
Abstract
Introduction
P
Eradication of microbes is the mainstay in the management of periodontal disease, and the conventional treatment for such infections can be achieved by standard mechanical debridement such as scaling and root planing (SRP) with the adjunctive use of systemic antibiotics. 14,15 Despite microbiological improvements, antibiotics have several untoward effects in which bacterial resistance cannot be overruled. 16 SRP has some physical limitations as well, which attenuates complete elimination of calculus and bacterial deposits from deep periodontal pockets. 17,18 To overcome the limitations of scaling and root planing and to reduce the bacterial load, antimicrobial photodynamic therapy (aPDT) has been proposed as a treatment strategy for elimination of bacteria in periodontal disease. 19,20 The mechanism of action of aPDT involves three main components including light, a photosensitizer (PS), and oxygen. Upon administration of PS dye in the periodontal pocket, excitation with light of a specific wavelength leads the PS to undergo a transition from ground singlet state to a higher-energy triplet state that reacts with endogenous oxygen to produce singlet oxygen and other radical species, causing a rapid and selective destruction of the target bacterial species. 21,22
The benefits of aPDT includes further suppression of periopathogenic bacteria and risk of bacteraemia. 23,24 In a clinical trial by Moreira et al., 19 periodontitis patients treated with aPDT as an adjunct to SRP showed significant reduction in the counts of all four major periodontal pathogens (Pg, Tf, Td, and Aa) compared with those treated with SRP alone at 3-month follow-up. However, Rühling et al., 25 in a similar trial, showed comparable outcomes in the counts of periodontal pathogens treated with aPDT as an adjunct to SRP and SRP alone at 3-month follow-up. Therefore, there appears to be a controversy with regard to the bactericidal efficacy of aPDT as an adjunct to SRP in reducing the counts of periodontal pathogens in periodontal disease.
The aim of the present study was to systematically review the bactericidal efficacy of aPDT as an adjunct to SRP against four major periodontal pathogens – Aa, Pg, Tf, and Td – in periodontal disease.
Materials and Methods
Focused question
Based on the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines, 26 a specific question was constructed. The addressed focused question was “Does aPDT as an adjunct to SRP exhibit better bactericidal effect against Aa, Pg, Tf, and Td than the use of SRP alone in periodontal disease?”
Selection criteria
Eligibility criteria were as follows: (1) original articles; (2) prospective clinical trials; (3) intervention, involving application of aPDT as an adjunct to SRP in treating periodontal disease; (4) controls, involving application of SRP in treating periodontal disease; (5) studies reporting any four major periodontal pathogens Aa, Pg, Tf, and Td in vivo after aPDT application in periodontal disease; and (6) studies published in English only.
The exclusion criteria included; review articles, in vitro and experimental studies, ex vivo studies, case reports, commentaries, interviews, and updates.
Search strategy
The authors (Z.A., U.D., A.H.S., and M.A.A.) searched the MEDLINE®/PubMed, Embase, Scopus, Web of Science, and Google Scholar databases from 1977 up to and including December 2015 for appropriate articles addressing the focused question. A structured and logical approach to literature searching was used to identify the relevant articles that reported the bactericidal efficacy of PDT against any one or all four periodontopathogens Aa, Pg, Tf, and Td in periodontal disease. Reference lists of original studies were hand searched to identify any articles that could have been missed during the initial search. Hand searching of the following journals was performed: J Clin Periodontol, J Periodontol, J Lasers Med Sci, Lasers Surg Med, Photodiagnosis Photodyn Ther, Photochem Photobiol Sci, J Periodontal Implant Sci, J Nat Sci Biol Med, Clin Oral Investig, and J Periodontol Implant Dent. Any disagreements regarding study selection were resolved via discussion. Electronic database searches were performed using different combinations of Medical Subject Headings (MeSH) terms and free text words:
Screening methods
Titles and abstracts of articles that satisfied the selection protocol were screened by the authors and checked for agreement. Full texts of studies judged by title and abstract to be relevant were read and independently assessed against the eligibility criteria. Following this, reference lists of original and review articles that were found to be pertinent in the previous step were hand searched and checked for agreement via discussion among the authors.
Study selection
The search protocol is presented in Fig. 1. A total of 59 studies were initially identified. Forty-two studies that did not fulfil the eligibility criteria were excluded (Appendix A). In total, 17 studies 19,20,25,27 –40 were included and processed for data extraction. All studies were performed at either universities or healthcare centers. Figure 1 shows the study identification flow chart with the reasons for exclusion of articles.
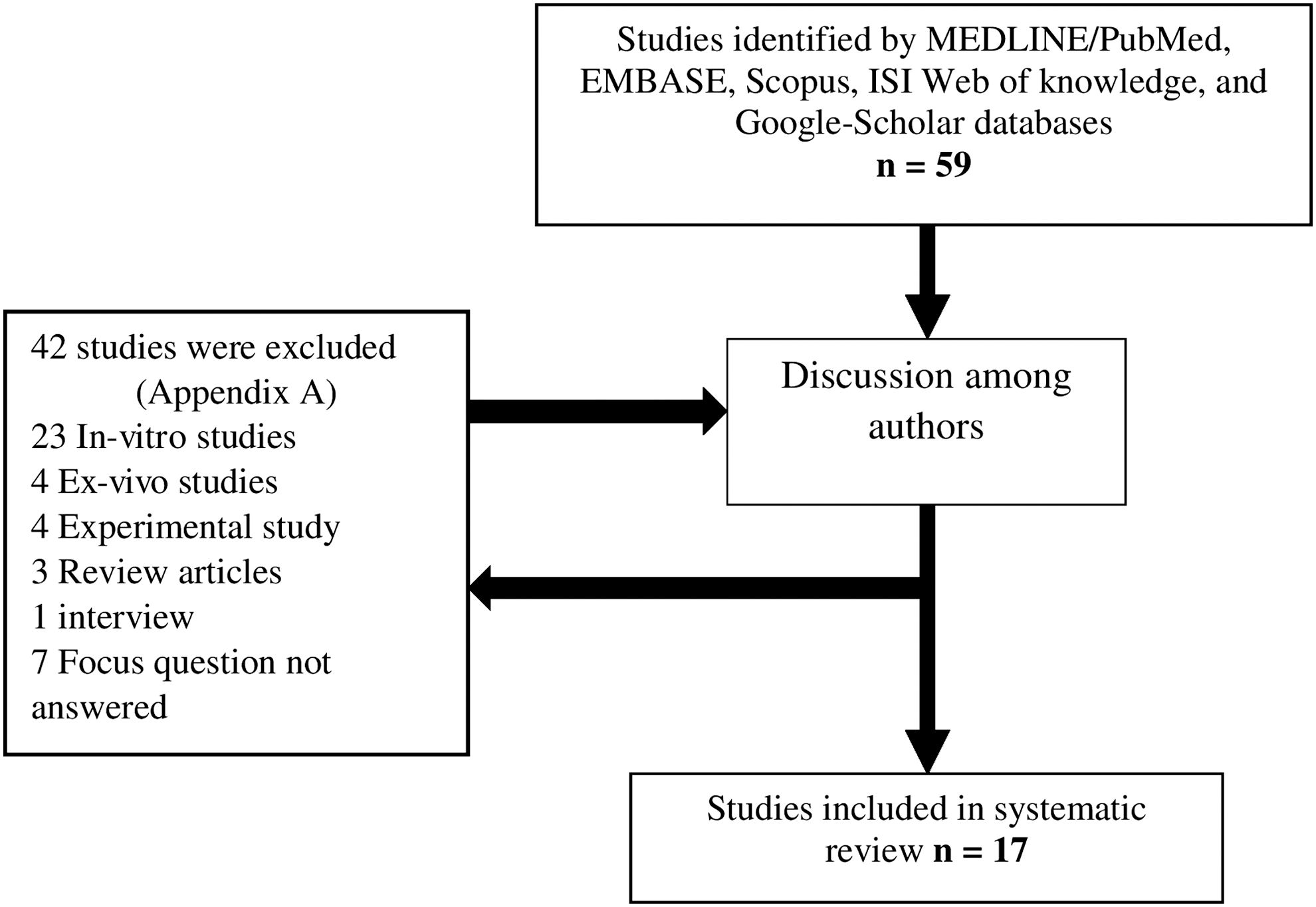
Study identification flow chart.
Methodological study quality assessment
Two authors (Z.A. and S.A.A.S.) independently assessed the methodological quality of the included studies according to a scoring system developed by the Jadad quality scale 41 for reporting randomized controlled trials. This scale is used to score randomized controlled trials on the basis of three items, which are randomization, blinding of examiner or patients, and an account of all the patients; for example, loss to follow-up. The scores range from 0 to 5 points, with a higher score indicating higher study quality.
Results
General characteristics of included studies
Nine studies 19,20,28,29,33 –36,40 included in the present review had split-mouth design. In all included studies, 19,20,25,27 –40 number of individuals ranged between 1035 and 58, 38 with mean age ranging between 29.029 and 52.036 years. All included studies reported the number of female participants, which ranged between 333 and 3925 individuals. All the included studies 19,20,25,27 –40 used aPDT with SRP in the test group. Two studies 20,34 used additional group of PS in their test group, whereas Birang et al., 28 and Cappuyns et al., 36 used laser therapy (LT) in their test group. One study 40 used curcumin gel combined with LT and PDT in their test group. Fifteen studies 19,20,25,28 –31,33 –40 used SRP alone, whereas two studies 27,32 used PS with SRP in the control group. Fourteen studies 20,25,27,28,30 –34,36 –40 included chronic periodontitis subjects whereas three studies 19,29,35 included patients with aggressive periodontitis. In all included studies, the follow-up period ranged from 431 to 4827 weeks (Table 1). All the enrolled participants had a complication-free healing period with no side effects related to aPDT, except for one participant who developed abscess during the follow-up period. 25
RCT, randomized clinical trial; aPDT, antimicrobial photodynamic therapy; CP, chronic periodontitis; AP, aggressive periodontitis; SRP, scaling and root planning; LT, laser therapy; PS, photosensitizer; NR, not reported; US, ultrasonic scaling; Aa, Aggregatibacter actinomycetemcomitans; Pg, Porphyromonas gingivalis; Tf, Tannerella forsythia; Td, Treponema denticola.
Laser and photosensitizer related parameters
Diode lasers with wavelengths ranging between 470 and 810 nm were used. Power output, energy fluence, and duration of irradiation were 75 mW, 212.23 J/cm2, and 60–180 sec, respectively (Table 2). Power density ranging between 13 and 500 mW/cm2 were used. Fifteen studies 19,20,25,27,29,30,32 –40 included in the systematic review used either methylene blue (MB), 20,27,32,33 toluidine blue (TBO), 29,34,39 phenothiazine chloride (PTC), 19,30,35 –38 tolonium chloride, 25 or curcumin 40 as PS. In all included studies, 19,20,25,27 –40 PS was placed in the periodontal pockets for 1–5 min. Studies 19,25,27,29,30,32 –35,37 –40 reporting the frequency of aPDT application ranged from one to four times throughout the study period. Five studies 19,20,32,33,37 reported the concentration of PS, which was 10 mg/mL, whereas one study 36 reported 0.1 mg/mL, and one study 40 reported the concentration as 10 mg/g.
PS, photosensitizer; PTC, phenothiazine chloride; TBO, toluidine blue; MB, methylene blue; TC, tolonium chloride; NR, not reported; aPDT, antimicrobial photodynamic therapy. aExpressed in mg/g.
Microbiologic-related parameters of the included studies
Sixteen studies reported the counts of Aa 19,20,25,27 –37,39,40 and Pg 19,20,25,27,28,30 –40 , whereas 14 studies 19,20,25,27,30 –39 and 11 studies 19,25,27,28,30,31,35 –39 reported Tf and Td counts respectively at follow-up. The bacterial counts were expressed in mean ± SD, mean total counts and proportions (Table 3).
PCR, polymerase chain reaction; aPDT, antimicrobial photodynamic therapy; SRP, scaling and root planning; PS, photosensitizer; LT, laser therapy; NR, not reported; US, ultrasonic scaling.
Significant intragroup difference related to baseline.
Significant difference between the groups.
Main outcomes of the study
All studies 19,20,25,27 –40 reporting periodontal pathogen profile, showed that aPDT application was effective in reducing the counts of all the four major pathogens, except one study, 37 in which the counts of Td were significantly increased at follow-up. Four clinical studies 19,30,34,35 showed significant reduction in the counts of Aa, Pg, Tf, and Td for aPDT as an adjunct to SRP as compared with SRP alone at follow-up. Novaes et al. 35 showed significant reduction only in Aa counts for aPDT as an adjunct to SRP, whereby counts of Pg, Tf, and Td were only significantly reduced in the SRP group at follow-up. Thirteen studies 20,25,27 –29,31 –33,36 –40 showed comparable reduction in the counts of bacteria when aPDT as an adjunct to SRP was compared with SRP alone.
In studies 20,34 utilizing PS in their test groups, Theodoro et al. 34 showed significant reduction in the Aa, Pg, and Tf counts in the aPDT group as compared with the groups treated with PS and SRP alone. Kolbe et al. 20 showed comparable outcome among all the groups for reduction in the Aa, Pg, and Tf counts at follow-up.
In studies 28,36 utilizing LT without PS in their test groups, comparable bacterial counts among aPDT, LT, and SRP groups were shown at follow-up.
One study 40 utilized curcumin combined with SRP, LT, and aPDT in their test groups. Comparable bacterial counts among all the three groups were reported at follow-up.
Quality of the clinical studies
All the studies 19,20,25,27 –40 included in this systematic review were randomized controlled trials. In the studies included, randomization was performed by the use of coin toss, 31,35,37,39 computer- generated sequence, 25,27,32 –34,36 opaque sealed envelopes, 19 and randomized charts. 28 Thirteen studies 19,20,25,27,29,31 –34,36 –39 reported the power and sample size calculation. The quality of six studies 19,25,28,31 –33 was regarded as high, because these studies received a score of 4 and 5. Eight studies 20,27,29,34 –37,39 were graded as moderate, receiving a score of 3, whereas three studies 30,38,40 were graded as poor, receiving a score of 2 or 1 (Table 4).
Discussion
The present study reviewed the in vivo bactericidal efficacy of aPDT as an adjunct to SRP against four major periodontal pathogens in periodontal disease. All included studies 19,20,25,27 –40 showed that adjunctive treatment with aPDT reduced periopathogenic microorganism counts in periodontal disease, except that by Chondros et al. 37 in which Td counts were significantly raised, and that by Novaes et al., 35 in which the counts of Pg, Tf, and Td were significantly increased in the aPDT group as compared with the SRP group at follow-up. Multiple explanations for the bactericidal effect of aPDT are proposed. These include DNA structural breakdown, efflux of potassium ions, modification of cell membrane proteins, and disruptions in the cell-wall synthesis. 22,42 It is also postulated that PS penetrates the outer membrane of the bacterium by the mechanism of the transfer of hydrogen ions. PS rapidly reacts with oxygen to form reactive oxygen species, 22,43 resulting in bacterial cell destruction.
Results from nearly 24% of the studies 19,30,34,35 that fulfilled our eligibility criteria showed significantly better bactericidal effect for aPDT as an adjunct to SRP than for SRP alone against periodontal pathogens. However, 76% of the studies 20,25,27 –29,31 –33,36 –40 showed comparable reduction in the counts of Aa, Pg, Tf, and Td when adjunctive use of aPDT was compared with use of SRP alone. It is noteworthy that the included studies had significant heterogeneity in the parameters related to aPDT. For example, the laser wavelengths in the studies, 30,34,35 showing significant reduction in the counts of periodontal pathogens in the aPDT group as compared with the SRP group was 660 nm, in contrast to the studies 28,29,37 –39 that showed comparable results between aPDT and SRP groups, whose laser wavelength ranged from 670 to 810 nm. Laser wavelength has an overall effect on the bactericidal efficacy of aPDT. 44 It is possible that increasing the wavelength of lasers in the studies 19,30,34,35 showing significant bactericidal effect of aPDT as compared with SRP could have modified the study outcomes.
Analysis of the studies reviewed also reveals a possible correlation between laser power density and the reduction of periodontal pathogen counts. Clinical studies 19,30,34,35 that showed significant reduction of Aa, Pg, Tf, and Td with the adjunctive use of aPDT as compared with SRP had a higher range of laser power densities (60–400 mW/cm2) than the studies 31,37 showing comparable periodontal bacteria reduction for aPDT and SRP application (13–75 mW/cm2). However, a relationship between laser power density and the bactericidal efficacy of aPDT remains to be established. Further, the type of PS used varied among the included studies and only 519,20,32,33,37 out of 16 studies 19,20,25,27 –39 reported the concentration of PS, which was 10 mg/mL. The dose of photosensitization in aPDT is a combination of different parameters of PS, light, and its acting time in the tissues and oxygen. 45,46 It is evident from the previous discussion that the variations in light wavelengths, laser power densities, types of PS, and their concentration would have resulted in a nonstandardized overall dose of aPDT in the included studies. Therefore, to assess the efficacy aPDT as an adjunct to SRP in eradicating major periodontal pathogens in periodontal disease, further randomized clinical trials with standardized laser and PS parameters are warranted.
The initiating step for the photosensitizing mechanism is light absorption by the PS resulting in excited singlet state and triplet excited state. 45 The interaction of a triplet excited state with surrounding molecules causes type I and type II photo-oxidative reactions causing bacterial cell death. 45 Interestingly, from all the included studies systematically reviewed, two studies 20,34 used only PS in their test group without application of light for eradication of Aa, Pg, and Tf. In these studies, 20,34 all three bacterial counts were comparable in PS application between baseline and follow-up; however, significant reduction in the counts of Aa, Pg, and Tf resulted from aPDT application at follow-up. These outcomes highlight the significance of the combined use of PS and light activation for the bactericidal efficacy of aPDT against Aa, Pg, and Tf.
A higher prevalence of Aa has been reported in tissue samples from aggressive periodontitis patients in comparison with those with chronic periodontitis. 47 As SRP is the mainstay in the management of chronic periodontitis, it is well recognized that antibiotic treatment as an adjunct to SRP is employed in the management of aggressive periodontitis. 15,48 Interestingly, the type of periodontal disease included in the clinical studies reviewed varied. In 319,29,35 out of 16 included studies, 19,20,25,27 –39 only aggressive periodontitis patients were included, and antibiotic therapy as an adjunct to SRP was not employed. In the presence of the varying prevalence of Aa and different disease conditions (some more favorable than other for the growth of Aa) as reported in the studies included 19,20,25,27 –40 in the present review, it is impossible to ascertain the bactericidal efficacy of aPDT as an adjunct to SRP against Aa, Pg, Tf, and Td in periodontal disease. Therefore, studies with standardized inclusion criteria and treatment regimens are recommended in this regard.
Conclusions
The bactericidal efficacy of aPDT as an adjunct to SRP against periodontal pathogens in periodontal disease remains unclear, given that the reported findings were inconsistent.
Footnotes
Author Disclosure Statement
No competing financial interests exist.