
Abstract
Introduction
A
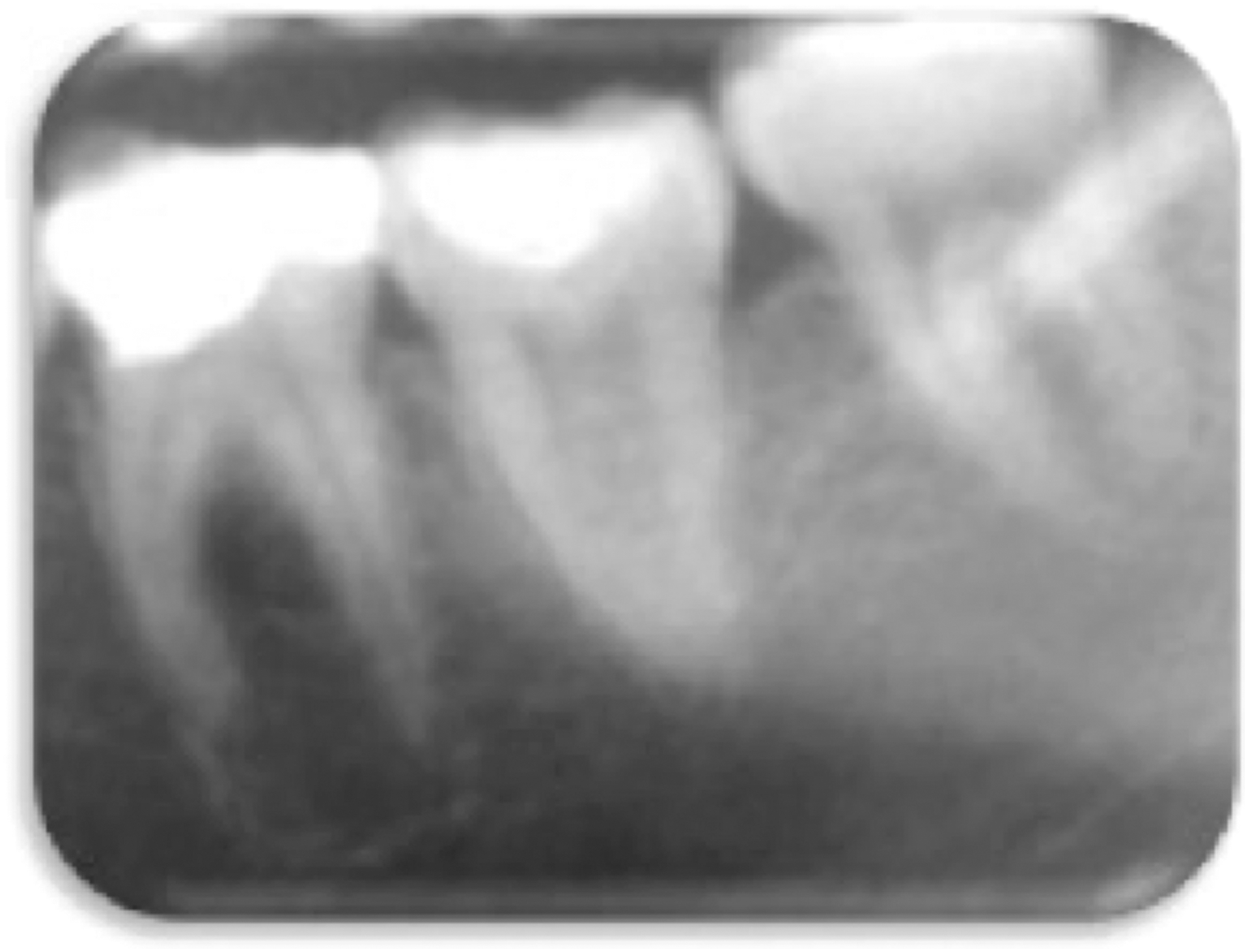
Initial aspect of the tooth 3.6 with AP and a radiopaque rim lining the lesion (notice the round, unilocular radiolucent area and the resorption of the apical third of mesial roots) compatible with the diagnosis of an apical cyst.

Clinical aspect of the autogenous transplanted tooth after 6 months (notice the edema at the buccal side).
For RCT, both sodium hypochlorite (NaOCl) and calcium hydroxide (CH) can arguably be considered the mostly used endodontic disinfectant agents. However, the extent of their clinical effectiveness remains unclear. 9 –13 Moreover, there is still no technique able to fully render the canal system free of smear layer (SL) and debris as often preconized. 14 –17 Therefore, alternative strategies (e.g., ozone, ultrasonic, lasers) have been purposed to overcome such limitation. 18 –20
Each laser wavelength has a specific absorption coefficient for each tissue component. 21 The rationale for adopting the 2780 nm (Er,Cr:YSGG) laser in endodontics may be briefly described as (1) the interaction with aqueous solutions produces cavitation effects that were shown to be capable to remove the smear layer and debris from the root canal walls 22 –24 and (2) the ability to propagate into the dentin, achieving high bactericidal effects deeper than any endodontic solution. 25,26 In addition, the development of radial firing tips (RFTs) has overcome the limitations of plain fiber tips, favoring a homogeneous energy distribution along the root canal wall. 25,27 –31
Despite several in vitro investigations having been reported, only few clinical evidences have actually shown the potential benefits of using RFTs and Er,Cr:YSGG laser for RCT. 32,33 As few studies have reported alternative strategies for endodontic disinfection of autogenous transplanted teeth, 34 this case report may be considered useful to support a new laser-assisted endodontic concept. 35 The aim is to present the clinical outcome of a laser-assisted endodontic treatment using RFTs in a nonvital autogenously transplanted third molar associated with AP.
Case Report
A 23-year-old male presented an asymptomatic carious lesion in the tooth 3.6, being clinically and radiographically diagnosed as pulp necrosis with extensive AP (Fig. 1). The patient's medical history was not contributory and autogenous transplantation was chosen as preferred treatment plan.
Under local anesthesia, the extraction of tooth 3.6 was performed with cautious preservation of the alveolar surrounding structures. The intra-alveolar septum was trimmed with a bone gauge forceps and the socket rinsed with physiologic solution. The third molar (3.8) was extracted and stored accordingly to Raghoebar et al. 36 After transplantation into the 3.6 socket, the papillae were sutured (4/0 supramid; B. Braun), passing over the crown to immobilize it.
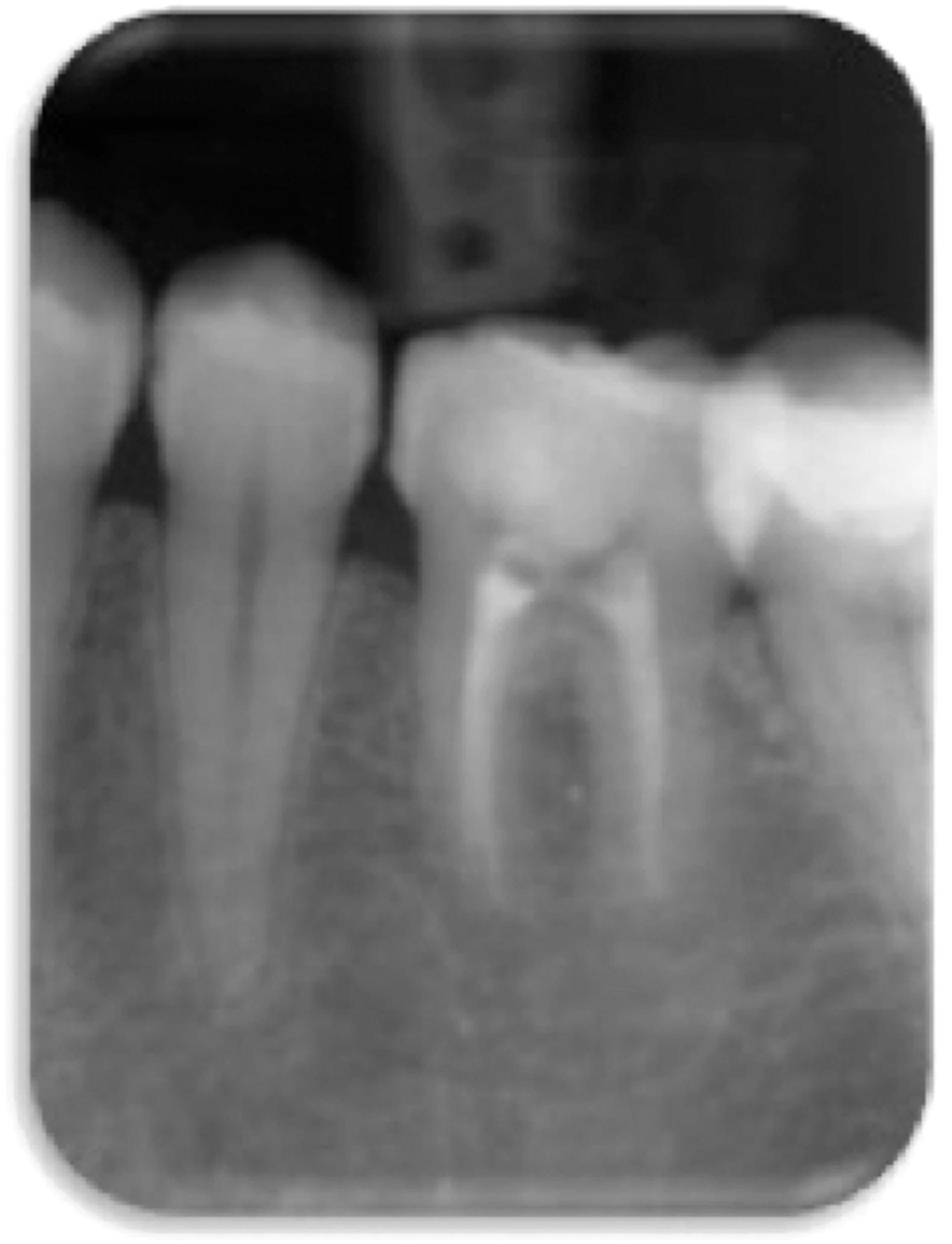
The patient only returned after 6 months with symptoms of masticatory discomfort, tenderness to percussion, transitory swelling, and negative response to thermal tests. After performing the radiographic examination, the initial diagnosis of AP was confirmed (Fig. 2).
Ethical approval for the endodontic clinical protocol (N_682/068) was obtained and the required consent (Helsinki Declaration, revised in Edinburgh [2000]) was acquired.
Under local anesthesia (2% lidocaíne with 1:100.000 epinephrine, Scandonest, France) and rubber dam isolation (Hygenic Colte`ne/Whaledent), the access cavity was prepared (Zekrya; Dentsply).
The working length (WL) was electronically established (ProPex II; Dentsply) 1 mm short of the biological apex of the root. Patency was confirmed with an ISO#10 K-file and canal preparation was performed with Protaper (Maillefer) sequence up to F3 (#30.09) and F4 (#40.06) files in mesial and distal canals, respectively.
Irrigation was performed between each file with 3 mL of saline solution (Monoject 27G; Kendall-Covidien). No chemical irrigants or interappointment medications were used.
Following preparation, the SL removal and disinfection of the root canal system were performed with the Er,Cr:YSGG laser using RFTs. 32,33 Laser irradiation was performed with a 270 μm tip (RFT2; Biolase; calibration factor of 0.55) with panel settings of 0.75W (37.5 mJ pulse energy), pulse rate 20 Hz, pulse duration 140 μs, 0% water, and 0% air. The tip was placed 1 mm short of the WL and irradiation was performed approximately at the speed of 2 mm·sec−1, withdrawing in coronal direction (Fig. 3). The irradiation procedure was repeated four times: 2 × with the canal filled with distilled water, followed by 2 × in dry conditions, resting 15 sec between each irradiation. The access cavity was left with a sterile cotton pellet and temporarily sealed (IRM; Dentsply).

Er,Cr-YSGG laser irradiation using RFT2.
At the second appointment (after 1 week), there was a negative history on questioning to pain, tenderness to percussion, or swelling. Under rubber dam isolation, the canals were once again filled with distilled water, and laser irradiation was performed with a 320 μm tip (RFT3, Biolase, USA; calibration factor of 0.85) with panel settings of 1.25 W (62.5 mJ pulse energy), pulse rate 20 Hz, pulse duration 140 μs, and 0% water and air. The irradiation movements and repetitions were identical to the first appointment.
A final rinsing with saline solution (3.0 mL) was performed, and the canal was dried with sterile paper points, checking for the absence of exudate. Filling was performed with tapered gutta-percha (2xF3 and 1xF4) adopting an autofitting technique, vertical compaction, and an epoxy resin-based sealer (TopSeal; Dentsply) (Figs. 4 and 5).

Radiographic assessment of gutta-percha fitting.

Immediate radiographic assessment following laser-assisted endodontic treatment.
Radiographic controls and clinical records were recorded after 6 months (Fig. 6), 1 year (Fig. 7), 2 years (Fig. 8), and 3 years (Figs. 9 and 10). Over this follow-up period, the tooth remained completely asymptomatic and periapical healing could be noticed.

Six months' follow-up.

12 months' follow-up.
Two years' follow-up.

Three years' follow-up (notice the complete reestablishment of the periodontal ligament).

Three years' follow-up panoramic radiography.
Discussion
Data provided by radiographic means can only provide a moderately accurate diagnosis to distinguish between AP and radicular cyst. 37,38 However, the compromised clinical status of the tooth 3.6 justified the extraction along with excision of the lesion content (Fig. 1).
Given that tooth transplantation is considered a predictable treatment option, wisdom teeth often represent the best donor alternative. 2,39 This report may confirm such statements, along with the viability of a single-appointment surgical approach 39,40 and the importance of endodontic treatments, to predict successful outcomes. 6,41
In teeth with complete root formation, the small size of the apical foramen can play a role by delaying bacterial contamination during the surgical procedure. 42 Nevertheless, to prevent pulp necrosis and inflammatory reactions, the RCT of transplanted mature teeth is preconized between 7 and 14 days following surgery or performed as soon as the peridontal ligament (PDL) is restored. 3,6
As our report may confirm, 6 months after transplantation, severe inflammatory reactions could be noticed, surpassing all recommended periods to perform the RCT. 4 This may also highlight the importance of patient compliance with the pre-established protocol. 6
Ankylosis and root resorptions are often reported as consequences of tooth transplantation. 43,44 In this clinical case, the apical resorption of the distal root can be related to the breakage of vascular supply and to the AP chronic nature (Fig. 5). 3,8,45
Despite several reports of distinct surgical techniques, there are still no guidelines for endodontic management (i.e., disinfection) of transplanted mature teeth. Therefore, this report may be of special relevance while adequately reporting a new disinfection technique and its clinical outcome. 35,46 The adoption of laser-assisted disinfection protocol was based on the assumption that (1) third molars often present intricate root canal anatomies where irrigants cannot penetrate effectively and (2) the apical resorption at the distal root could be seen as a predisposal factor for the occurrence of an iatrogenic accident. 47
The high absorption coefficients of the 2780 nm wavelength in both water and hydroxyapatite justify the selection of this wavelength for both SL removal and disinfection. 48 In fact, it is known that the interaction between this laser wavelength and aqueous solutions induces both primary and secondary cavitation effects that are able to remove debris and SL from the root canal system. 22,49 Previous studies inclusively found that the Er,Cr:YSGG laser could be more efficient than EDTA irrigation or passive ultrasonic irrigation, while minimizing the risk of any irrigant extrusion. 27,49 –52 However, to exhibit its maximum bactericidal properties, Er,Cr:YSGG laser irradiation should be performed in dry conditions, allowing the energy to be transmitted through the dentinal tubules 25 and instantaneously interact with the water inside bacterial membranes, as well as the water trapped within endodontic biofilms. 53
However, in vitro studies often provide confounding evidences regarding laser settings and, due to standardization demands, do not take into account relevant clinical factors. Therefore, the laser settings used in this clinical case were based on a previously reported clinical trial. 31,33 The protocol consists of two irradiations with distilled water in the main canal for debris and SL removal, followed by two other irradiations—in dry conditions—to achieve higher dentin disinfection depth.
The present protocol is in contrast with the one reported by Christo et al. that attempted to use the Er,Cr:YSGG laser for NaOCl activation, but did not show any bactericidal improvements. 54 Moreover, it is known that the activation of chemical irrigants by erbium lasers with relatively high output powers may eventually induce their apical extrusion. 55
Independently of the wavelength, laser bare fibers have been used since many years for endodontic purposes. These fibers are required to be inserted in the main canal and withdrawn from apical to coronal region in a rotating motion to overcome their relatively small beam divergence. 56 Despite their relative success, such technique is known to be operator sensitive and to produce inconsistent results. 48,57,58 In contrast, RFTs can spread laser energy toward the direction of dentinal tubules and were shown to increase cavitation effects toward the root canal walls without being hazardous to the periapical tissues. 25,27 Moreover, they were shown to produce clinically safer temperature increments with complete absence of molecular dentine changes 28 –31 and to be highly efficient in biofilm disaggregation. 53,59 RFTs also demonstrate the potential to overcome the airlock effect, allowing irrigant solutions to safely reach the apical third. 60
Despite the absence of a cone beam computed tomography (CBCT) assessment to further validate the outcome of this report, 61 it is still debatable whether such tridimensional techniques overestimate periapical images or if they are even able to identify various forms of periapical bone tissue changes. 62
The present clinical findings are in agreement with the majority of in vitro studies that demonstrate the capability of the Er,Cr:YSGG laser to remove SL and to provide a uniform deep disinfection of the entire root canal system. 25,31,50 This report may also attest the effectiveness, safety, and clinical outcomes reported for single-rooted teeth. 33
Conclusions
After 3-years of follow-up and, despite the intrinsic limitations of a single-case report, our findings may attest that RFTs can be considered for the endodontic treatment of multi-rooted teeth associated with AP, inclusively in autogenous transplanted teeth. Further randomized clinical trials should be conducted to clearly demonstrate its effectiveness.
Footnotes
Acknowledgments
The authors thank the AALZ—Aachen Dental Laser Centre (Germany) for their support and encouragement.
Author Disclosure Statement
No competing financial interests exist.