
Abstract
Introduction
O
Many studies have researched different methods to reduce the relapse of orthodontically rotated teeth, including gingival injection of relaxin, 1 circumferential supracrestal fiberotomy (CSF), 2 –7 laser-aided CSF, 8,9 gingivectomy, 10 overcorrection, prolonging the use of retention appliances for a considerable period of time, 11 reproximation, 5,6 and early correction during the eruption of tooth. 12 These methods could truly decrease the risk of relapse, but they have some drawbacks; for example, they might cause some pain and discomfort to the patients, or surgical procedures used to reduce the relapse might have negative effects on periodontal tissues.
Compared to the aforementioned methods, low-level laser therapy (LLLT) has not reported negative systematic effects on human beings yet. Since its first introduction into clinical medicine in 1968, 13 there are lots of published data on the use of LLLT because of its noninvasive manner and biostimulatory effect on tissues without increasing the temperature of treated region above the normal body temperature. This technology is also widely used in stomatology, such as enhancement of the stability of orthodontic mini-implants, 14 reducing pain and inconvenience for patients with orthodontic adjustment 15,16 or recurrent aphthous stomatitis, 17 prevention of dental caries, 18 improvement of enamel surface microhardness around orthodontic brackets, 19 relieving dentine hypersensitivity, 20 accelerating tooth movement during orthodontic treatment, 21 and so on.
Researches have been conducted to confirm the effectiveness of LLLT on the relapse of rotational teeth, including animal models and human subjects. Therefore, a systematic review of available knowledge is in need to comprehensively evaluate the influence of LLLT on the relapse of orthodontically rotated tooth.
Materials and Methods
This systematic review was carried out and reported in accordance with Cochrane Handbook for Systematic Review of Interventions and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Two reviewers independently conducted search and the work of extracting data, and assessed the risk of bias and eligibilities of the retrieved articles. Any disagreement was resolved by discussing with a third reviewer.
Search strategy
The following databases were searched: PubMed, MEDLINE (via OVID), EMBASE, Web of Science, website of Cochrane Central Register of Controlled Trials (CENTRAL), and ProQuest Research Library (PRL). Ongoing clinical trials were searched in World Health Organization International Clinical Trials Registry Platform (WHO ICTRP). Terms used in the search included “laser therapy, low-level/laser therapy/laser irradiation/laser,” “orthodontics/orthodontic,” “relapse.” Specifically, the electronic searching was conducted up to November 2015 with no language restriction. Table 1 shows strategies used in the data search process. This process was conducted independently and in duplicate by two reviewer authors.
Inclusion criteria
Types of studies
We included studies that estimated the efficacy of LLLT on the relapse of orthodontically rotated tooth. The study design should be randomized controlled trials (RCTs), quasi-RCTs, or controlled clinical trials (CCTs).
Types of experimental subjects
Subjects included in this review could be animals or human beings. For the former, experimenters should comply with the principles of animal rights defined by authorities. For the latter, the studies should have been approved by the appropriate research ethics committee. Moreover, the participants should have no systematic diseases, should have exhibited good oral hygiene, and should have agreed to attend this research.
Exclusion criteria
Types of studies
Reviews, case reports, cohort studies, descriptive studies, letters, opinion articles, and abstracts are excluded.
Types of experimental subjects
Patients with gingival or periodontal problems and those who consumed medicine that interrupted bone metabolism are excluded.
Study inclusion
Two reviewers independently conducted the search, reviewed the titles and abstracts, and went over the full text when information given by the abstracts was insufficient to judge whether the articles met the inclusion criteria or not. Also, they discussed with a third reviewer when there was a disagreement.
Assessment of risk of bias
Risk of bias assessment was undertaken according to Cochrane Handbook for Systematic Reviews of Interventions. The features of interest in the standard “Risk of bias” table of Cochrane review were as follows: sequence generation (selection bias), allocation sequence concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective outcome (reporting bias), and other potential sources of bias. Each entry of these features addressed a specific feature of the included studies. The judgment for each entry involves assessing the risk of bias as “low risk,” as “high risk,” or as “unclear risk,” with the last category indicating either lack of information or uncertainty over the potential for bias.
Data extraction
Basic data of the included studies were extracted and recorded independently and in duplicate by two review authors, including study design, participant information, methods used to rotate the teeth, interventions for each group, time for rotation and follow-up, retention or not, means to measure tooth movement, and the final conclusions. Meanwhile, the parameters of LLLT were recorded in the same way, including type of laser, wavelength, energy density, power output, energy during each irradiation session, spot area, spot size, and frequency of laser treatment. Further, the degree of initial rotation and relapse, and percentage of relapse were also extracted. Last, information relating to feasible adverse effects caused by LLLT on experimental subjects and histologic examination was also extracted.
Results
Search results
A total of 112 studies were collected following the search strategies mentioned earlier. After screening the titles, abstracts, and full texts when necessary, three articles met the inclusion and exclusion criteria and were brought into the systematic review. The procedures of electronic searching are presented in Fig. 1.
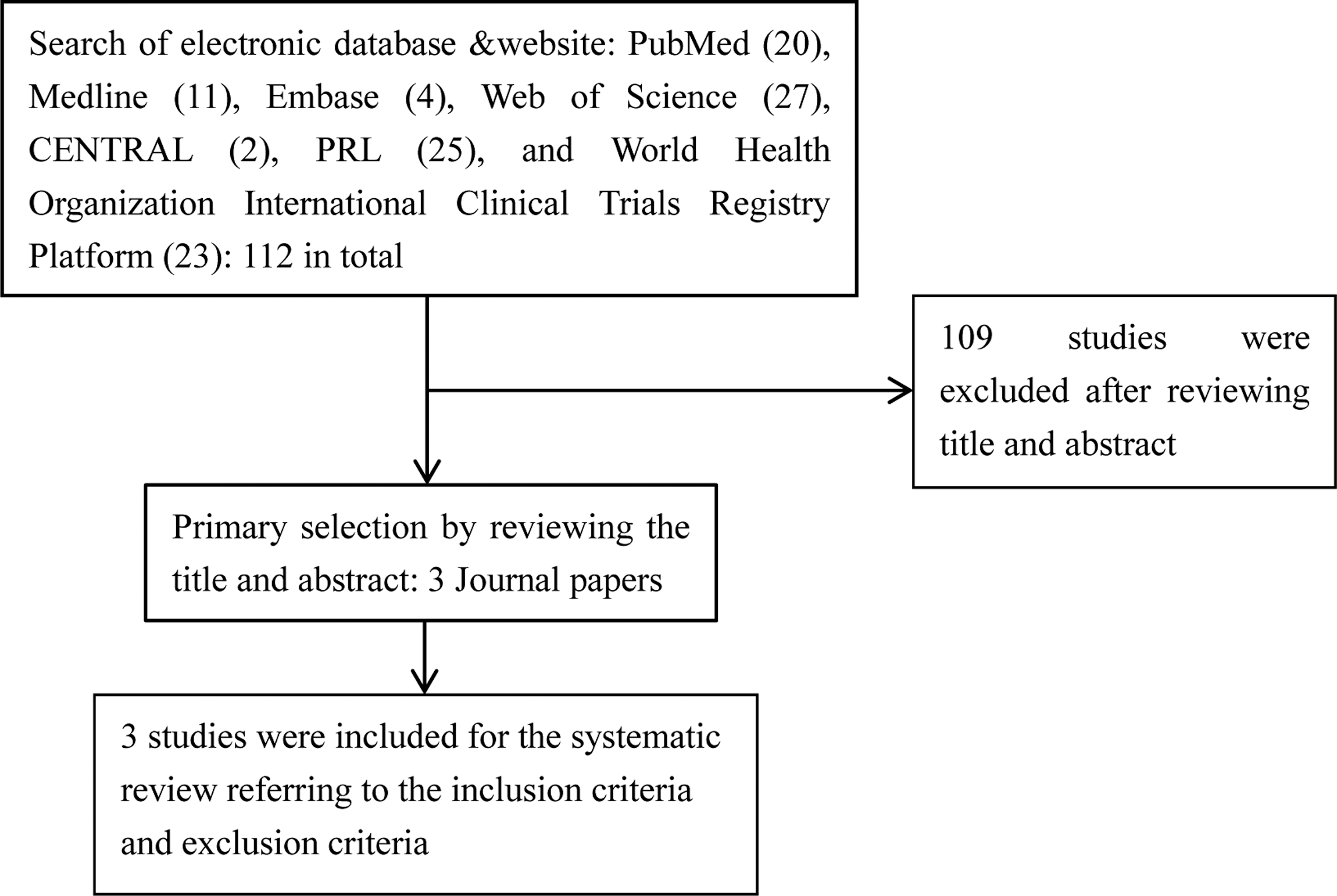
Systematic search and selection strategy (flow chart).
Characteristics of included studies
Three studies were included in this systematic review: two animal experiments, conducted on mandibular lateral incisors in beagles, and one human study that included 23 rotated maxillary incisors. Table 2 elucidates the general characteristics of the recruited studies. Meanwhile, details of laser parameters used in every study are summarized in Table 3.
C, control group; I, LLLT group; LLLT, low-level laser therapy; n, number of subjects; RCT, randomized controlled trials.
Methodological and quality assessment
Randomization was performed among all included RCTs. One animal experiment 22 used split-mouth design and took the left side as the experimental group. And no withdraws happened in the CCT. 8 Risk of bias assessment according to the Cochrane Handbook for Systematic Reviews of Interventions for each study is presented in Table 4.
+, low risk of bias; −, high risk of bias; ?, unclear risk of bias.
The effect of LLLT on relapse of orthodontically rotated teeth
Three included studies reported degree of relapse for orthodontically rotated teeth. All studies took alginate impressions, photographed original, rotational, and relapse casts, imported these images into a computer image analyzer, and measured the angles formed between the defined reference line and the incisal edge line of the experimental incisors. The percentage of relapse was the degree of relapse, divided by the total rotational movement of each tooth and multiplied by 100.
Human study
Jahanbin et al. 8 recruited 12 rotated incisors in six patients and 11 rotated incisors in six patients for the LLLT group and control group, respectively. Continuous wavelength mode (810-nm wavelength) with an energy density of 35.7 J/cm2 was applied during relapse for the LLLT group. Statistical analysis revealed that LLLT with high energy density was effective in alleviating relapse after 1 month compared to the control group.
Animal study
Twenty-eight mandibular lateral incisors in beagles were involved in the researches performed by Kim et al. 9 and Salehi et al. 22 Kim used pulsed wave with a 4.63–6.47-J/cm2 energy density and 808-nm wavelength to irradiate incisors after removing the orthodontic appliance in the LLLT group and came to the conclusion that LLLT seemed to increase the relapse tendency of orthodontically rotated teeth over a short observation time of 4 weeks. Salehi et al. irradiated the experimental teeth with continuous wavelength of 810 nm and 31.8 J/cm2 during the orthodontic movements in the LLLT group. The data analysis demonstrated that LLLT did reduce the relapse of rotational teeth, but the decreasing tendency was weakened over time since the difference between the LLLT group and control group was smaller after 3 months of observation compared to 1 month.
Adverse effect
Only one study 9 included observed the adverse effect of LLLT on periodontal tissues, in which laser-aided CSF was also conducted on other experimental teeth. Compared to laser-aided CSF group, whose pocket depth increased by 0.67 mm averagely after 1 month of relapse in contrast with the initial level, the LLLT group showed no increase of pocket depth. Although there did exist gingival swelling during rotation of the teeth due to wearing the orthodontic appliance, gingivitis subsided and the gingival height returned to its original level at the end of experiment.
Histologic examination
The study conducted by Kim et al. 9 used hematoxylin–eosin and Masson's trichrome staining to examine the tissue blocks, which were sectioned perpendicular to the long axis of the experimental teeth. Under light microscopy, the changes and thickness of the fiber bundles, as well as the phase of the blood vessels from LLLT group, were similar to those of control group.
Discussion
Rotation was quite different from the mesiodistal dental movement, and the mechanism for relapse of corrected tooth rotations to its pretreatment position has been surveyed since 1959 by Reitan, 12 who concluded that relapse of rotated tooth was caused primarily by a contraction of displaced supra-alveolar fibers. Further conclusions were drawn by Boese, 10 who divided the phases of orthodontic rotational relapse into the following two parts. (A) In the first 8 weeks, following orthodontic rotation of a tooth, relapse was mainly caused by stretched principal fibers, which could be terminated by the remodeling of alveolar bone, providing new attachments for the principal fibers. (B) After the first 8 weeks, the relapse was caused by the supra-alveolar fibers. The proliferative response of oxytalan and collagen fibers in the supra-alveolar tissue caused by orthodontic tooth rotation and the stable attachments of the trans-septal fibers seemed responsible for this part of relapse. Edwards had similar findings. 2 This result was corroborated by an in vitro study, 23 in which transcription of collagen type I was increased and collagenase was decreased under centrifugal force. However, Redlich found disorganized, split, and ripped collagen fibers and revealed an increase in elastic fibers after orthodontic rotation and retention. 24 So they assumed that the relapse might not be due to “stretched” collagen fibers, but rather originated in the changing elastic properties of the whole gingival tissue. From the aforementioned discussion, we can deduce that the relapse of rotated teeth is related to the change of collagen and elastic fibers in periodontal and gingival tissues during rotation and retention. Moreover, the mechanism of CSF in reducing the relapse of rotational teeth can be ascribed to rearrangement of collagen and elastic fibers. However, the problem that plays a more important role in the relapse of rotational tooth, collagen or elastic fibers, needs to be explored further.
Collagen and elastic fibers in gingiva and periodontal ligament (PDL) are mainly secreted by fibroblasts. Several studies in vitro have indicated that LLLT can increase fibroblast cell proliferation in gingiva 25 –27 and PDL, 28 low energy density applied in these studies. The alteration of fibroblast proliferation on circumstance of laser irradiation may change the amount of fibers in periodontal tissues, and relapse of rotational teeth further. Since these changes were observed in vitro, the influence of LLLT on the amount of fibroblasts in vivo needs deeper studies.
As to the effect of LLLT at the molecular level, relevant research has discovered that LLLT can change the protein expression in cells, not only by upregulating but also by downregulating the content of different proteins. 25 A statistically significant increase in gene expression of collagen and vascular endothelial growth factor was also found in fibroblasts under laser irradiation. 29 –31 The induction of collagen synthesis by laser irradiation may be related to activation of TGF-β/Smad signaling pathway, 30 which plays an important role in the formation of extracellular matrix.
The photobiological effect of LLLT is on the basis of its influence on cells, especially the excitation of the respiratory chain in the mitochondria in cells. Evidence shows that mitochondria are sensitive to monochromatic to near-IR radiation. 32 When irradiated in vitro at a wavelength of 660 nm and a fluence of 5 J/cm2, enzyme in fibroblast mitochondria was influenced, in particular, cytochrome c oxidase, 33 which plays a role as possible photoacceptor. This leads to a cascade of reactions, including changes of mitochondrial morphology from a filamentous to a granular appearance, more extensive distribution, 34 increased mitochondria activity and ATP synthesis, 33 inducing reactive oxygen species (ROS) generation, 35 and the mitochondrial membrane potential is strengthened. 36 These changes may promote phosphorylation of Jun N-terminal kinase (JNK)/activator protein-1 (AP-1) expressions 37 and activate the redox-sensitive NF-κB signaling pathways. 38 All these primary changes may cause a series of secondary effects, such as alteration of metabolic activity, upregulating or downregulating gene and protein expression, 39 which might contribute to the biostimulatory effects of action of LLLT.
Hu 37 irradiated melanoma cell line A2058 cells with He-Ne laser (632.8 nm), with dosages of 0.5, 1, 2 J/cm2, and found that cytochrome c oxidase activity increased by about 70%, 140%, 170% after irradiation, respectively, compared with the control group. Further, LLLT in a greater scope of energy density was applied by Sharma et al., 40 who irradiated primary mouse cortical neurons from mice with influence of 0.03, 0.3, 3, 10, or 30 J/cm2 of 810-nm laser and found an increase in calcium, ATP, and mitochondrial membrane potential at lower fluences and a decrease at higher fluences. However, the production of ROS showed a different pattern—triphasic dose–response pattern, 41 which displayed an increase at low fluences, followed by a decrease and a second larger increase at 30 J/cm2. Wu et al. 42 applied a much higher energy density 120 J/cm2 in vitro to irradiate human lung adenocarcinoma cells and African green monkey SV40-transformed kidney fibroblast cells, which showed activation of caspase-3, accompanied by an immediate increase of ROS and decrease of mitochondrial membrane potential after irradiation. A mass of ROS generation may contribute to mitochondrial pore transition. 43 These changes indicated the activation of the mitochondrial/caspase-3 pathway, which can initiate and regulate cell apoptosis. Low energy density also can cause the increase of ROS in mitochondria after irradiation, but the amount of ROS does not reach the concentration that can trigger mitochondrial pore transition. On this occasion, an involvement of ROS might not cause cell apoptosis but enhances cell migration, proliferation, and adhension. 44,45 So, this might be the reason why low energy density can promote tissue metabolism, while high energy density suppresses the activity of irradiated tissues. This phenomenon suggests that the effect of LLLT has a biphasic dose response. 46 Many researches illustrated this biphasic dose response with the Arndt Schulz model, 41,45 but we preferred that the inverted U-shaped model 47 might be more accurate to describe this relationship between energy density applied and the biological effect, as shown in Fig. 2. Point A means proper energy density that can arouse the maximal stimulatory effect, while point B implies the critical point above which LLLT will cause inhibitory effect rather than stimulatory effect. We can get a better understanding of this biphasic dose–response effect of LLLT by making connection with the triphasic dose response of ROS produced by mitochondria after irradiation. Treated by LLLT with low energy density, an increase of ROS might contribute to the stimulatory effect of LLLT. With the energy density rising, production of ROS begins to descend, and so, the stimulatory effect caused by ROS decreases, which coincides with the segment from A to B in Fig. 2. As the energy density increases further, a large amount of ROS is generated, activating the mitochondrial/caspase-3 pathway and causing an inhibitory effect on irradiated cells and tissues. This corresponds to the segment after B in Fig. 2.
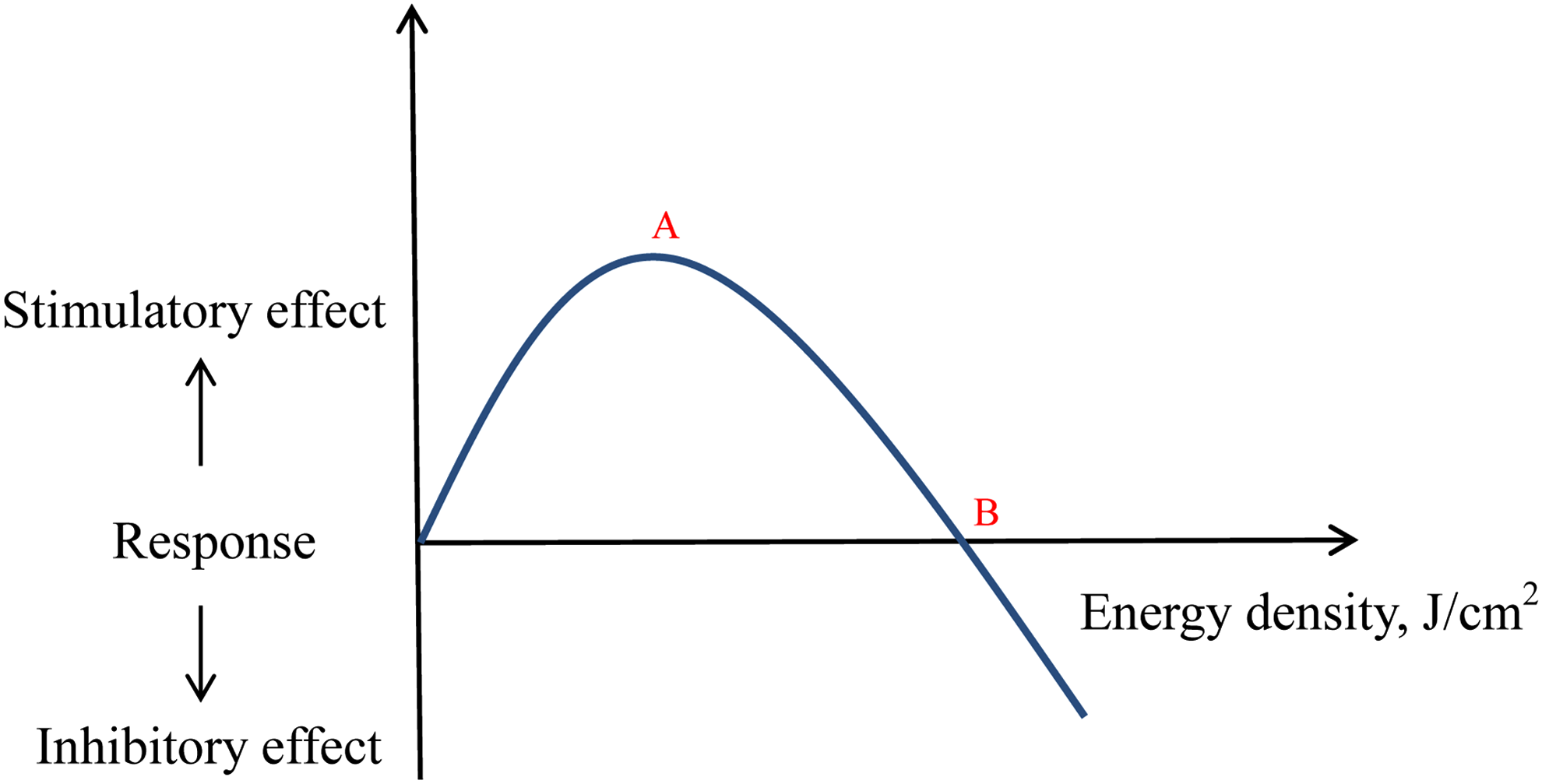
Biphasic dose response of LLLT described by the inverted U-shaped model. Point A means proper energy density that can arouse the maximal stimulatory effect, while point B implies critical point above which LLLT will cause inhibitory effect rather than stimulatory effect. LLLT, low-level laser therapy.
Studies have confirmed that the influence of laser irradiation is not only related to energy density 26,30,38,48 but also connected with wavelength, 49 cell type, 38 and treatment time. 26,28 So, under different kinds of situations (wavelength, cell type, etc.), the values of point A and point B in Fig. 2 vary a lot. Murayama 50 irradiated the glioblastoma cell with a diode laser at a wavelength of 808 nm and concluded that a relatively low energy density less than 5 J/cm2 had a stimulatory effect on proliferation of normal cells, while energy density higher than 5 J/cm2 had an inhibitory effect. This argument was not compatible with Zhang, 51 who irradiated the Hela cells with a wavelength of 608 nm and summarized that laser irradiation lower than 25 J/cm2 promoted cell viability while high dose impaired. As to point B regarding the effect of LLLT on relapse of rotational teeth in beagles, available data were insufficient to determine. Kim et al. 9 applied a diode laser with 4.63–6.47 J/cm2 energy density and under this condition, LLLT increased the relapse tendency and had a stimulatory effect. On the contrary, Salehi et al. 22 irradiated the rotational teeth with laser of 31.8 J/cm2-energy density, which alleviates the relapse of rotational teeth and had an inhibitory effect. We can presume that point B might lie between these two values. More researches are in need to ascertain point A and point B in humans for different kinds of tissues so that we can apply suitable energy density for various purposes.
Salehi et al. 22 observed that after 3 months of follow-up, the percentage of relapse was still lower than in the control group, but the degree of relapse failed to show the same results. This phenomenon suggested that the effect of LLLT on relapse of rotational tooth might change as time went by. Maybe this was also related to the fact that the maximum of relapse happened in the early time after rotation. 4 So early application of LLLT after rotation is advised to decrease its relapse.
This systematic review included two animal experiments and one human study. Only one study described methods of randomization. One animal experiment used split-mouth design, namely both experimental and control sides were in the same participant and the assignment would not change. Although the allocation was not concealed, it would not result in bias. Thus, we gave“+” in allocation concealment. All studies recruited randomly selected dental models and calculated tooth rotation for the second time, 8,22 and the correlation coefficients were 0.997 and 0.97, which implied good reliability and reproducibility of these measurements. Double determination measurements were performed by two investigators independently, 9 and so, we judged “Blinding of outcome assessment” to be “+.” Other bias in this article specialized in baseline imbalance between the LLLT and control group. Since there was no statistical significance of initial angle of rotation between the groups, we judged them to be “+” in “other bias.” In total, the quality of these three studies was high.
However, the foremost limitation in this review was that there were only three available studies, and only one was conducted on human beings. Although the arrangement of the supporting structures in man and the dog is fairly similar, the periodontal fiber bundles are coarser and the bone tissue is frequently denser in the dog than in human. 12 This confinement demonstrated disadvantage for this systematic review. In addition, there were some inconsistencies in the utilization of LLLT: Kim et al. 9 and Jahanbin et al. 8 irradiated teeth after rotation, while Salehi et al. 22 applied irradiation during rotation. This dissimilarity may cause inconformity in the results. Further, in clinical practice, patients are ordered to wear retainers after active orthodontic treatment. In these studies, however, no retainers were used, which might cause potentially different effects since Kim et al. 48 found that the influence of LLLT on relapse was disparate with or without retainers. In the future, more well-designed RCTs involving human are required to further study the effect of LLLT on the relapse of rotational teeth.
Conclusions
According to the results of our systematic review, it seems that the effect of LLLT on relapse of corrected tooth rotations is related to energy density. Taking this one step further, low energy density seems to promote relapse, while high energy density might alleviate the relapse, which implies that LLLT has a biphasic dose–response effect. Also, early application of LLLT was suggested. Since available investigations are limited, the conclusion should be interpreted with caution, and more well-designed RCTs involving human are needed to get more clinically significant conclusions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.