
Abstract
Introduction
S
High costs of care, increased antibiotic resistance, and the obvious morbidity and potential mortality associated with SSIs have driven a significant amount of investigation aimed at reducing SSIs. There has been some success, but there is still a gap to be closed. 4 This is in large part due to the alarming increase in multi-drug-resistant bacteria, particularly the ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species). Today, the heavy and inappropriate use of antibiotics has contributed to widespread resistance, resulting in superbugs that are unresponsive to conventional therapy. Given the harsh reality and growing concerns over antibiotic resistance along with reluctance by the industry to develop new antibiotics, 5,6 finding an alternative means to reduce infection rates in the face of antimicrobial resistance is warranted.
UVC light has wavelengths ranging from 100 to 280 nm. At appropriate doses, UVC can inactivate surface pathogens while preserving the viability of host cells. UVC is bactericidal, directly damaging DNA through the formation of cyclopyrimidine dimers regardless of drug resistance. 7 –10 A distinct advantage of UVC is that it has a limited ability to penetrate deeper tissues, thus minimizing cellular damage to the host. 11 Additionally, UVC does not discriminate between highly drug-sensitive organisms and multi-drug-resistant organisms. 12 Studies have demonstrated that UVC is bactericidal in wounds and can dramatically lower the bacterial bioburden. 7 –15 Differences have been seen in susceptibility of different bacterial species to ultraviolet light, making it important to identify the susceptibility of pathogenic species. For example, it is possible for bacteria to inherently have superior DNA repair mechanisms that are not error-prone in the face of UV exposure, which may allow for differences in survival among bacteria having a similar cell wall structure and thickness 16,17
Given the scarcity of medical literature evaluating the efficacy and safety of UVC, it is not surprising that UVC has not been adopted as a widespread clinical tool. Concerns over occupational exposure will necessitate that UVC be used at the lowest effective dose with precise treatment protocols. To our knowledge, no study has determined the lowest effective dose for clinically applicable scenarios. The dog is the most common species treated in veterinary medicine and it is important to validate UVC efficacy in this species. Equally important, the dog has a stratum corneum that more closely approximates that of humans. 18 –20 Previous studies have generally aimed to completely sterilize contaminated wounds, which require relatively high doses of UVC. Our work is different in that we explore the concept of decreasing bacterial burden to a level that is unlikely to be able to establish an infection in a typical clinical scenario by demonstrating that it is comparable with chlorhexidine. Our group has already performed significant pilot work on dosing of skin and muscle tissue surfaces and proposes the use of doses over 80 times less than reported in the literature. 7,15 We hypothesize that low-dose UVC will result in a similar reduction of multi-drug-resistant ESKAPE pathogens E. faecium, S. aureus, and Klebsiella pneumonia compared with 0.05% chlorhexidine and be synergistic when used in combination with 0.05% chlorhexidine. It is our ultimate hypothesis that when used appropriately, UVC is a potentially effective and synergistic tool in prevention of SSIs and treatment of wounds. Such data are critical in the development of treatment protocols and determining whether UVC is a suitable treatment modality for the prevention or treatment of SSIs, as well as other applications in humans.
Methodology
UVC light source
A low-pressure mercury vapor lamp with a peak emission at 254 nm (American Ultraviolet, Lebanon, IN) and a UVC LED (SETI, Columbia, SC) light were utilized to deliver UVC. Both light sources underwent peak spectral emission testing at our laboratory to confirm output using a commercially available spectroradiometer (International Light Technologies, Peabody, MA). To ensure a stable output, the mercury lamp was warmed for a minimum of 5 min before each use. Light emissions were confirmed before and after each use with a UVC dosimeter (Solartech, Harrison, MI). Based on the dosimeter reading, the exposure times required to achieve a dose of 0.015, 0.03, and 0.04 J/cm2 were calculated. Preliminary studies were performed to calculate the exposure time at a fixed distance, as summarized in Table 1.
These treatments were performed for skin inoculated with S. aureus, K. pneumoniae, or E. faecium
Harvesting of canine skin and muscle
All skin and muscle biopsies were obtained from dogs that were freshly euthanized for reasons unrelated to the study. The harvesting of tissues was approved by University of Florida IACUC number 201508767. Samples were obtained from areas of the body that appeared grossly normal. The trunks of dogs were most frequently used as this region of skin was easily accessible. These dogs were part of a surgical teaching laboratory, in which veterinary students and surgical residents performed reconstructive surgeries and were considered to be in good health. The skin and muscle removed to perform these reconstructions were opportunistically harvested for use in this study. The subject's skin was clipped and cleaned with saline. Ten millimeter diameter skin and muscle specimens were generated from the harvested tissues utilizing a Keyes punch biopsy instrument. A total of 200 skin and 200 muscle specimens were collected from various dogs. The specimens were vacuum packaged and then packaged in a self-sealing sterilization pouch for storage in a −80° freezer until gamma irradiation for sterilization. All skin and muscle samples were placed in dry ice for transfer to a gamma irradiation facility (FTSI, Mulberry, FL). The samples were sterilized with a dose of 25 kGy. The samples were then returned to the −80° freezer until use.
Microorganism isolates
The University of Florida's Veterinary Diagnostic Laboratory provided one clinical isolate of multi-drug-resistant K. pneumoniae. Methicillin-resistant S. aureus (MRSA) ATCC 43300 and multi-drug-resistant E. faecium ATCC 51559 were purchased (American Type Culture Collection, Manassas, VI).
Preparation of inoculum
All bacteria were grown for 18–24 h on Columbia blood agar (Hardy Diagnostics, Santa Maria, CA) in an air-forced incubator at 95% ± 2% relative humidity in 5% CO2 at 35°C–37°C. To achieve optical density equal to McFarland 0.5 standard (Sensititre, Inc., Westlake, OH), the isolated colonies were suspended in sterile double-distilled water.
Bacterial inoculation and treatments
Specimens were sterilized in groups of 11 based on the number of treatments performed, in which one treatment was performed per group (Tables 1 and 2). Group 1 received no inoculation of bacteria as its treatment to confirm the skin or muscle specimens were free of bacteria before testing. The central region of the specimen was swabbed with a sterile rayon-tipped applicator. The applicator was transferred to 1 mL of sterile deionized water, allowed to incubate at room temperature for 10 min, and then vortexed. Once mixed, 100 μL of the negative control sample was plated to Columbia blood agar with 5% sheep's blood (Hardy Diagnostics) and incubated at 95% ± 2% relative humidity in 5–10% CO2 at 35–37°C for 18–24 h, at which time colonies were counted by the primary investigator.
These treatments were performed for muscle inoculated with S. aureus, K. pneumoniae, or E. faecium.
Group 2 served as the negative control; the specimen was coated with 30 μL of a water-based solution containing a concentration of bacteria (determined in preliminary studies), resulting in a colony-forming unit (CFU) count ranging between 30 and 300 colonies. The final concentrations used on skin samples for S. aureus, K. pneumoniae, and E. faecium were 1.5 × 106/mL, 1.4 × 106/mL, and 1.5 × 106/mL, respectively. The final concentrations of S. aureus, K. pneumoniae, and E. faecium used on muscle samples were 1.3 × 106/mL, 1.4 × 106/mL, and 1.5 × 106 mL, respectively. Once the 30 μL of target bacteria was delivered onto the surface of the sample, it was allowed to dry for 30 min at room temperature. After drying, a central region of the specimen was swabbed and processed as described for treatment 1.
Groups 3–8 were inoculated as described above with 30 μL, followed by exposure of UVC with the 254 nm mercury light or the 270 nm UVC LED at doses of 0.015, 0.03, and 0.04 J/cm2. Cultures were obtained as described above after exposure by swabbing the central region with a sterile rayon-tipped applicator and transferring the applicator to 1 mL of sterile deionized water. After 10 min, the applicator was vortexed and 100 μL of the sample was plated.
Groups 9 and 10 were inoculated as described above with 30 μL. Sterile rayon-tipped applicators were then used to scrub the corresponding specimen thrice in an alternating manner with sterile saline and 0.05% chlorhexidine or 2% chlorhexidine, which resulted in a contact time with chlorhexidine of ∼60 sec. Cultures were obtained immediately after swabbing with a sterile rayon-tipped applicator and transferring the applicator to 1 mL of sterile deionized water. After 10 min, the applicator was vortexed and 100 μL of the sample was plated. Two percent chlorhexidine was considered the positive control.
Group 11 was inoculated as described above with 30 μL and underwent an alternating scrub with sterile saline and 0.05% chlorhexidine, which resulted in a contact time with chlorhexidine of ∼60 sec. This was immediately followed by exposure to 0.015 J/cm2 using the 254 nm mercury light. Culture swabs from the central region were obtained and plated 10 min after exposure as described above.
Bacterial counts were not blinded and the primary investigator manually counted all CFUs. A grid was drawn onto the plate with a permanent marker to assist in counting.
Statistics
CFUs were recorded for controls and for individual treatments as continuous numerical data. The data were determined to be nonparametric using a Shapiro–Wilk test and summarized using outlier box plots. A Kruskal–Wallis test was used to compare differences among groups (individual bacteria and tissue) by treatment type (Controls, UVC, and Chlorhexidine). The Wilcoxon method was used for comparison of individual treatments within each group when significance was determined by the overall Kruskal–Wallis analysis. p Values less than 0.05 were considered statistically significant.
Results
All skin and muscle samples were confirmed to be sterile before inoculation of bacteria based on negative culture results of a skin or muscle sample used to ensure sterility within each batch of assays. There were no significant differences in CFU counts when comparing UVC light sources (254 nm mercury vs. 270 nm LED) for MRSA, K. pneumoniae, or E. faecium. Therefore, for all subsequent statistical analyses, the light sources were grouped together according to UVC dose.
Methicillin-resistant S. aureus-inoculated skin
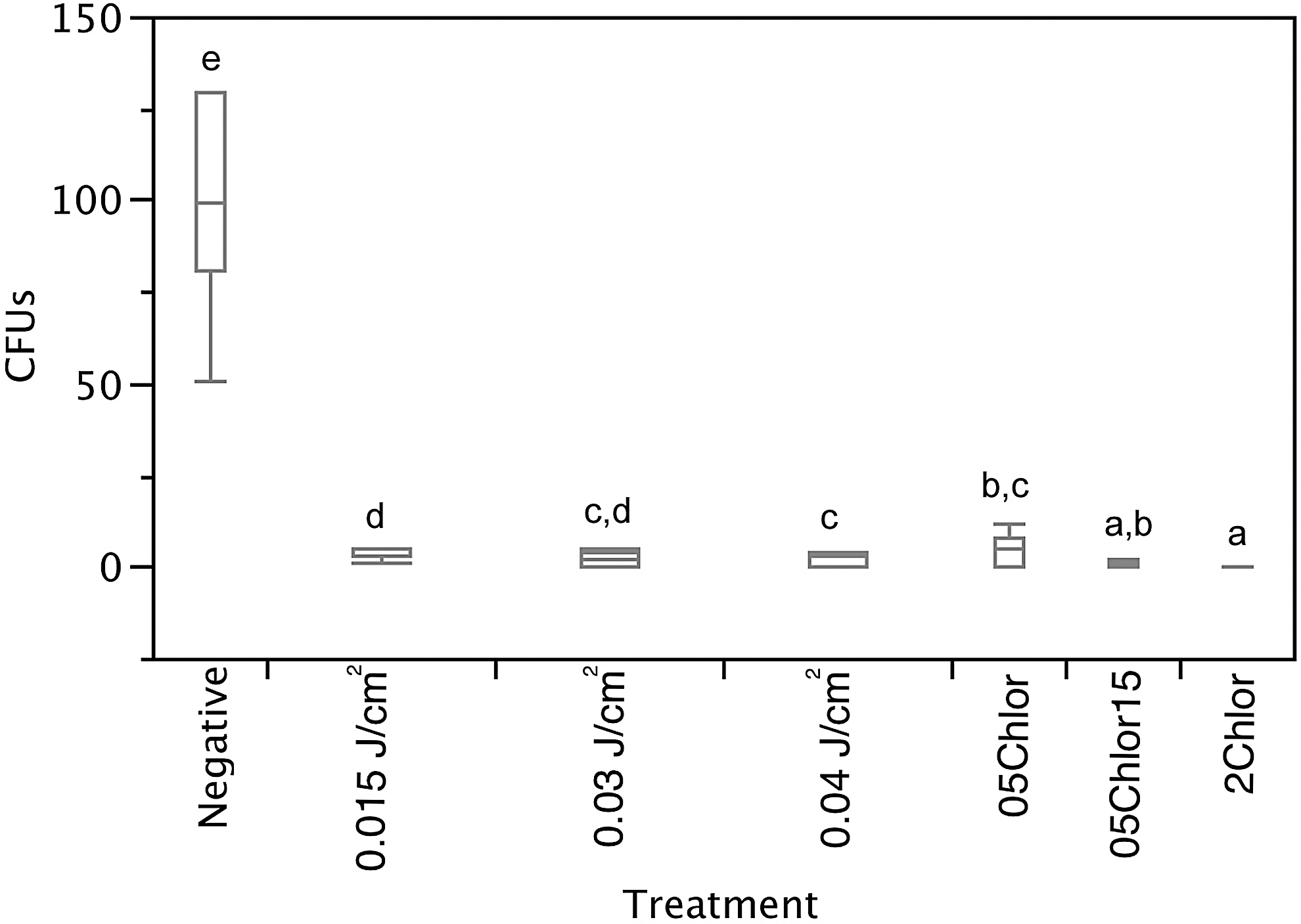
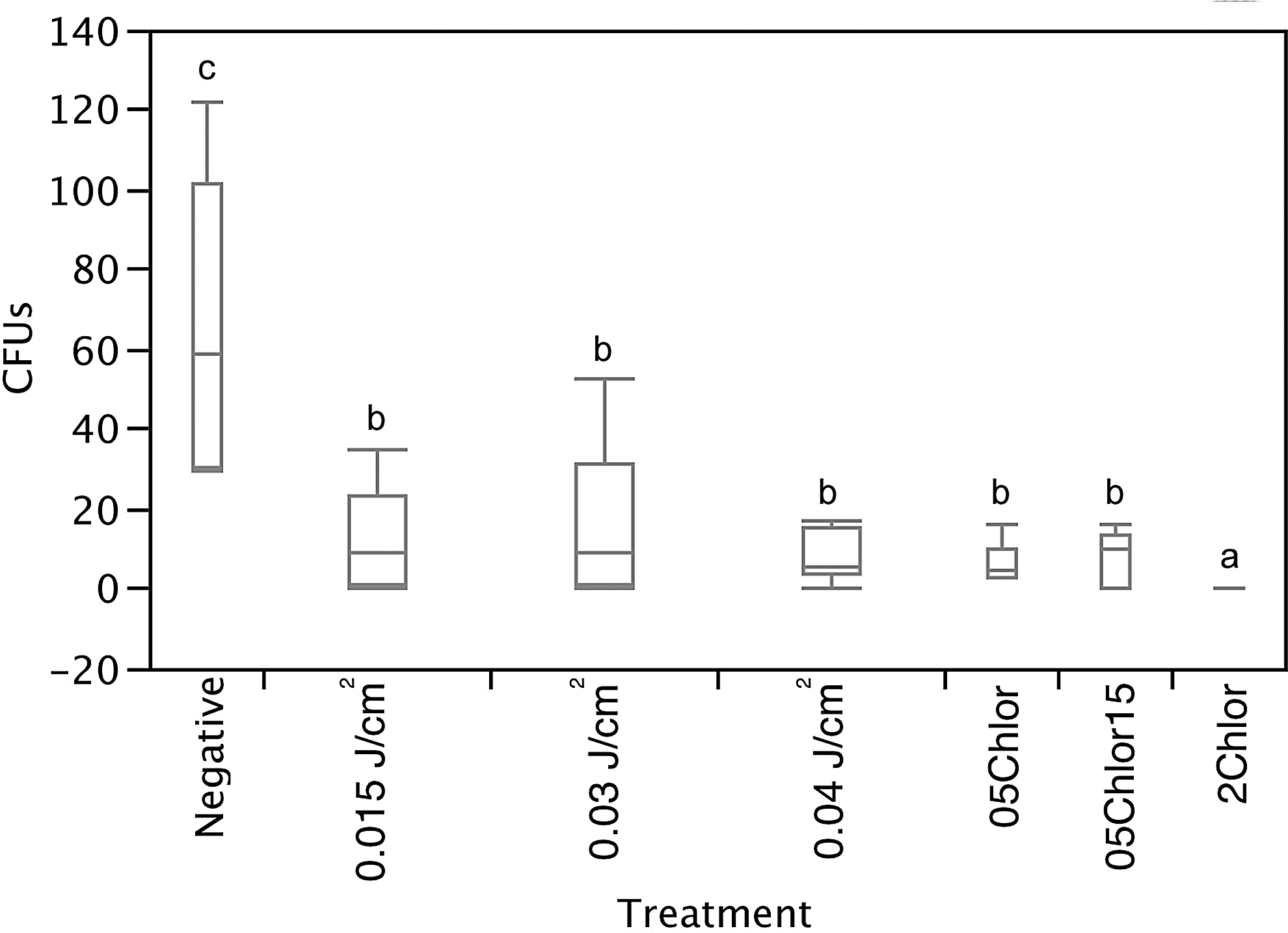
All treatments resulted in a significant decrease in CFU counts when compared with the negative control (Fig. 1). Two percent chlorhexidine resulted in lower CFU counts than other treatments (p < 0.03). Treatment with UVC at all doses resulted in significantly lower CFU counts than 0.05% chlorhexidine treatment (p = 0.01). There were no significant differences between UVC treatment doses.

Box plot of MRSA on skin samples. Different letters indicate statistical significance (p < 0.05). Negative, Negative Control; 05Chlor, 0.05% chlorhexidine; 05Chlor15, 0.05% Chlorhexidine and 0.015 J/cm2 Mercury Light; 2Chlor, 2% Chlorhexidine.
K. pneumoniae-inoculated skin
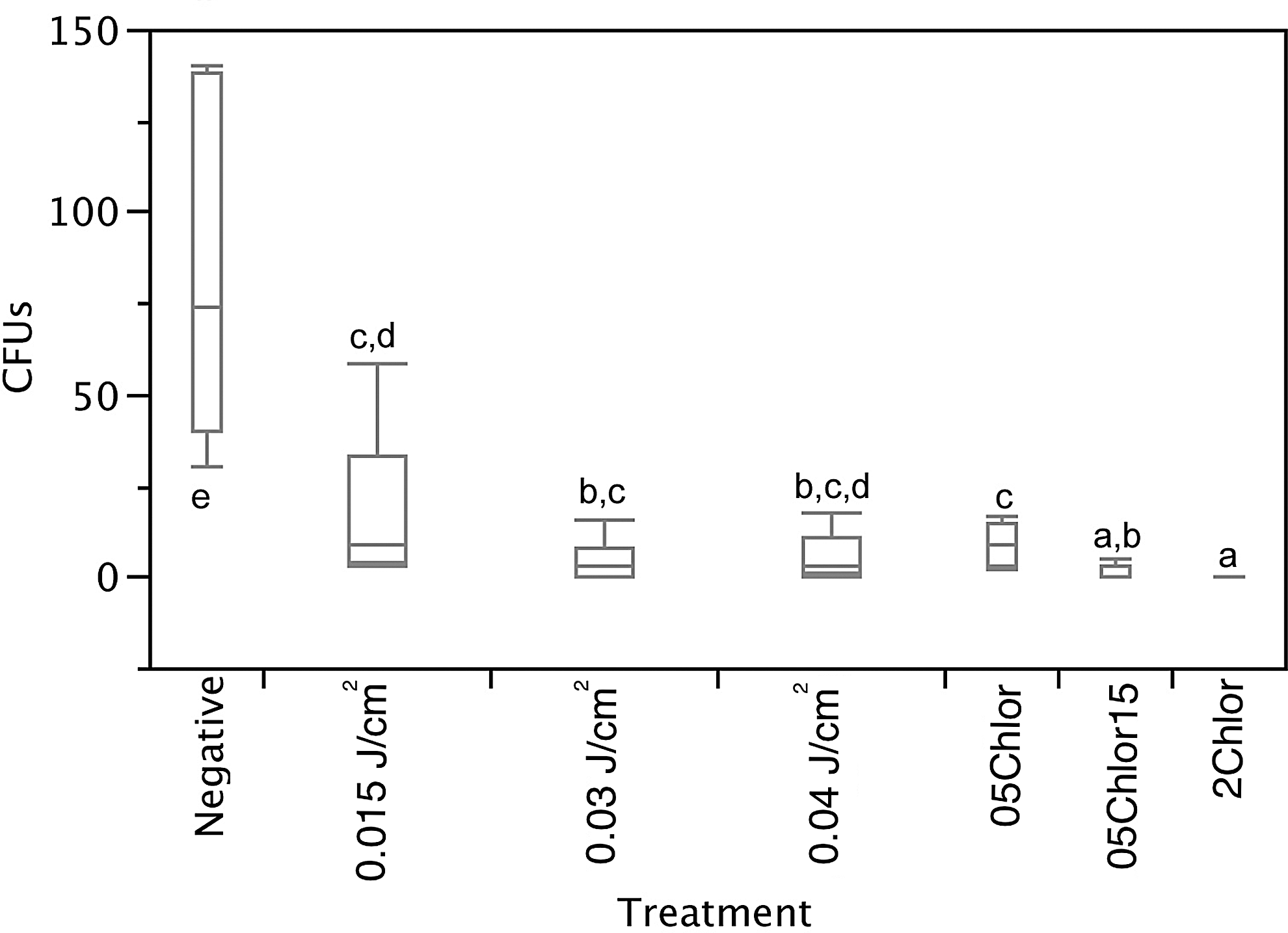
All treatments resulted in significantly lower CFU counts when compared with the negative control (Fig. 2). Two percent chlorhexidine treatment resulted in lower CFU counts compared with other treatments (p < 0.03), except for comparison against 0.05% chlorhexidine combined with 0.015 J/cm2 (p = 0.176). The 0.04 J/cm2 treatment outperformed the 0.015 J/cm2 UVC dose (p = 0.0089). The combination of 0.05% chlorhexidine with 0.015 J/cm2 resulted in lower CFU counts than treatment with 0.015, 0.03, or 0.04 J/cm2 of UVC (p < 0.05).
Box plot of Klebsiella pneumoniae on skin. Different letters indicate statistical significance (p < 0.05).
E. faecium-inoculated skin
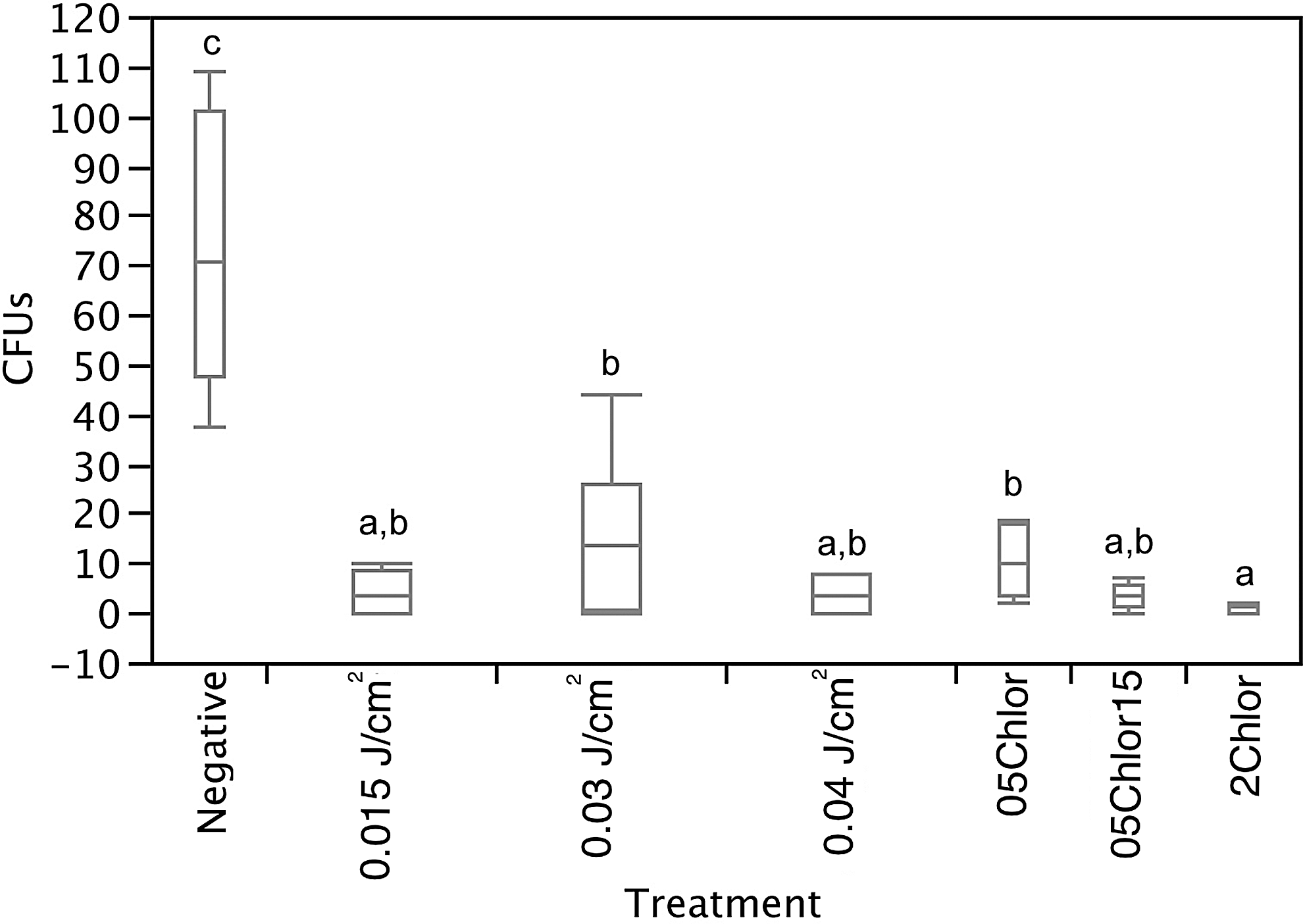
All treatments resulted in a significant decrease in CFU counts when compared with the negative control (Fig. 3). For all samples, 2% chlorhexidine treatment resulted in significantly lower CFU counts when compared with other treatments (p < 0.01), except for comparison against 0.05% chlorhexidine combined with 0.015 J/cm2 of UVC (p = 0.18). The 0.03 J/cm2 UVC treatment resulted in lower CFU counts than the 0.015 J/cm2 treatment (p = 0.03); 0.05% chlorhexidine combined with 0.015 J/cm2 resulted in lower CFU counts than the 0.015 J/cm2 or 0.05% chlorhexidine treatments (p = 0.01 and p = 0.044, respectively).
Box plot of Enterococcus faecium on skin Different letters indicate statistical significance (p < 0.05).
Methicillin-resistant S. aureus-inoculated muscle
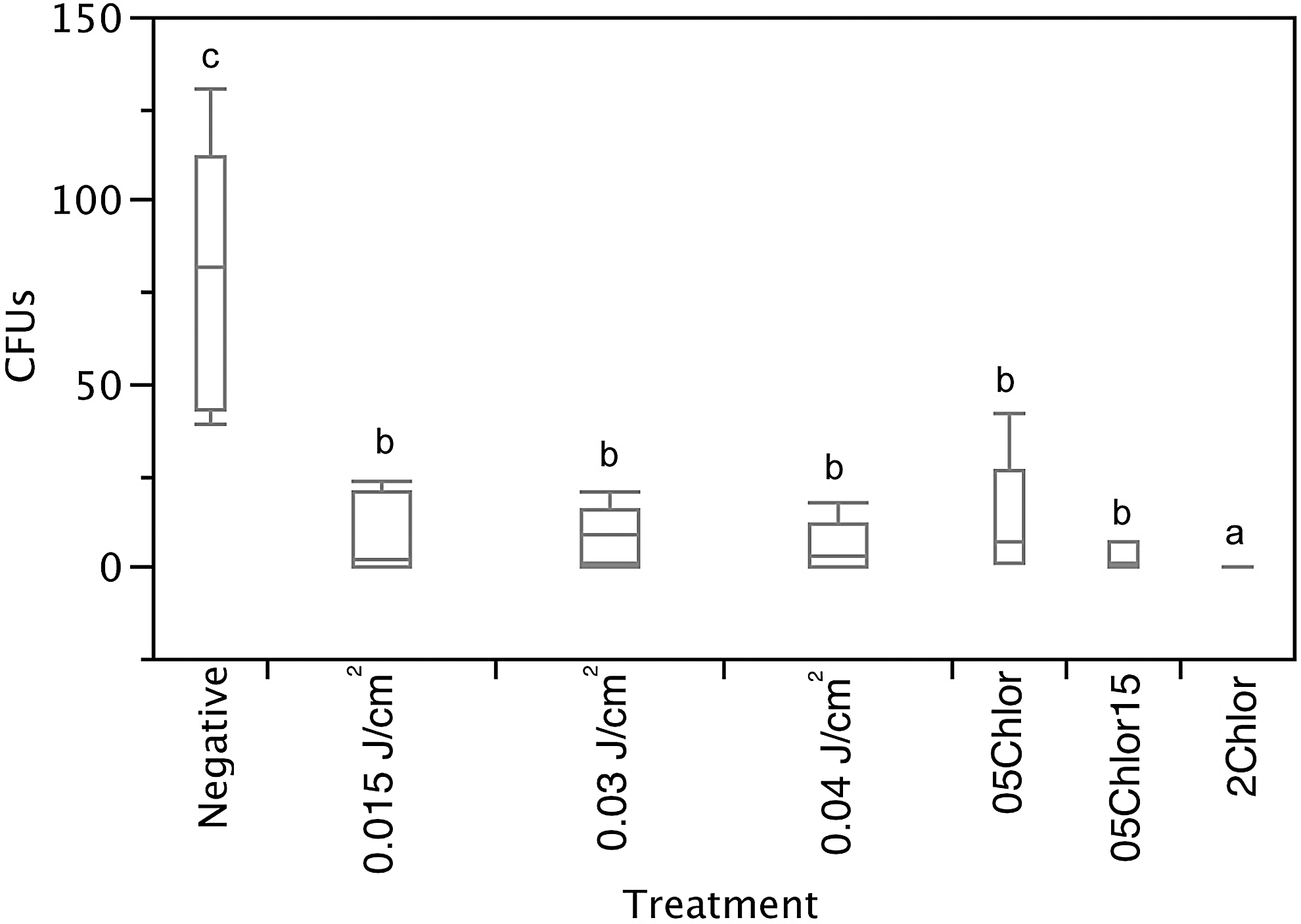
All treatments resulted in lower CFU counts when compared with the negative control (Fig. 4). Two percent chlorhexidine resulted in significantly lower CFU counts when compared with 0.05% chlorhexidine and 0.03 J/cm2 of UVC exposure (p = 0.0147 and p = 0.046, respectively). There were no other significant differences between treatments.
Box plot of MRSA on muscle. Different letters indicate statistical significance (p < 0.05).
K. pneumoniae-inoculated muscle
All treatments resulted in a significant decrease in CFU counts when compared with the negative control (Fig. 5). For all samples, 2% chlorhexidine treatment resulted in significantly lower CFU counts than other treatments (p < 0.03). No other significant differences were appreciated between treatments.
Box plot of K. pneumoniae on muscle. Different letters indicate statistical significance (p < 0.05).
E. faecium-inoculated muscle
All treatments resulted in a significant decrease in CFU counts when compared with the negative control (Fig. 6). For all samples, 2% chlorhexidine treatment resulted in significantly lower CFU counts than other treatments (p < 0.02). No other significant differences were appreciated between treatments.
Box plot of E. faecium on muscle. Different letters indicate statistical significance (p < 0.05).
Discussion
We have demonstrated effectiveness of low-dose UVC for reducing CFU counts of all ESKAPE pathogens analyzed in both canine skin and muscle, regardless of UVC wavelength. Further, we have demonstrated low-dose UVC treatment to result in significantly lower CFU counts of methicillin-resistant S. aureus and K. pneumoniae than 0.05% chlorhexidine treatment on canine skin. We have also demonstrated synergism between UVC and 0.05% chlorhexidine for reduction of E. faecium on canine skin. In this study, we compared our results with 0.05% and 2% chlorhexidine as it is widely considered an agent of choice when sterilizing skin or wound surfaces for surgical procedures. 21 –27 Chlorhexidine is a bisbiguanide with known bacteriostatic and bactericidal activity. 21 We felt this comparison would allow for a more clinically applicable evaluation of UVC. Our research is different from previous studies applying UVC for decreasing bacterial burdens, in that we were not using infected wounds and we deliberately were not trying to get a complete kill of the organism evaluated. Instead, our approach was focused in finding the lowest UVC dose able to decrease bacterial numbers such that an infection would be less likely to develop in a standard clinical setting. The use of low-dose UVC as an intraoperative and postoperative adjunct in surgical patients deserves clinical investigation. The use of low-dose UVC in muscle possessed equivalent bactericidal activity to that of 0.05% chlorhexidine and may be of more limited efficacy in tissues lacking an epidermal barrier. These findings suggest that it is possible to limit bacterial burdens using low-dose UVC on skin and muscle surfaces, making infection less likely. Limiting UVC exposure will limit any unwanted acute damage to the patient and minimize occupational exposure associated with heavy use, as might be the case for a healthcare provider.
UVC ranges between 254 and 270 nm had been previously shown to be more effective than other wavelengths in the UVC spectrum. 28 We suspected that a higher frequency might result in deeper penetration and therefore better activity. In our study, we did not appreciate a difference in effectiveness between wavelengths. One simultaneous advantage and disadvantage of UVC is that the short wavelength precludes it from deep penetration. This is advantageous from the standpoint of minimizing collateral damage, but is a limitation if bacteria cannot be reached within hair follicles or beneath organic debris. Deeper penetration may be advantageous in the presence of organic debris, but collateral damage to deeper structures would be a concern. Buonanno et al. showed less damage to human cells when exposed to 207 nm light versus 254 nm light. 20 Conversely, contaminated tissue bathed in blood has been shown to be less capable of being sterilized with 254 nm UVC. 29 Further studies evaluating host cell damage and penetration in biologically relevant tissues and clinical scenarios are indicated to determine optical wavelengths for a given clinical application.
The 254 nm light source was mercury based, while the 270 nm light source was LED based. Mercury lamps currently provide much higher power outputs than LED-based lights, allowing for application of the same dose in seconds compared with minutes for LED UVC. The higher the power output, the shorter the treatment time, making this highly desirable. The disadvantage of mercury lamps is that they require a warm-up time and will gradually deteriorate in power output over time, particularly when switched on and off frequently; ultraviolet deterioration occurs at a different rate than visible light, making regular photospectrometric assessment necessary. 30 As UVC has the potential to cause collateral damage, knowing the exact dose delivered is highly desirable. In comparison, LED UVC allows for instant on/off and there is slower expected power output deterioration over time. 31 It is the authors' opinion that although the power output of LED UVC is currently suboptimal and they are significantly more expensive, as their technology and demand evolve, they may replace mercury-based UVC sources. To our knowledge, this is the first study documenting the use of LED UVC technology on biological surfaces.
As of now, there is a scarcity of literature identifying the short-term and long-term effects of UVC use in a clinical setting. 32,33 Our results show that low-dose UVC has a similar or better immediate bactericidal effect to that of 0.05% chlorhexidine. We also show a trend toward synergism when UVC is combined with chlorhexidine. This may result in a higher safety index and more acceptance by the medical community. Recently studied doses are substantially greater than 8-h occupational exposure limits of 0.006 J/cm2. 33 For example, some studies have used doses of over 2.5 J/cm2. The doses used in this study are as much as 80 times less than previously reported doses on biologically relevant surfaces. 8,15 Of interest, these higher doses showed no short-term permanent damage; however, it seems reasonable to seek the lowest effective dose able to prevent SSIs.
Our combination treatment resulted in similar effectiveness to 2% chlorhexidine when treating K. pneumoniae and E. faecium on skin and MRSA on muscle. It is probable that sample size did not allow for a clear distinction in regard to the combination of chlorhexidine with UVC and 2% chlorhexidine in all treatments; future studies with larger sample sizes may resolve this. Chlorhexidine has been shown to reduce SSIs. 21 –27 Combination therapy may aid in decreasing diverse bacterial burdens when organisms may be more resistant to one modality over the other. Based on our results, especially in circumstances where the negative effects of concentrated chlorhexidine are clinically significant, further investigation of UVC sterilization is indicated. Chlorhexidine has been shown to be lethal to macrophages as well as osteoblastic, endothelial, and fibroblastic cell lines in a dose- and time-dependant manner. 22,34 –37 Similarly, chlorhexidine has recently received more attention for having decreased efficacy against some strains of bacteria 38 –42 and the use of UVC may be beneficial in these circumstances.
Although all treatments with UVC resulted in decrease in bioburden, there was not always a clear pattern. This highlights the potential complexity and limitations associated with UVC treatment. Factors that may have played a role in variation include, but are not limited to, surface topography, distance from treatment, presence of organic debris, wavelength, angle of incidence, and variability between samples within the same group. This study also has several limitations that should be noted. The methodology used is similar to what is used in a clinical setting and was consistent between treatment samples and controls. However, the recovery of bacteria may be considered suboptimal. Because of the limitations of the methodology, we specifically aimed to achieve similar efficacy to chlorhexidine using the same methodology, which would then infer success with UVC exposure. The in vitro nature precludes us from making definitive conclusions about the ability for low-dose UVC to successfully prevent SSIs. Not all pathogens implicated in SSIs were evaluated and it is likely some pathogens, such as Clostridium difficile, will be more resistant to UVC damage. 16 It is unknown at what time points or how frequently low-dose UVC might need to be used to achieve a protective effect. Our study involved the use of planktonic bacteria and did not specifically evaluate effectiveness against biofilms. Further, it is possible that chlorhexidine may have performed better over a longer study as it is known to have residual activity. 43 Type II sampling error may have also been present in this study.
Despite some of the limitations inherent to in vitro studies, our results demonstrate the promise of low-dose UVC to reduce bacterial bioburdens of multi-drug-resistant bacteria commonly implicated in SSIs. Currently, there is no easy, safe, synergistic, cost-effective, and scalable solution to prevent SSIs. 34 –37,44 Bacterial loads and routes of presentation play major roles in development of infections. Although there are significant variations and synergism that occur when there are multiple organisms present in a wound, in general, a burden of greater than 105 CFU/gr has been found to result in infection. 45,46
The UVC doses selected were not able to achieve complete eradication of the bacteria evaluated, and some may view the reduction in bacteria as marginal in comparison with other reported means of bacterial reduction. 8,10,47,48 We suggest that in most clinical settings, complete eradication is not necessary, nor desired. The aim in wound or incision management is to achieve a host manageable bioburden; it is not possible and considered suboptimal to produce a truly sterile wound environment. 45,46 Commensal skin flora are important in excluding more pathogenic bacteria and are typically more susceptible to antibiotics and some disinfectants than more pathogenic bacteria. 21,49 UVC exposure at the doses used had similar or better bactericidal activity than 0.05% chlorhexidine, which may imply efficacy in preventing SSIs. 50,51 UVC may represent a methodology for reducing bioburdens without selecting for pathogenicity. 52 It is important to note that we are not suggesting that UVC replace current practices in creating sterile surgical fields. Instead, we are looking to augment current gold standards to further reduce the incidence of SSIs. Reduction in bacterial loads using a 0.015 J/cm2 low dose of UVC merits additional exploration. Low dosing would minimize collateral damage. The surgical incision repair process can be divided into four overlapping phases: coagulation, inflammation, proliferation, and remodeling. 53 Wound strength is not present until 3–5 days after the initial incision in a healthy patient. Clinical investigation of the effect of UVC treatment at various stages of wound healing on SSI prevalence may provide options for improved patient outcomes.
Conclusions
In summary, we have demonstrated low-dose UVC to possess greater bactericidal efficacy against methicillin-resistant S. aureus and K. pneumoniae than 0.05% chlorhexidine on canine skin. We have also demonstrated synergism between UVC and 0.05% chlorhexidine against E. faecium on canine skin. The use of low-dose UVC as an intraoperative and postoperative adjunct in surgical patients deserves future clinical investigation.
Footnotes
Acknowledgments
The author would like to acknowledge Dr. Matthew Johnson, DVM, DACVS, and our surgical residents for their assistance with canine skin and muscle harvesting. This study was funded by the 2014–2015 Fall Consolidated Faculty Research Award Grant at the University of Florida College of Veterinary Medicine.
Author Disclosure Statement
No competing financial interests exist.