
Abstract
Introduction
D
The vascular endothelial growth factor (VEGF) is one of the most important factors involved in angiogenesis, exhibiting a notable presence in Achilles tendon injuries. 7 This increase in the VEGF has been interpreted as beneficial, since it is an attempt to increase the number of blood vessels and the nutritional contribution. Consequently, the proliferative rate increases, as does the healing process in the Achilles tendon. 8,9
However, there is evidence that this strategy is ineffective, as it is not strong enough to heal the Achilles tendon and the new vessels that appear are accompanied by new nerve bundles, thereby increasing nociceptive afferents and pain. 10 In addition, VEGF induces the expression and presence of distinct deleterious and degrading factors in the tendon tissue, including matrix metalloproteinases (MMP), which delay the healing process and may even weaken the injured tendon further. 8,11
Low-level laser therapy (LLLT) has provided satisfactory results when used to treat Achilles tendon injuries, due to the proliferative and modulatory stimulation it promotes. 3 –6,12 There are also some reports of increases in the expression and presence of VEGF in several experimental situations in which LLLT was involved. This phenomenon—if not clarified and controlled—could hinder the healing process of the Achilles tendon. 8,13 –16
Although there are positive reports of the interaction between LLLT and Achilles tendon injuries, there are still uncertainties about the main active pathways involved and whether this angiogenic characteristic of LLLT, which is found in different clinical and experimental situations, also occurs in Achilles tendon injuries. 3,5,6 Thus, the aim of the present study was to analyze the modulatory effects of near infrared (780 nm) LLLT on the presence of VEGF in the partially injured Achilles tendons of rats.
Materials and Methods
The present study was approved by the Research Ethics Committee of the Universidade Federal de São Paulo under protocol number 0074/2011.
Sixty-five male 12-week-old Wistar rats (Rattus norvegicus: var. albinus, Rodentia, Mammalia), weighing between 270 and 300 g, were used. They were kept in standard polypropylene cages, with a light/dark cycle of 12 h, a temperature of ∼20°C, and 65% of humidity. They received water and rat chow ad libitum.
Injury procedure
Sixty animals were randomly anesthetized with an intraperitoneal injection of ketamine hydrochloride (100 mg/kg) and xylazine hydrochloride (50 mg/kg). The five remaining animals were not submitted to anesthesia.
After anesthesia, manual trichotomy of the right hind paw was performed (Achilles tendon areas). The animals were positioned at an injury device base—a mini-guillotine dispositive designed to drop weight and promote injury by direct trauma. The right hind paw was positioned on the equipment base, and mild traction was exerted through ankle dorsiflexion until the dorsal region of the paw rested against the injury device base. Finally, a weight of 186 g was released from a height of 20 cm onto the Achilles tendon of each animal, corresponding to a potential energy of 364.9 mJ at the time of trauma. 3,4
Group distribution
After partially injuring the Achilles tendon of 60 animals, they were distributed randomly into six groups: • Sham 1: 10 tendons submitted to simulated LLLT for 1 day. • LASER 1: 10 tendons submitted to LLLT application for 1 day. • Sham 3: 10 tendons submitted to simulated LLLT for 3 days. • LASER 3: 10 tendons submitted to LLLT application for 3 days. • Sham 7: 10 tendons submitted to simulated LLLT for 7 days. • LASER 7: 10 tendons submitted to LLLT application for 7 days.
The five remaining animals (10 tendons) were placed at the Control group and were not submitted to any procedures.
Laser treatment
The AsGaAl LLLT (MM Optics®, Model: Twin Laser) equipment was used. Table 1 presents the LLLT parameters applied.
LLLT, low-level laser therapy.
Laser was performed manually once a day at the central portion of injured Achilles tendons, with the animal gently caged and immobilized during treatment and/or simulation period. The animals were treated for 1 day (LASER 1), 3 consecutive days (LASER 3), or 7 consecutive days (LASER 7). Treatment started 1 min after induced injury and contact technique and continuous emission were used in all irradiations. 3,4,17
In Sham groups (1, 3, and 7), simulated applications of LLLT were performed, with the apparatus turned off. However, contact was made between the equipment and the injured area for the same period of time as in the treated groups.
Euthanasia
The animals in the LASER 1/Sham 1, LASER 3/Sham 3, and LASER 7/Sham 7 groups were euthanized (inhalational anesthetic overdose with isoflurane, 5% for induction and 2% maintenance until euthanized) 24 h, 4 days, and 8 days after the injury had been induced, respectively. The animals in the Control group were euthanized on the last day of the experiment (eighth day).
Sample processing
After euthanasia, tendons of the two hind paws were surgically removed from animals in the Control group, as well as the 60 tendons (right hind paw) of animals belonging to the other groups.
The tendons were immediately washed in saline solution (0.9%) and then fixed in paraformaldehyde (4%) in a Millonig 0.1 M buffer (pH 7.2–7.4) for 12 h.
After fixation, the tendons were washed in the buffer and dehydrated in increasing solutions of ethyl alcohol (from 70% to 100%) for 45 min in each solution. Next, they were diaphanized in xylene (two baths of 45 min each) and included in paraffin, positioned in such a way that longitudinal slices could be obtained. Microtome slices (model: RM2155; Leica) with a thickness of 5 μm were used in immunohistochemistry. The slides were silanized (3-aminopropyl-triethoxysilane—Sigma) for slice adhesion.
Each slide was prepared with a slice from each tendon to quantify the VEGF levels, a process that was repeated thrice. Therefore, three nonconsecutive slides were obtained for each animal studied.
All of the sections were dewaxed, hydrated, and submitted to the above method.
Analysis of angiogenesis (immunohistochemistry)
A specific antibody kit for the VEGF was used (anti-VEGF monoclonal; brand: Abcam—AB1316; dilution: 1/200). The dewaxed slices were washed in distilled water and Tris-phosphate buffer pH 7.4 (TBS).
Antigen retrieval was performed using pork trypsin 0.25% in phosphate buffer (code T7409; Sigma Aldrich) for 20 min at 37°C. Endogenous peroxidase was blocked with hydrogen peroxide 10v (3%). The samples were then washed in tap water, deionized water, and then left in phosphate buffer pH 7.4 (PBS). Nonspecific proteins were blocked through the immersion of the slides in casein (Synth) and diluted in PBS (pH 7.4) for 5 min at room temperature.
The slides were incubated with the primary antibodies in a specific diluent (Spring Bioscience) for 24 h at 4°C and then incubated with the secondary antibody Histofine (Nichirei Biosciences, Inc.) for 45 min at 37°C. Subsequently, the slides were washed in water and the sections were placed in diaminobenzidine (DAB) (Spring Biosciences) for 10 min at room temperature.
Finally, the slices were counterstained with Harris hematoxylin (Merck) and mounted with Entellan (Merck).
The effect of the treatment on the VEGF response of the injured Achilles tendon was analyzed in three different anatomical regions of the tendon (proximal, intermediary, and distal) to identify and quantify positive cell types. Two random images of each of the anatomical regions analyzed were collected, with a zoom of 200× (objective 20×), using a DFC420 camera (Leica Microsystems) coupled to a DMLB microscope (Leica Microsystems). After obtaining the images, cells that exhibited positive markings were identified and quantified using version 4.5.0 of the LAS computerized image system (Leica Microsystems).
Statistical analysis
The Statistical Package for Social Sciences (SPSS®—version 15.0) was used, with the level of significance set at 5% (p < 0.05). The Levene's tests and one-way analysis of variance (ANOVA) were used to assess the homogeneity of the data and to compare the results between the groups, respectively. The data were displayed in mean and standard deviation values and the result of the comparisons was reported using the F test, when homogeneity of the variances was recorded. If differences were to be recorded between the groups, Tukey's multiple comparisons tests (post hoc) were conducted.
Results
Table 2 presents the total number of positive cells for VEGF in the proximal, intermediary, and distal regions analyzed. The experimental groups (LASER and Sham: 1, 3, and 7) did not exhibit elevated levels of angiogenesis at the analyzed regions and also at the total average when compared with the Control group (p > 0.05).
VEGF, vascular endothelial growth factor.
The intergroup analysis (Sham 1, 3, and 7 vs. LASER 1, 3, and 7) concerning the number of applications (1, 3, and 7) and the regions analyzed (proximal, intermediary, and distal) also exhibited no statistically significant differences for the levels of VEGF (p > 0.05), with similar angiogenesis patterns (Fig. 1).
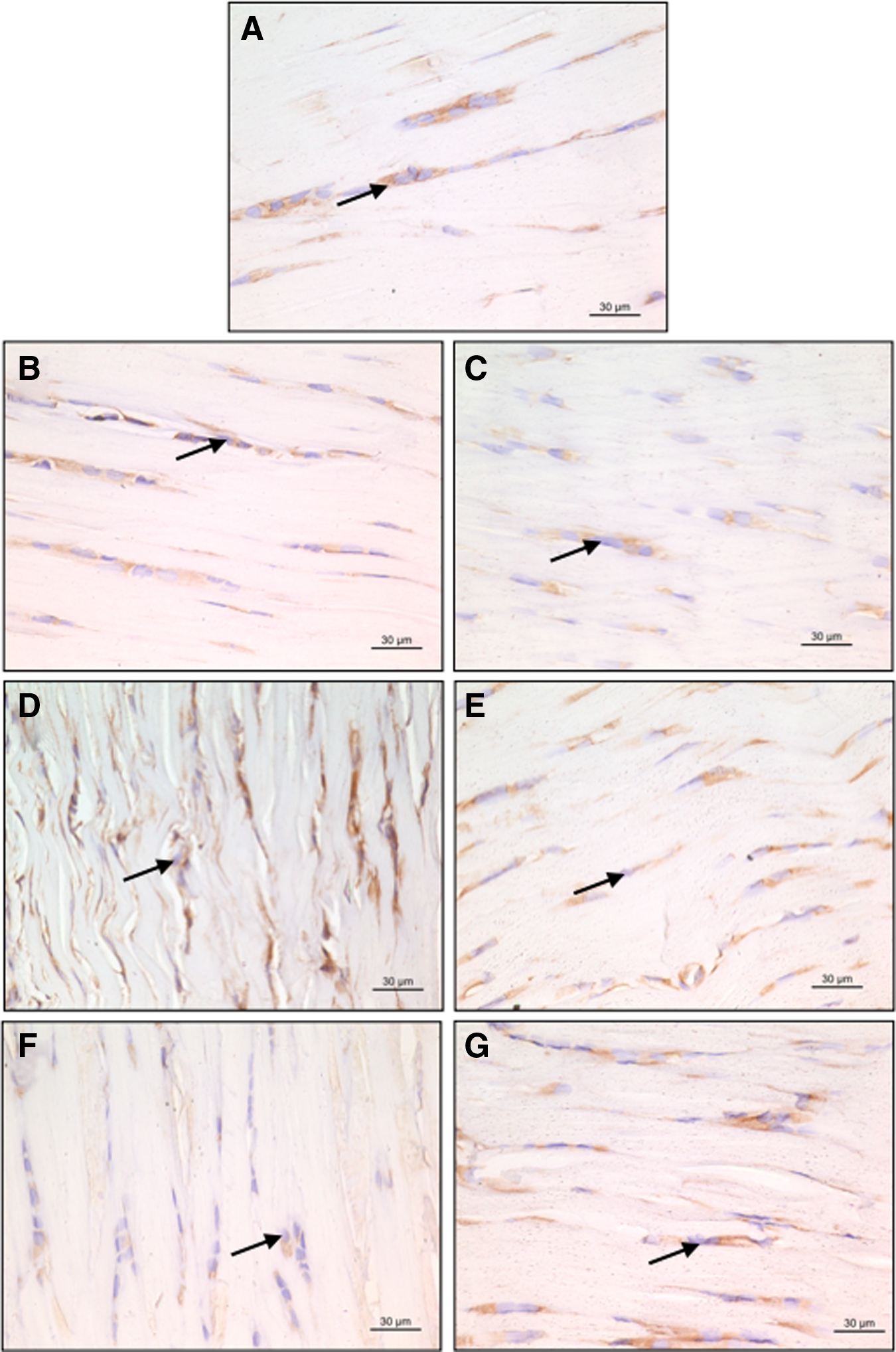
Photomicrography of the mean values for cells that were positive (
Discussion
The aim of this controlled laboratory study was to analyze the effect of LLLT on the VEGF modulation of the partially injured Achilles tendons of rats. The most significant result obtained was the maintenance of the quantity of VEGF at near-normal levels in the tendons treated with LLLT.
Achilles tendon injuries are complex and multifactorial, as is the subsequent healing process. 4,18,19 LLLT has provided promising results when used in the treatment of Achilles tendon injuries, basically acting in two pathways: proliferative (regeneration and collagen reorganization) and modulatory (controlling the inflammatory process). 3 –6
Besides the regeneration and reorganization of collagen fibers and the control of the inflammatory process, modulating the VEGF levels is important when seeking to repair injured Achilles tendons, given that its high and uncontrolled presence may hamper and delay the healing process once VEGF induces the expression of tendon tissue degrading factors and also may increase pain (stimulating the presence of new nerve bundles) during rehabilitation programs. 8,10,11,18,20
There are reports in the literature of increases in VEGF levels based on the induction of Achilles tendon injuries. However, unlike the present one, these studies used different methods of tendon injury (collagenase), which in turn may be more specific to trigger the modulation of VEGF levels. 20 In addition, the periods studied were longer than those proposed in this study, which may have perpetuated the tendon injury for enough time to induce and favor the detection of VEGF modulations. 20
The LLLT applied in this study, different several previous reports in the literature, 13 –16,21 did not cause an increase in VEGF levels, which may be a positive effect given the complications that this increase can cause when found in injured tendon tissues. 7 –11 Although the active mechanisms of LLLT in Achilles tendon injuries have not been completely clarified, it is probable that this LLLT (which exhibits anti-inflammatory effects) reduces the migration of proinflammatory agents (macrophages and monocytes) to the injury site, thereby maintaining near-normal VEGF levels, since VEGF is also secreted by these agents. 6,11,19,20
Furthermore, the interaction between LLLT and the different types of tissues and factors involved in the healing/regeneration processes depends on a number of factors: wavelength, mean power, and the dose and frequency of the treatment. 22 –24 There are reports in the literature showing modulations in VEGF levels with a lower mean power (22 mW) and a higher final energy (1.54 J) 20 than those used in the present study. It is probable that our dosimetric parameters did not achieve the required specificity and thus did not promote an increase in the VEGF levels.
Conversely, there are also reports in the literature showing the proliferation and reorganization of collagen fibers, as well as the reduction of the levels of proinflammatory and deleterious factors of injured Achilles tendons using the same LLLT protocol (wavelength, dose, and treatment frequency). These reports also used the same experimental model as the present study, demonstrating the specificity of this LLLT in the interaction with these other factors during the repair of injured Achilles tendons. 3 –6,18
Therefore, this LLLT protocol exhibited positive effects on the healing of injured Achilles tendons (specifically by increasing collagen proliferation and organization) and on the control of the inflammatory process, acting in a proliferative and modulatory, rather than an angiogenic pathway, since there was no increase in the VEGF levels after its application.
Although no VEGF modulation was found with the LLLT used in this study, uncertainty remains about its effects when applied in other experimental models (more aggressive and chronic injuries) and other treatment protocols—since this research investigated a small period and a single method of analysis—and there is also uncertainty about the best LLLT parameters.
Conclusions
Near infrared 780 nm LLLT did not stimulate VEGF expression at the partially injured Achilles tendons at the early stages of the repair process.
Footnotes
Acknowledgment
The authors thank the São Paulo Research Foundation (FAPESP) for supporting this study (2011/00979-1) and Magna Aparecida Maltauro Soares for providing technical support.
Author Disclosure Statement
No competing financial interests exist.