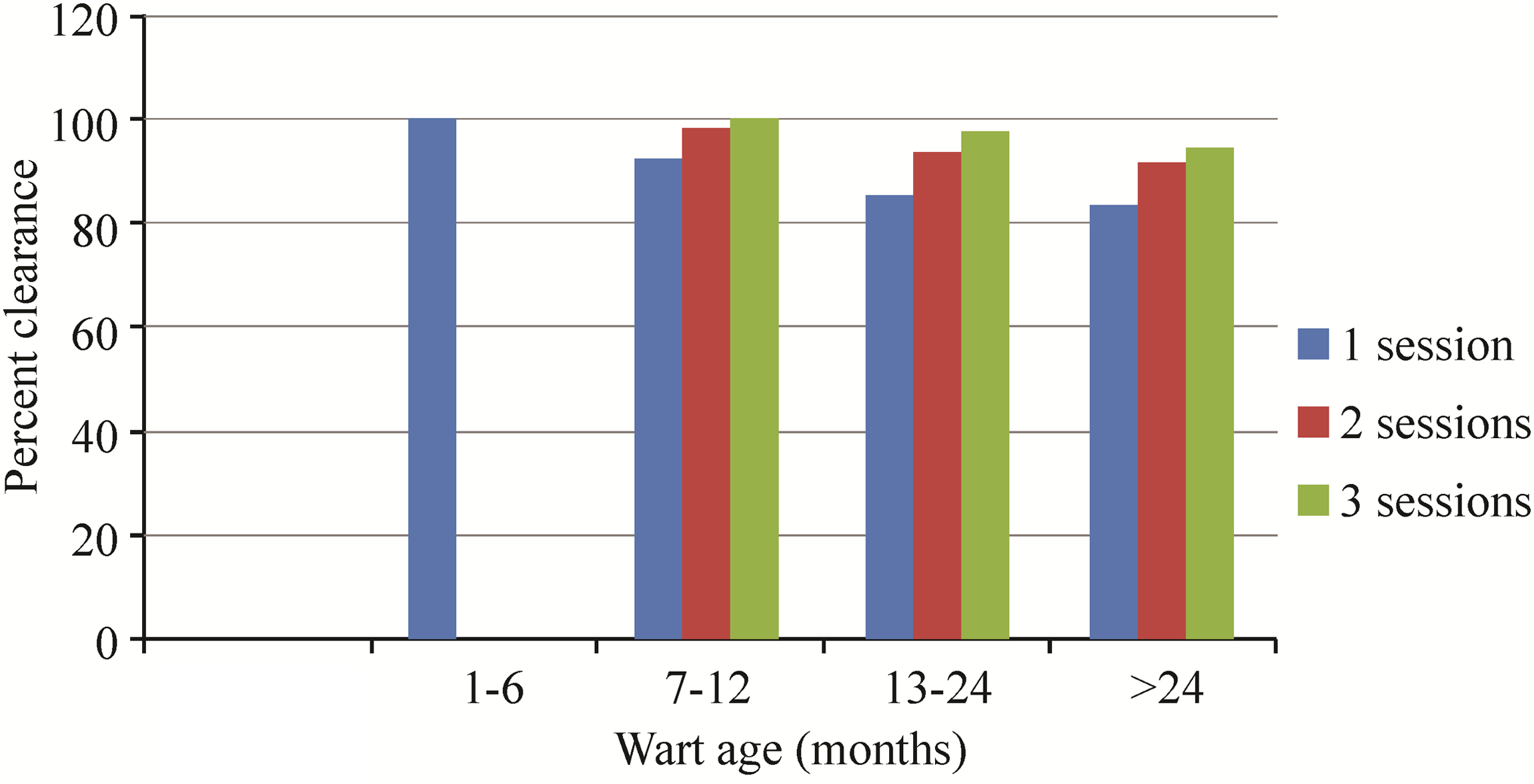
The impact of wart age on treatment outcome.
The typical evolution of the skin appearance is presented for three cases (Figs. 6 and 7). Complications were infrequent (17.5%) and mild, namely postinflammatory hyperpigmentation (5%), secondary bacterial infection (10%), and mild scarring (2.5%). Follow-up ranged from 4 months to 7 years (Table 5). Remission lasted more than 6 years in some patients. Recurrence was observed in 10% of patients within the 4-month follow-up period and this was more common among patients who had many lesions or persistent lesions or lesions located in interdigital spaces.

Perioperative progress of laser treatment of palmoplantar warts in a 20-year-old male and 23-year-old female patient.

The progress of laser treatment of plantar warts in a 25-year-old male patient.
Discussion
Laser treatment is based on the theory of selective photothermolysis, which states that specific structures of the skin preferentially absorb specific wavelengths. 4 The laser energy is then converted to heat energy, resulting in destruction of the target tissue. Known targets in the skin are water, melanin, and hemoglobin. 4 The selectivity of lasers is advantageous by decreasing surrounding tissue damage due to collateral thermal damage compared with other methods.
In the past decades, many types of lasers have been employed in wart removal. The first was the CO2 laser, which leads to vaporization of the wart, but has been associated with scarring. Further, HPV particles were identified within the smoke produced by this type of laser. 5 –7 The more precise, ablative Er:YAG laser has also been assessed for this indication, with a similar, but milder, profile of complications. 12 –15 Both CO2 and Er:YAG lasers target water in the wart tissue. More recently, the PDL has been used for wart removal by targeting hemoglobin within the dilated blood vessels of warts. 3,16,17
A 1991 study reported the therapeutic potential of the long-pulsed 1064-nm Nd:YAG laser in treating genital warts. 18 Evidence of the efficacy of Nd:YAG hyperthermia to remove recalcitrant plantar warts has also been demonstrated. 19,20 The long-pulsed Nd:YAG laser has similar properties to the PDL, in that it is absorbed by hemoglobin to some extent, and to the CO2 laser, in that it is partially nonselective, meaning that it can be absorbed by many tissue contents, including water and connective tissue. This property makes the Nd:YAG laser attractive for treating palmoplantar warts due to its deep tissue penetration. 21 –25
Plantar warts have an irregular dry surface, which leads to scattering of laser energy and decreases the amount of absorbed laser energy, thus previous studies with long-pulsed Nd:YAG laser have pared the surface of warts before laser treatment. 8 On the other hand, previous studies of the optical properties of psoriatic skin have provided evidence that application of a lipophilic liquid can maximize the selective penetration of all optical wavelengths into psoriatic skin, which decreases regular reflectance, as the cream provides a better match of refractive index between the layers of the skin. 9 Since there is great similarity between the histology of psoriasis and warts, we hypothesized that application of a moisturizing cream on the wart's surface will decrease reflectance and increase penetration of the laser into the deep wart tissue.
The present study was conducted to assess the efficacy and safety of a novel application of long-pulsed Nd:YAG laser for the treatment of deep palmoplantar warts. Our method is unique, in that the warts are not pared before treatment, as described in the study published by Han et al., 8 which is advantageous for the prevention of fume development, which is a risk factor for viral spread, as well as saving time, and decreasing the risk of injury to both the patient and the treating dermatologist. This novel method consists of covering the wart surface with a thin film of a moisturizing cream, which helps to prevent fume development and to deliver the laser energy to the deepest parts of the warts by decreasing the amount of scattered and reflected laser energy. Plantar warts have an irregular dry surface, which leads to scattering of laser energy and decreases the amount of absorbed laser energy. The surface of the warts after applying the moisturizing cream is smooth, which increases the amount of energy absorbed by the wart tissue. In addition, the cream melts immediately after the first laser pulse and diffuses between the dry keratinocytes, hydrating them and further increasing laser energy penetration. After completing the procedure, the patients were also advised to apply fusidic acid cream over the treated areas thrice per day to prevent secondary bacterial infections.
A clearance rate of up to 97% was achieved, depending on the diameter, age, site, and number of warts. Compared with the study published by Han et al., which included 348 patients, 68 with palmoplantar warts, and reported a cure rate of 88.3% for palmoplantar warts after a total of four sessions, 8 our results are superior, with a 97% cure rate after three sessions. The larger the number of warts, the greater their size, and the longer their duration, the lower our observed cure rates. These effects can be explained by low immunity against HPV, which is necessary for HPV clearance. Warts located in interdigital spaces were also associated with lower cure rates because they were difficult to access with the laser head. This result was not seen in the study conducted by Jain et al., using PDL to treat plantar warts, who found no difference in cure rates according to wart localization. 17 Notably, uncontrolled studies have suggested clearance rates of 70–90% with PDL, with plantar warts showing the lowest response to this treatment. 16 Regarding the efficacy of CO2 laser, two case series reported cure rates of 64% and 71% at 12 months, which is far less than ours (97%).Additionally, no randomized controlled trials have been published on the efficacy of the CO2 laser for palmoplantar wart ablation.
The total healing time of our patients (4–8 weeks) was considerably longer than that reported by Han et al. (1–2 weeks) using long-pulsed Nd:YAG laser without cream. 8 This difference can be partially explained by the thickness of the treated skin area. However, we observed side effects in only 17.5% of patients, which were limited to temporary postinflammatory hyperpigmentation (5%), secondary bacterial infection (10%), and mild scarring (2.5%) (Table 5). This observed 10% incidence of postoperative infection results from the treated areas being the hands and feet, which patients use for performing their daily activities. Notably, many patients in this study were housewives or farmers, who could not stop their daily activities for time to permit healing. Therefore, this rate of infection is acceptable. By contrast, Han et al. reported side effects in 31% of patients, including transient numbness (15%), hemorrhagic bullae (7%), hyperpigmentation (5%), and hypopigmentation (4%). These data suggest that the moisturizing cream protected the skin from severe side effects caused by the long-pulsed Nd:YAG laser. Kimura et al. treated 20 patients (11 males, 9 females) with a total of 34 palmoplantar and periungual warts using a long-pulsed Nd:YAG laser (spot size 5 mm, pulse duration 15 msec, and fluence 150–185 J/cm2) and reported a 56% cure rate after up to six laser sessions administered 4 weeks apart. No scarring, postinflammatory hyperpigmentation, or serious side effects were observed. 22
El-Mohamady et al. compared Nd:YAG with PDL for the treatment of plantar warts in 46 patients with multiple warts. One-half of the warts in each patient were treated with Nd:YAG (spot size 7 mm, pulse duration 20 msec, fluence 100 J/cm2) and the other half with PDL. The cure rate was 73.9% in the PDL group and 78.3% in the Nd:YAG group after a maximum of six sessions delivered at 2-week intervals. The Nd:YAG and PDL groups had complication rates of 43.5% and 8.7% and relapse rates of 8.7% and 13%, respectively. 25 Bingol et al. described the overlapped triple circle pulse technique with Nd:YAG laser (spot size 3 mm, pulse duration 23 msec, fluence 180–200 J/cm2) for the treatment of 146 refractory hand warts in 51 patients and achieved a 100% cure rate after a maximum of two sessions. The treated warts were aligned at the intersection point of the circles of three laser pulses at each session. Low rates of mild scarring (11.64%) and hyperpigmentation (5.48%) were observed, and no recurrence was reported in the 1-year follow-up period. 23 Goldberg et al. assessed the effectiveness and safety of a novel 100-msec pulsed, 200-mJ,1064-nm Nd:YAG laser for the treatment of 63 verruca vulgaris in 25 adults and observed a complete response in 19 subjects and 41 verrucae (76%) after a maximum of three treatments administered at monthly intervals, with no adverse events noted. 24 Compared with these previous reports, our study is the largest, including 240 subjects with a total of 2929 palmoplantar warts (1088 in females and 1841 in males).
One limitation of this study is that it did not compare the efficacy of the long-pulsed 1064-nm Nd:YAG laser with and without the moisturizing cream on the same patients. Future studies should compare both methods on the same patient to better control for interpatient variability.
Conclusions
The present study provides evidence that the application of a moisturizing cream before long-pulsed 1064 nm Nd-YAG laser treatment considerably reduces time required for wart removal, reduces side effects without affecting efficacy, reduces the risk of injury to both patient and physician, and prevents the development of noxious and infectious fumes affecting both the patient and practitioner.
Footnotes
Author Disclosure Statement
No competing financial interests exist.