
Abstract
Introduction
D
Oral biofilms are composed by more than 700 different bacterial species. It is known that biofilms are 10–1000 times more resistant to antibiotic agents when compared with their planktonic counterparts. Other studies demonstrated that orthodontic patients have higher counts of Streptococcus mutans when compared with patients without orthodontic treatment. The initial clinical manifestation of the presence of oral cariogenic (caries-producing) biofilms, during orthodontic treatment, is the appearance of white spot lesions (ICDAS levels 0, 1, and 2). If not adequately treated, these white spots may develop into active carious lesions (ICDAS levels 3–6) around the brackets and metallic bands. 4 –6 Caries-preventive measures include instructions on oral hygiene and dietary habits, and the prescription of fluoride toothpastes and mouthwashes (≥1000 ppm). Antibiotic-driven decontamination has been proved to be effective against Gram-positive and Gram-negative bacteria. However, increasing reports of bacterial resistance restrain their use as oral decontamination agents in dentistry. Chlorhexidine, another well-known potent antibacterial agent, has been comprehensively demonstrated to be successful against several oral bacteria, and, therefore, it has been widely used as a topical agent in the decontamination of dental cavities and oral mucosa, but its continuous use has been implicated with the development of several adverse effects. 7,8
Antimicrobial photodynamic therapy (aPDT) has been demonstrated to be effective against a broad spectrum of microorganisms and, therefore, has been considered a possible candidate to control the oral cavity's microbial load. The aPDT's nonspecific antibacterial mechanism is based on the production of reactive oxygen species (ROS). It is believed that free radicals generated on light irradiation are capable of oxidizing organic molecules by a lipid peroxidation process. 9,10 Other studies 11 –14 have highlighted that due to the nonspecific nature of its underlying antimicrobial mechanism, it is unlikely that resistant bacterial strains could be developed due to the recurrent use of aPDT.
Current literature 15,16 indicates that, independently of photosensitizer type, concentration, wavelength, power output, and irradiation conditions, the antibacterial efficacy promoted with the use of aPDT is still at inadequate levels, which suggest its use as a decontamination agent against cariogenic biofilms. A previous in vitro study from our group 17 has demonstrated that aPDT using curcumin associated with the surfactant sodium dodecyl sulfate (SDS) and blue light inactivated S. mutans biofilms. Our findings suggested the establishment of a synergistic effect between the photosensitizer and the surfactant that optimizes the aPDT antibacterial mechanism. To the best of our knowledge, aPDT mediated by curcumin and blue light has never been used in combination with SDS in a clinical trial. Therefore, the aim of the present study was to investigate the antibacterial efficacy of the association of aPDT mediated by curcumin with SDS as an oral decontamination agent in orthodontic patients. Our working hypothesis is that the combination of aPDT with SDS will result in an optimization of antibacterial efficacy.
Materials and Methods
The Human Research Ethics Committee of the Federal University of São Carlos approved the execution of the present research (protocol N° 258.461). Selected patients signed an informed consent before they could participate in the present study. The present randomized and cross-sectional clinical trial study was registered at the NIH Clinical Trials (NCT02337192).
Inclusion and exclusion criteria
A total of 50 orthodontic patients from the city of São Carlos (São Paulo State, Brazil) were examined in a dental office to determine their participation eligibility. The inclusion criteria were as follows: ages between 18 and 50 years, being under fixed orthodontic treatment, absence of periodontal disease, having not used antibiotics 90 days before the study, and having not used fluoride mouthwashes. The exclusion criteria were as follows: presence of uncontrolled systemic diseases (e.g., diabetes, hypertension, and heart diseases), breast feeding or pregnant women, or patients with the presence of oral tumors, temporomandibular joint disorders, and with allergy history to any of the materials used, such as curcumin and chlorhexidine.
Experimental groups and conditions
After the screening process, 24 volunteers were randomly distributed into four groups (n = 6 patients/group) using a computer program, as follows: (1) Light group, which was treated only with blue light irradiation, no drug; (2) PDT group, which was treated with curcumin and blue light; (3) PDT + S group, which was treated with curcumin plus surfactant and irradiated with blue light; and (4) Chlorhex group, which was treated with chlorhexidine.
Preparation of the photosensitizer agent
The photosensitizer agent was synthesized immediately before each treatment according to the method previously described by our laboratory. 17 In brief, the photosensitizer was prepared by diluting 0.03 g of the curcumin salt (PDT Pharma, Cravinhos, Brazil) in 1.5 mL of dimethyl sulfoxide at 5% (DMSO; Labsynth, Diadema, Brazil). The solution was further diluted in 30 mL sterile distilled water, to obtain a final curcumin concentration of 1 g/L. The photosensitizer that was associated with surfactant required an extra step where SDS (Labsynth) in a concentration of 0.1% was added to the photosensitizer in its therapeutic concentration immediately before its use.
Irradiation devices to perform aPDT
To perform the irradiation of both teeth and oral cavity, we have used two distinct LED-based devices emitting blue light (Fig. 1): (A) Extra-oral irradiation (in-contact mode) of teeth was accomplished by using a commercial LED device (Bright Max Evolution 4; MMOptics, São Carlos, SP, Brazil) that was designed to provide concomitant irradiation of both the upper and lower arches in dental bleaching procedures, whereas (B) the intra-oral irradiation (noncontact mode) was performed with a prototype irradiation unit that was specifically developed for the present study (São Carlos Physics Institute, University of São Paulo, IFSC/USP). The former device is composed of four blue LEDs (450 ± 10 nm) mounted on a rectangular base (63.7 × 13.1 mm) with a transparent acrylic diffuser tip (heights: 32 mm [extremities] and 19 mm [central]). The latter device is composed of five LEDs (450 ± 10 nm) placed on a circular base of the 22 mm diameter with transparent acrylic diffuser tip with a cupola shape (length = 16.95 mm, radius = 12 mm). An optical power meter (FieldMaster TO-II; Coherent, Inc., Santa Clara, CA) connected to a photodetector (measurement area = 2.54 cm2; Coherent, Inc.) was used to measure the power intensities of each device used here. The intensity measurements revealed that the Bright Max device had an average optical power output of ∼200 mW and a power intensity of ∼80 mW/cm2, whereas the prototype LED device had an average optical power output of ∼1200 mW and a power intensity of ∼472 mW/cm2. Both the teeth and oral cavity were irradiated for a total of 180 sec, which led to an energy dose of ∼14 and 85 J/cm2, respectively. The irradiation parameters used in the present study are summarized in Table 1. The thermal images during clinical protocol is illustrated in Fig. 2.

Irradiation devices to perform antimicrobial photodynamic therapy. Teeth

Thermal image during clinical protocol. Before protocol
Treatments
For the PDT and PDT + S groups, the patients performed the swishing with the proper photosensitizer (curcumin alone or curcumin-associated SDS) for 2 min. Buccal and lingual surfaces of teeth were then sequentially irradiated (180 sec/each) using the devices previously described for a total irradiation time of 360 sec (∼100 J/cm2). Patients of the Light group performed the swishing with an aqueous solution of DMSO 5% during 2 min before irradiation. Patients of the Chlorhex group performed the swishing with chlorhexidine gluconate 0.12% for 30 sec.
Saliva collection
Collection of nonstimulated saliva (n = 3; 3 mL/collection) was performed at the following steps: (1) immediately before swishing (with curcumin, chlorhexidine, or water); (2) after swishing; and (3) after execution of aPDT treatments. Saliva was collected using 15 mL sterile polypropylene tubes (Falcon; BD Science, Durham, NC). After each collection, saliva samples were identified and stored in a refrigerated environment (dark conditions). Samples obtained from each patient in each experimental step were used for microbiological assessment.
Microbiological assessment
Aliquots of saliva samples (100 μL), from each collection step (as previously described), were diluted in 900 μL of phosphate buffered saline (PBS; Biogen, Ribeirão Preto, Brazil). Five 10-fold serial dilutions were then carried out in PBS for each sample. Aliquots (25 μL) of each dilution were plated (in duplicate) on Petri dishes containing Mitis Salivarius culture medium (BD Difco, Franklin Lakes, NJ) supplemented with 0.01 g of bacitracin. Petri dishes were incubated for 48 h (37°C). Colony-forming units (CFU) were then visually counted, and values were adjusted to CFU/mL using the correspondent dilution factor.
Statistical analysis
Shapiro–Wilk and Levene tests were used, respectively, to analyze the normality and homogeneity of variances of the data obtained (α: 0.05). Normalized data were then analyzed using two-way analysis of variance (ANOVA) with repeated measures. Independent factors were group (Light, PDT, and PDT+S) and time (before swishing, after swishing, and after irradiation), which were also considered as repeated measures. When significant differences were found, Tukey's post hoc test was applied. Paired Student test was used for Chlorhex group. The bacterial survival rate (nonnormalized data) was analyzed using ANOVA Kruskal–Wallis test. Statistical analysis was performed with a 95% confidence level using the program Statistica for Windows Release 7 (Statsoft, Inc., Tulsa, OK).
Results
The results of the antibacterial efficacy of the decontamination treatments proposed in the present research are presented in terms of S. mutans viability reduction (Table 2) and bacterial survival rates after experimental treatments (Fig. 3). Significant intragroup differences (p < 0.05) were observed in the experimental groups PDT, PDT+S, and Chlorhex when compared with the control group (swishing with water). S. mutans reductions for the groups PDT, PDT+S, and Chlorhex were 0.55 ± 0.27, 1.61 ± 0.41, and 3.34 ± 1.65 Log 10 CFU/mL, respectively. The highest bacterial reductions were observed in the experimental groups treated with PDT + S and Chlorhex, which have shown survival rates of 70 ± 5 and 43% ± 27%, respectively. There were no significant differences between PDT + S and Chlorhex groups (p ≥ 0.05).
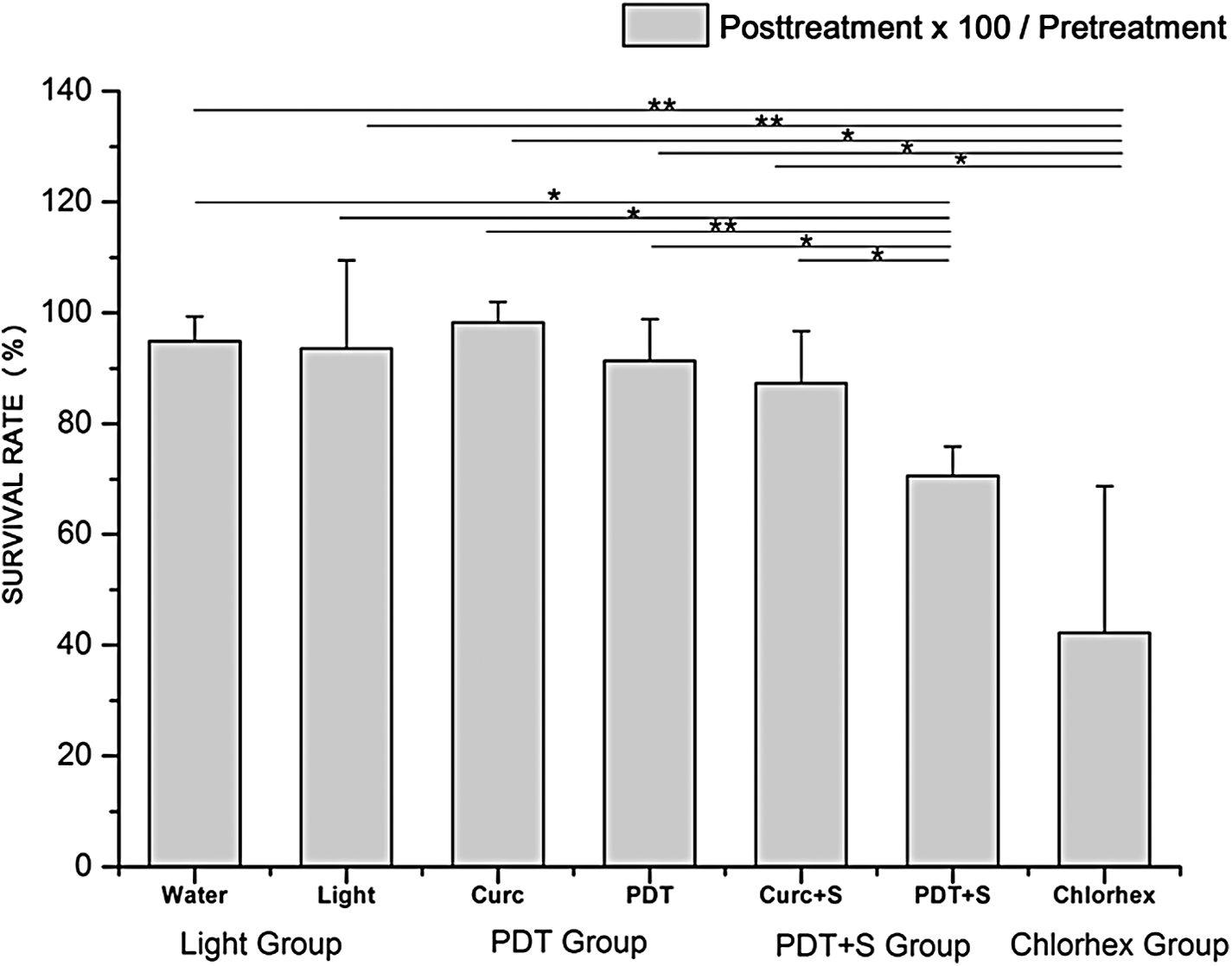
Bacterial survival for all situations. Water denotes swishing with water; Curc denotes swishing with curcumin; Curc+S denotes swishing with curcumin associated with surfactant; Light denotes irradiation with blue light; PDT denotes swishing with curcumin and irradiation with blue light; PDT + S denotes swishing with curcumin associated with surfactant and irradiation with blue light; and Chlorhex denotes swishing with chlorhexidine. Data shown as mean and standard deviation of the survival rate with a significant intergroup difference (*p < 0.05 and **p < 0.01).
Significant intragroup difference compared with pretreatment (* p < 0.05 and ** p < 0.01).
Significant intragroup difference compared with period immediately earlier († p < 0.05).
CFU, colony-forming units.
Discussion
PDT has been considered a suitable alternative approach to traditional antimicrobial treatments focused on the control of bacteria, fungi, viruses, and protozoans. In this context, aPDT can be easily adapted to treat several different infections such as chronic ulcers, infected burns, acne vulgaris, cutaneous leishmaniosis, gastric Helicobacter pylori infection, otitis media, sinusitis, tonsillitis, pneumonia, tuberculosis, osteomyelitis, onychomycosis, blood disinfection, and a variety of oral and tooth infections. 18 However, several studies 18 –21 have demonstrated that many variables such as type and concentration of photosensitizers, light sources, and irradiation parameters must be taken into consideration when developing novel aPDT protocols.
Florez et al. 20 investigated the aPDT's efficacy using curcumin, hypericin, and Photogem® in S. mutans planktonic cells. Their findings demonstrate that the combination of hypericin (1–10 mgL−1) and amber light (590 ± 10 nm, 55 mW/cm2) promoted complete eradication of S. mutans initial population (3 × 108 CFU/mL). However, this strong photodynamic action was not observed when using either curcumin (250–1500 mg/L) or Photogem (1–10 mg/mL) as photosensitizers. Our results are in agreement with the findings reported by Florez et al. 20 regarding the poor antibacterial effects observed for curcumin-mediated aPDT against S. mutans in saliva (planktonic cells).
However, several in vitro 21,22 and in vivo 23 studies showed that the aPDT with curcumin and blue light reduced CFU counts. Paschoal et.al. 22 demonstrated that aPDT using higher doses (48 and 72 J/cm2) associated with curcumin (4000 μM) promoted moderate levels of microbial inactivation (between 60.66% and 71.07%). Araújo et al. 21 demonstrated that aPDT with curcumin (1.5 g/L) and blue LED (470 ± 15 nm) at a low dose (5.7 J/cm2) was able to maximize the S. mutans inactivation in planktonic cultures. 20 In a clinical trial, Araújo et al. 21 reported significant levels of microbial inhibition using curcumin (1.5 g/L) and blue light irradiation (450 ± 15 nm, 67 mW/cm2) for oral decontamination. In another clinical trial, Leite et al. 23 showed lower levels of microbial inhibition after aPDT in oral cavity, but this reduction remained over time.
Some studies have reported that bacterial composition within multi-species biofilms varies considerably depending on the colonization niche considered and among different people. This complexity of bacterial species is believed to adversely impact the aPDT treatments' antibacterial efficacy. Therefore, and to improve the efficacy of the experimental aPDT treatments proposed in the present study, we have used higher averages of power output and energy doses along with shorter periods of light irradiation when compared with other in vitro 17 studies and clinical trials 23 previously reported. Moreover, the anatomical and morphological features of oral cavity and tooth structure may possibly affect light distribution, but this complexity is mostly evident in the areas of teeth roots. 24,25 Although there are small differences in the anatomical structure of dental arches, 26 two distinct irradiation devices used in the current study allowed for the proper delivery of light.
Regarding the short time of irradiation, Dovigo et al. 27 demonstrated that the blue light absorption and the fluorescence of curcumin were reduced as a function of irradiation time. There were the spectral changes when measurements of the induced photobleaching of the curcumin molecules were performed, indicating the potential photodynamic response. It suggests that the high photobleaching rate of curcumin is correlated with low levels of ROS formation after long periods of irradiation. 27 Chignell et al. 28 suggested that the photobleaching of curcumin results in the obtainment of a less active photosensitizer due to the presence of fewer optically active molecules, thereby supporting the irradiation protocols proposed here. Thus, in the current clinical trial, the short time of irradiation (180 sec) may have resulted in efficient ROS generation together with a low photobleaching rate, mainly when SDS surfactant was added in curcumin solution, reducing CFU.
Our previous in vitro study investigated the effects of aPDT on S. mutans biofilms using curcumin (1 g/L) associated with SDS surfactant (0.1%) and blue LED (455 ± 15 nm) delivering 30 J/cm. 2,17 In this study, the addition of surfactant to perform aPDT showed higher bacterial inactivation levels (5.6 Log) compared with the control group without treatment. 17 An similar in vitro study 29 showed the effects of aPDT with red LED (100 mW and 200 mW/cm2) combined with methylene blue and four different surfactants (CTAC [cetyltrimethylammonium chloride], HPS [N-hexadecyl-N-N 0-dimethyl-3-ammonio-1-propane-sulfonate], Triton X-100 [octylphenoxypolyethoxyethanol], and SDS) with subinhibitory concentrations (32, 16, and 8 μg/mL) on the inactivation of Candida albicans. Thus, these combined therapies showed higher antifungal and antimicrobial activity when aPDT or surfactants were applied alone. 29 However, Lyon et al. 29 obtained better results with CTAC and HPS than Triton X-100 and SDS, because SDS is anionic surfactant, triton X-100 is nonionic surfactant, and CTAC and HPS are strongly associated with the presence of the cationic charge. It acts on Gram-positive bacterial cell walls that contain peptidoglycan, interfering with nucleic acid synthesis and leading to genetic mutation and DNA-strand breaks due to photodynamic action. 22,29
In this context, surfactants alone have antimicrobial activity. 29,30 Low concentrations of the surfactant agent may reduce or inhibit microbial adherence. In parallel, high doses of curcumin alone also lead to antimicrobial activity. 31 On the other hand, Leite et al. 23 demonstrated that low doses of curcumin significantly increased CFU at 1 h post mouthwash, suggesting disaggregation of dental plaque clumps on tooth enamel and leading to saliva. However, in our study, the curcumin alone (1 g/L) or curcumin associated with surfactant (0.03 g/L) without light did not promote any significant change.
Low levels of curcumin are used for aPDT. They are conducive for reduction of CFU 21,27,32 as observed in our study. Thus, the aPDT with the surfactant SDS potentiated the bacterial reduction. Chemical compounds act by decreasing the superficial free tension between the photosensitizer and the microorganisms; simultaneously, this increases their trans-membrane permeability. 29 This twofold effect guarantees a higher photosensitizer concentration inside of the cells, which, ultimately, will permit the obtainment of a more optimized photodynamic reaction. However, it was not better than chlorhexidine.
Several studies 33,34 showed the effectiveness of oral decontamination for oral hygiene, leading to produce a reduction in the mouth odor and a prevention of the pneumonia with chlorhexidine. Low concentrations of chlorhexidine (0.12–0.2%) are used for oral decontamination. Chlorhexidine is also a cationic agent that exhibits broad antimicrobial effects. 35 However, Somal and Derby 33 demonstrated that its efficacy is insufficient to reduce the incidence of respiratory infections due to resistant bacteria. According to Järvinen et al., 36 oral S. mutans remains susceptible to chlorhexidine as well as to systemic antibacterial agents (amoxicillin, cefuroxime, penicillin, sulfamethoxazole-trimethoprim, tetracycline, and erythromycin). The resistance of some microorganisms to chlorhexidine that can be observed in some patients may explain the large standard deviation found in the Chlorhex group when compared with the PDT + S group. 36 Moreover, the long-term use of chlorhexidine oral may cause black/brown staining of teeth, tongue, and restorative materials, burning sensation, alteration of taste, and an increased calculus formation. 8,37 In the present study, patients had no side effects, because chlorhexidine required swishing only once as well as lower concentrations of the photosensitizer and SDS surfactant were used.
Conclusions
The results presented indicate that curcumin associated with surfactant and blue light has the potential to reduce S. mutans load in the saliva of orthodontic patients. In this context, the surfactant SDS optimized aPDT. However, other surfactants should be explored to obtain bacterial reduction that exceeds the results obtained with the chlorhexidine use. In addition, long-term studies should be performed to compare aPDT and other known antibacterial treatments.
Footnotes
Acknowledgments
The authors would like to acknowledge the São Paulo Research Foundation (FAPESP)—Grant Nos. 2013/07276-1 and 2013/14001-9, the National Council for Scientific and Technological Development (CNPq)—Grant No. 573587/2008 and Coordination for the Improvement of Higher Education Personnel (CAPES). The authors also would like to acknowledge the scientific contributions of Clovis Grecco.
Author Disclosure Statement
No competing financial interests exist.