
Abstract
Introduction
E
A bipolar fractional radiofrequency (FRF) system, which was developed to overcome these limitations, creates microscopic zones of thermal damage, and the regions of damaged skin tissue are interspersed with areas of intact skin tissue. 2 This approach has been found to have significant beneficial effects in the treatment of atrophic ASs or acnes. 2,3 However, to our knowledge, no clinical or histological study has examined the long-term efficacy and safety of bipolar FRF therapy as a treatment for atrophic ASs and active acne in people with darker skin.
Materials and Methods
After institutional ethics committee approval and written informed consent, eight Japanese patients (two males and six females; median age of 29.9 years) with atrophic facial ASs and mild-to-severe acne vulgaris were surveyed from April 2013 to August 2015, using the Investigator Global Assessment. 1
Exclusion criteria were as follows: administration of any topical or oral antibiotic, retinoid, corticosteroid agent, or oral contraceptive pill or any aesthetic acne or AS treatment during the study or the prior 6 months; pregnancy; a history of keloid scarring; and the presence of an electrical implant such as a pacemaker anywhere in the body.
All eight patients underwent five treatment sessions, with a 1-month interval between each session. Patients used a topical anesthetic cream applied 30 min before treatment. Then, they were administered bipolar FRF (eMatrix™; Syneron) treatment on both cheeks in the most ablative mode with constant settings (coverage rate: 10%; peak energy: 62 mJ/pin; two passes) with a disposable single-use treatment tip consisting of a total of 64 pins (pin diameter: 200 μm) in a 12 × 12 mm area with an air cooler. The pins on the tip were arranged in alternating rows of positive and negative electrode pins. Epidermal disruption occurs over less than 5% of the surface, which is influenced by the length and diameter of each pin. 2 We recommended the use of moisturizing cream and sunscreen on the day after treatment and instructed the subjects to avoid sun exposure.
Treatment efficacy was assessed using a five-point scale measuring overall improvement for ASs and acne (≥25% worse = recurrent or worse, 0–24% improvement = no change, 25–49% improvement = fair, 50–74% improvement = good, and 75–100% improvement = excellent) at each visit and at least 1 year after the last treatment through a blinded photographic evaluation by two dermatologists. For histological analysis, 4-mm punch biopsies of the cheek were performed at baseline and at 3 months after the final treatment, and subjected to routine hematoxylin–eosin, elastica van Gieson, and Masson's trichrome staining.
Results
Results and patient data are listed in Table 1 and Fig. 1. Most subjects had Fitzpatrick skin types III–IV. The initial Investigator Global Assessment of the patients' acne lesions classified five (62.5%) as mild, one (12.5%) as moderate, and two (25.0%) as severe. As for the initial AS grade, three (37.5%) had mild ASs, three (37.5%) had moderate ASs, and two (25.0%) had severe ASs. Patients received an additional assessment with an average follow-up time of 1.5 years (ranging from 1 to 2 years). One month after the last treatment, the acne lesions were “Excellent” in seven patients (87.5%) and “Fair” in one (12.5%), whereas the AS lesions were “Excellent” in two patients (25.0%), “Good” in two (25.0%), “Fair” in two (25.0%), and “No change” in two (25.0%) (Fig. 1). Three months after the last treatment, 25.0% (two out of eight) of patients experienced a flare-up of their acne lesions, ASs returned, and their acne became more severe. Additional acne treatments were required. By the end of the study, the treatment had caused a marked improvement in the severity of mild ASs in two (25.0%) patients.
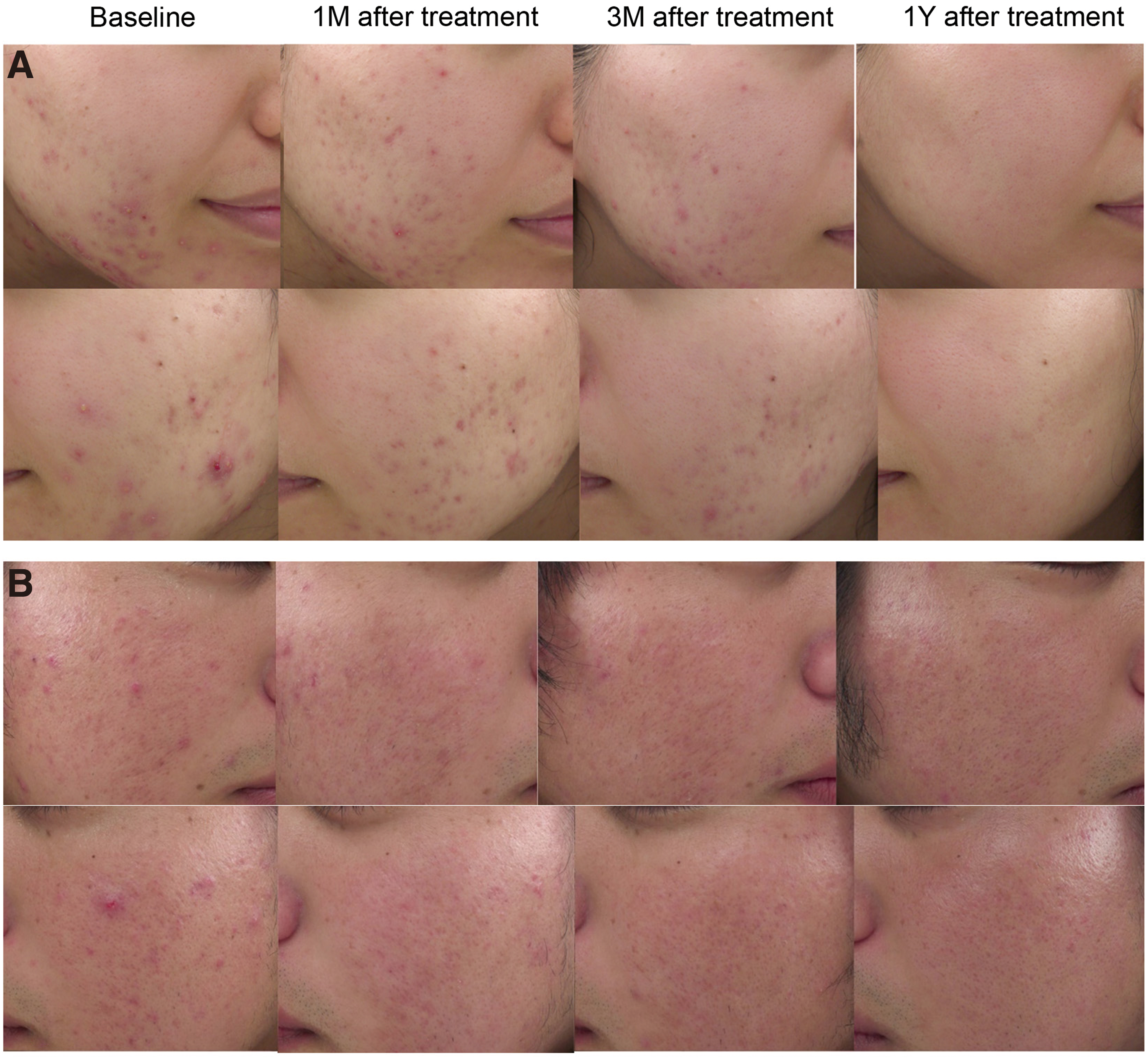
Atrophic acne scars and active acne. Clinical photographs of a 24-year-old female patient (Case 5) with a mild acne scar and severe acne
F, female; M, male; NC, no change.
Most participants reported transient and mild post-treatment erythema, swelling, scaling, and pain, but all of the participants tolerated the treatment well. Although dry skin was experienced by two (25.0%) patients, no significant side effects such as bullae, pigmentary complications, or scarring were observed during or after the treatment. No systemic adverse events were reported.
Before treatment, five out of eight (62.5%) subjects were found to have horny plugging of their hair follicles, and moderate infiltration of their lymphocytes and neutrophils. There was a mild loss of collagen and elastic fiber in the upper dermis as well as insufficient dense collagen fiber deposition in the deep dermis (Fig. 2A–C). The biopsy specimens taken after the completion of treatment showed a marked improvement characterized by a decrease in dermal pilosebaceous units, perivascular inflammatory cell infiltrates, and vasculature and an increase in elastin content and collagen deposition in the upper dermis (Fig. 2D–F).

Histopathological findings of the bipolar fractional radiofrequency therapy-treated side from Case 4. (
Discussion
Acne vulgaris is a disorder characterized by increased sebum production, keratinocyte proliferation of follicle epithelium, and follicular colonization with Propionibacterium acnes. 1 These manifestations are the main targets of treatment. Acne vulgaris can result in a variety of atrophic ASs depending on the depth and severity of the inciting inflammation. The involvement of the reticular dermis can result in “ice pick” scars, “boxcar” scars, and “rolling” scars. 1 As atrophic ASs involve atrophication and fibrosis, new collagen production and remodeling are considered to improve the appearance of ASs.
A variety of fractional photothermolysis (FP) lasers are now available, and ablative FP lasers are more effective at treating ASs than nonablative FP lasers. However, ablative FP lasers may also carry a greater risk of side effects. 4 Radiofrequency radiation is a form of nonionizing electromagnetic radiation with a frequency range of 3 kHz to 300 GHz. In contrast to most lasers that target specific chromophores, radiofrequency radiation is affected by the electrical properties of the target tissue and is chromophore independent. Thus, it is expected to be safer for all skin types. 5
We demonstrated that mild ASs responded better than moderate and severe ASs, and at least 50% improvement in scar severity was seen in 50.0% (four out of eight) of patients 1 month after the completion of the five treatment sessions. Six (75.0%) patients remained disease free 1.5 years after treatment without having received any additional therapy. Because the severe scars involving the subcutaneous region, such as the deep ice pick and boxcar type scars, were resistant to treatment, severe scars are most in need of focal trichloroacetic acid peeling or punch excision, possibly combined with bipolar FRF treatment. 1
Cannarozzo et al. treated five atrophic AS patients with Fitzpatrick skin type III with a new fractional CO2 laser device that adds bipolar radiofrequency to enhance its therapeutic efficacy. 6 Four out of five (80.0%) patients showed very good or excellent improvement after three sessions, with no severe side effects; efficacy was better than in our study (50.0%). Further controlled studies to compare the bipolar RF combined fractional laser and bipolar FRF devices are needed in people with darker skin.
In our previous study of atrophic ASs, we observed the thermal denaturation of peri-hair follicle collagen, hair follicles, and sebaceous glands. 7 Omi et al. reported remodeling of the dermis to replace AS-associated morphological and ultrastructural irregularities with a more normal architecture, particularly in the case of elastic fibers and over deposition of elastin. 8 Histological changes occurring 3 months after the bipolar FRF treatment, including a substantial reduction of pilosebaceous units, dermal inflammatory cell infiltrates, vasculature, and an increase in elastin content and collagen deposition in the upper dermis, are thought to contribute to the clinical outcomes of patients with ASs and acne.
The main limitations of our study were the small number of participants and absence of a control group.
In conclusion, the findings of this study suggest that bipolar FRF treatment is effective over the long term against mild atrophic ASs and mild-to-moderate acne in Japanese patients with minimal side effects. For severe ASs and acne, FRF treatment should be used in combination therapy for the synergistic effects.
Footnotes
Acknowledgment
This study was funded by JMEC Co., Ltd. (Tokyo, Japan).
Authors' Contribution
The sponsor of the study had no role in the study design, conduct of the study, data collection, data interpretation, or preparation of the report. This study was approved by the Human Research Protection Program of Wakayama Medical University (1088).
Author Disclosure Statement
No competing financial interests exist.