
Abstract
Introduction
R
Methods to remove root canal filling include mechanical, chemical, and thermal techniques. 6 Currently, the mechanical removal of root canal filling materials with rotary NiTi files is preferred in relation to the use of hand files and solvents. 7 The use of rotary NiTi files was reported to be superior to manual instrumentation for removal of the bulk of the filling. 8 However, all retreatment techniques have been shown to fail to render the root canal wall completely free of residual filling material, 9 and commonly used irrigation solutions are ineffective as solvents for residual epoxy resin-based sealers on root canal walls. 10
Therefore, various additional procedures, such as ultrasonic systems, lasers, and photon-induced photoacoustic streaming (PIPS), have been suggested and found effective in minimizing root filling residue on root canal walls. 11 –13 Neodymium-doped yttrium aluminum garnet (Nd:YAG) and erbium-doped yttrium aluminum garnet (Er:YAG) lasers have been utilized with various purposes in endodontics. Er:YAG laser systems have been reported to have lower thermal effects on tooth's surrounding structures when compared with Nd:YAG lasers. The photoablative effect of laser irradiation on dentin has been shown to improve material removal during retreatment. 14 The self-adjusting file (SAF; ReDent-Nova, Ra'nana, Israel) was proposed as a second-stage instrument in retreatment due to its scraping motion with simultaneous irrigation, which was considered to improve debridement of the root canal surface. 15 –17 Similarly, passive ultrasonic irrigation (PUI) was also advocated for use in retreatment procedures due to the superior debridement effect of acoustic streaming. 15
Retreated teeth were reported to exhibit lower fracture resistance than initially treated teeth, and decreased fracture resistance was correlated with increased loss of root dentin. 18 Retreatment procedures often require further mechanical preparation, and additional procedures might also cause damage to root canal dentin. The efficacy of additional retreatment procedures is well defined, whereas, to our knowledge, the effect of these procedures on fracture resistance of roots has not yet been addressed. The aim of this study was to compare the fracture resistance of roots after the additional use of SAF, PUI, PIPS, Er:YAG, or Nd:YAG lasers following root canal filling removal with R-Endo retreatment files.
Materials and Methods
Specimen selection
The study design was approved by the medical faculty's ethics committee (Protocol No: 109). Straight, single-rooted, mandibular canine teeth extracted for periodontal reasons were selected and radiographed in buccolingual and mesiodistal directions with an X-ray device (Belmont Phot-X II; Takara Belmont Corp., Osaka, Japan) at 60 kVp and 4 mA. Teeth showing previous root canal treatment, more than one root canal, open apex, calcification, and/or resorption were excluded. The ratio between the long and short diameters of the root canal was calculated using the ImageJ program (1.44p; National Institutes of Health, Bethesda, MD), and those teeth with a 2 × or 3 × long-to-short ratio were included for use in the study. A total of 117 teeth were selected and randomly divided into nine experimental groups (n = 13). Following a check for normality assumptions (Shapiro–Wilk test), the degree of homogeneity (baseline) of the nine groups with respect to root canal ovality was confirmed using a one-way ANOVA test, with a confidence level set at 5%. Specimens were disinfected in 0.1% thymol solution and stored in distilled water containing plastic vials at 4°C until use.
Group 1 was assigned as control group. The specimens in this group did not receive any treatment, whereas root canals were prepared in all the other groups.
Root canal preparation
Following preparation of endodontic access cavities using high-speed diamond burs (SybronEndo, Orange, CA) under water cooling, the working lengths (WLs) were determined by subtracting 1 mm from the length at which the No. 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) first appeared at the apical foramen. To facilitate endodontic access cavities as reservoirs for laser activation, the specimens were not decoronated.
An experienced operator mechanically prepared the root canals using a Revo-S NiTi rotary file system (MicroMega, Besançon, France), which comprises one recapitulating and cleaning instrument (SU) and two apical penetrating instruments (SC1 and SC2). Preparation was performed in a crown-down manner using an endodontic motor (W & H, Bürmoos, Austria) set at 300 rpm. Following preparation of the apical third to a size 25, 0.06 taper, apical preparation files (AS 30, 35, and 40) were used up to the WL. Apical preparation was completed with the use of a manual No. 45 K-file (Mani Co., Tokyo, Japan). The root canals were flushed with 20 mL of 2.5% NaOCl between each file change using disposable syringes with a 30-G NaviTip needle (Ultradent, South Jordan, UT) inserted 1 mm short of the WL. The final irrigation was achieved using 5 mL of 17% EDTA (pH = 7.7) for 1 min, followed by 5 mL of bidistilled water at 1 mL/min for 5 min. Finally, the root canals were dried with sterile paper points (Dentsply Maillefer).
For Group 2, the treatment ended here; all groups, except Groups 1 and 2, next received the root canal filling.
Root canal filling
A warm vertical compaction technique using the BeeFill 2 in 1 system (VDW, Munich, Germany) was used for the root canal filling. First, the root canal walls were coated with a thin layer of AH Plus sealer (Dentsply De-Trey, Konstanz, Germany), then gutta-percha master cone showing 45 apical size and 0.02 taper (Aceone-Endo; Aceonedent Co., Geonggi-Do, Korea) was inserted to full WL. The apical third of the root canal was obturated with a BeeFill down-packing device, while the coronal and middle thirds were obturated with a BeeFill back-filling device. The quality of root canal fillings was confirmed with radiographs, which were taken in both mesiodistal and buccolingual directions. The specimens were stored at 37°C at 100% humidity for 1 week to enable complete setting of the sealer.
Group 3 received no further treatment after the filling; the remaining (experimental) groups received different retreatment procedures.
Root canal retreatment and treatment of experimental groups
R-Endo NiTi rotary retreatment files (Micro-Mega, Besançon, France) driven by a torque-controlled motor (W & H) set to 340 rpm were used to perform the retreatment procedures. Re files (15 mm, size 25, 0.08 taper) were used at the 3 mm coronal third, R1 (15 mm, size 25, 0.08 taper) at the beginning of the middle third, R2 (19 mm, size 25, 0.12 taper) at the middle third, and R3 (23 mm, size 25, 0.04 taper) at the apical third; No. 45 K-files were used up to the WL. Irrigation with 2.5 mL of 5% NaOCl was performed between each procedure. Retreatment instruments were discarded after four canals, and retreatment was considered completed when no root canal filling material was detected between the flutes of the file and the final irrigation solution rinse appeared to be free of debris. The apex was sealed with wax to prevent extrusion of irrigation solutions and simulate a closed-ended canal system to create a vapor lock effect. The 117 specimens were randomly assigned to nine experimental groups (n = 13).
Group 1 (control group)
Root canals were not instrumented and not filled.
Group 2 (prepared group)
Root canals were instrumented, but no root canal filling was performed.
Group 3 (filling group)
Root canals were instrumented and root canal fillings were performed, but no further procedures were performed.
Group 4 (R-Endo group)
Root canals were instrumented only with R-Endo and irrigated with 5 mL of 17% EDTA for 1 min and then 5 mL of 5% NaOCl for 1 min.
Group 5 (R-Endo+SAF group)
Following the retreatment procedure with R-Endo, a 2.0-mm diameter SAF (ReDent-Nova) was operated with in-and-out motion to WL for 2 min using a vibrating handpiece RDT3-NX head (ReDent-Nova) adapted with a low-speed handpiece (NSK, Tokyo, Japan) at a frequency of 5000 movements per minute and amplitude of 0.4 mm. Continuous irrigation with 17% EDTA at a flow rate of 5 mL/min for 1 min was followed by 5% NaOCl irrigation for 1 min, applied using a special irrigation device (VATEA; ReDent-Nova). The canals were dried with paper points.
Group 6 (R-Endo+PUI)
Following the retreatment procedure with R-Endo, a noncutting ultrasonic tip (miniMaster; EMS, Nyon, Switzerland) mounted in a piezoelectric unit (EMS) was inserted into the canals 1 mm short of the WL. The tip was directed to the apical third with a frequency of 30 kHz in the endomode as per the manufacturer's instructions. Oscillation of the tip directed to the apical third with irrigation was initiated at the same time. Ultrasonic irrigation was completed for a total of 2 min, using 5 mL of 5% NaOCl for 1 min and a continuous flow of 5 mL of 17% EDTA for 1 min. The canals were irrigated with 2.5 mL of distilled water and dried with paper points.
Group 7 (R-Endo+Er:YAG group)
Following the retreatment procedure with R-Endo, the root canals were irradiated with an Er:YAG laser (2940 nm, Fidelis AT; Fotona, Ljubljana, Slovenia) at 1 W, 20 Hz, and 50 mJ per pulse in the very short pulse mode (VSP) delivered with a 14-mm-long optic fiber plain tip (Ø = 300 μm). The tip of the optic fiber was inserted into the canal 3 mm short of the WL and activated. Then, the fiber tip was gently withdrawn from the apical to coronal region with a helical movement and reintroduced to the apex. The laser unit air and water sprays were set to off and root canals filled with 5% NaOCl solution. Ten-second intervals of laser-activated irrigation were followed by 10 sec of rest in between. The application was completed at six intervals for a total of 60 sec, using 5 mL of 5% NaOCl. Then, the same irrigation protocol was applied using 17% EDTA. After the laser application, a final rinse was performed with 15 mL of distilled water.
Group 8 (R-Endo+Nd:YAG group)
Following the retreatment procedure with R-Endo, an Nd:YAG laser (1064 nm; Fotona) at 1 W, 20 Hz, and 50 mJ per pulse in the VSP mode was delivered with an optic fiber plain tip (Ø = 320 μm). Irradiation and irrigation were performed as described in Group 7.
Group 9 (R-Endo+PIPS)
Following the retreatment procedure with R-Endo, irradiation with an Er:YAG laser (2940 nm; Fotona) at 1 W, 20 Hz, and 50 mJ per pulse in the VSP mode was delivered with a 14-mm-long tapered PIPS fiber tip (Ø = 300 μm), which was inserted at the access cavity, remaining stationary during the procedure. Again, the irrigation protocol was performed as for Group 7.
Preparation for Instron testing
The teeth were decoronated using a high-speed saw under constant water cooling (Isomet 5000; Buehler, Lake Bluff, IL). The specimens were mounted vertically on custom-made acrylic blocks exposing 3 mm of the coronal part, while the rest was embedded in the resin (Caulk/Denstply, Milford, DE). The acrylic resin was allowed to polymerize for 1 h. Vertical alignment of the long axis of the tooth was ensured with a protractor. Resin blocks were stored in 100% humidity until Instron testing.
A previously described technique by Sedgley and Messer was applied for vertical loading to fracture. 19 A cone-shaped rod was mounted on an Instron tester (Instron, Canton, MA) directly over the specimens (Fig. 1). The Instron tester applied a constant slowly increasing force at a crosshead speed of 1.0 mm/min until the tooth fractured. Fracture was defined as the point at which the computer monitor showed a sharp drop in force and a crack was heard. The test was terminated at this point and the applied force recorded and measured (in Newtons).
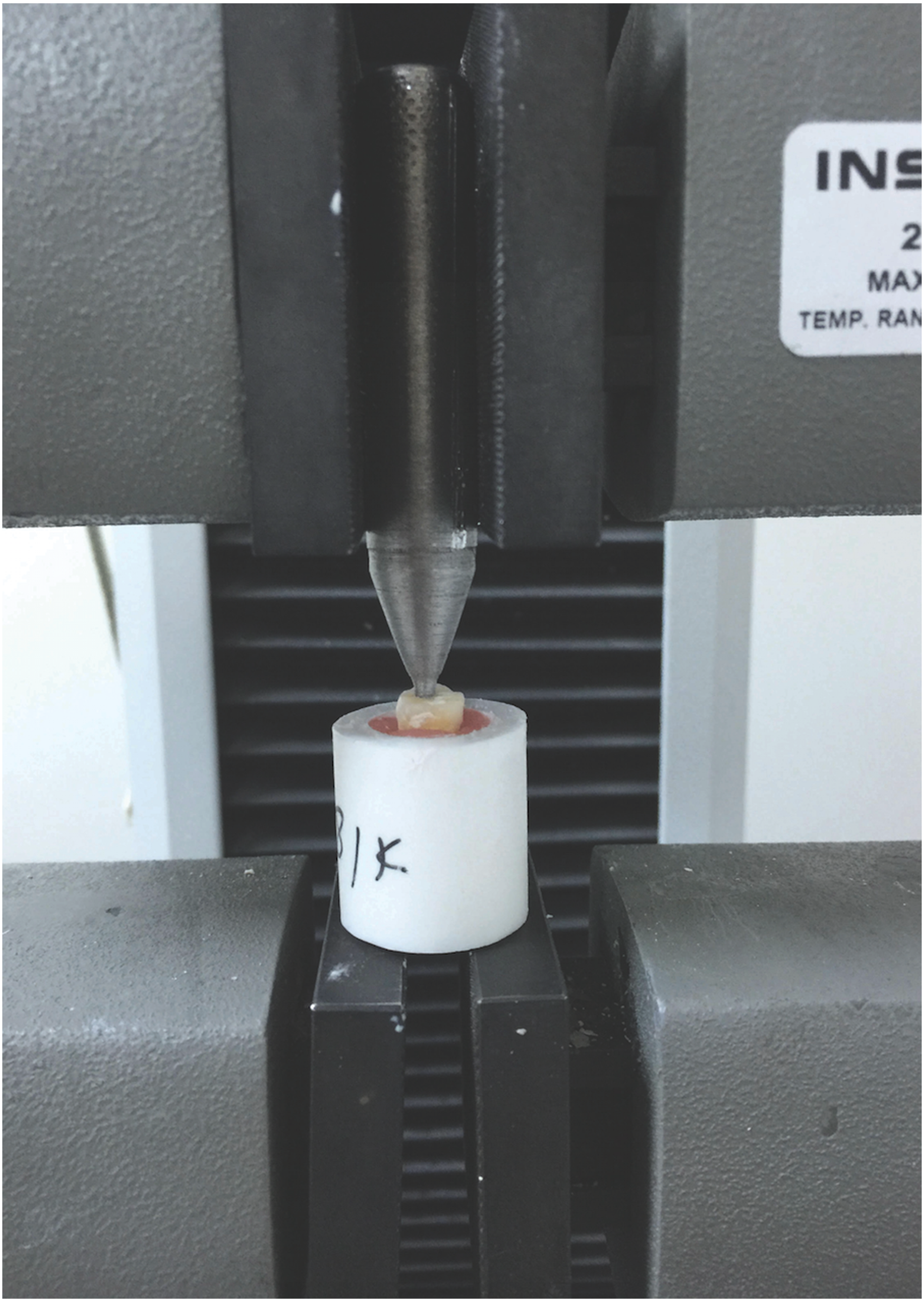
Vertical fracture strength test apparatus.
Statistical analysis
Statistical analysis was performed using a normality test of Shapiro–Wilk and one-way ANOVA test to evaluate differences among the nine experimental groups. The significance between groups was further tested with a Duncan test. The significance level was set at 5%.
Results
Box plot (Fig. 2) shows the results for fracture strength of Groups 1–9. The three groups that did not receive any retreatment procedure—Groups 1 (control), 2 (prepared), and 3 (filled)—exhibited a significantly higher fracture resistance than the other experimental groups, which received the retreatment procedure (Groups 4–9) (p < 0.05) (Table 1). The highest fracture resistance was detected in Group 1 (control group) and the lowest in Group 9 (R-Endo+PIPS). The one-way ANOVA test revealed no statistically significant difference among Groups 4–9 (p > 0.05).
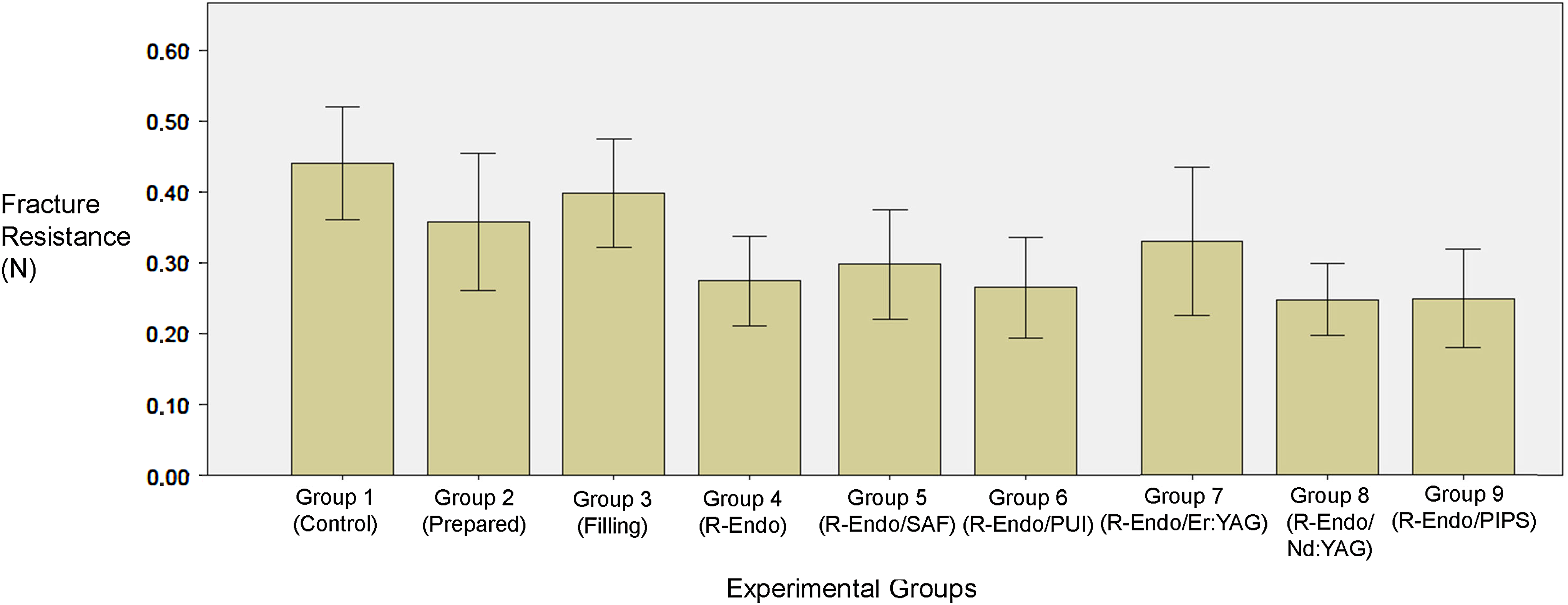
Box plot graphic comparing the vertical fracture strength values of Groups 1–9.
Different lowercase letters indicate statistically significant differences among tested groups.
Discussion
Endodontic and restorative procedures have been reported to affect dentin's mechanical properties, such as microhardness, elasticity, and fracture resistance. 20,21 Endodontically retreated teeth have been reported to have decreased resistance to fracture as a result of root dentin loss during root canal filling removal and further cleaning and shaping procedures. The finding of this study was consistent with those of a previous study reporting decreased fracture resistance of retreated roots. 18 Therefore, several factors should be considered for material selection to fill and disinfect retreated root canals. Additional retreatment procedures, including PIPS, Er:YAG laser, Nd:YAG laser, SAF, and PUI, have been suggested to enhance the efficacy of root canal filling removal, 11 –16 but the effect of these procedures on reinstrumented root dentin has not yet been investigated. During retreatment, clinicians should choose and apply a disinfection protocol that will not weaken tooth structure any further.
An interesting finding of this study was that there was no significant difference between the R-Endo group and additional laser application groups, including PIPS, regarding fracture resistance of roots. To authors' knowledge, there are no relevant available data for a direct comparison with previous literature. Nd:YAG laser irradiation is absorbed by mineral structures, such as hydroxyapatite, phosphate, and carbon, resulting in crystal disorder and melting on the dentin surfaces and also on the filling remnants (thermochemical ablation). 13,22 The effect of Nd:YAG laser irradiation on the mineral content of root dentin has been investigated and a decrease in calcium and phosphor levels reported. 23 Nd:YAG laser is absorbed by protein, pigmented tissue, and dark surfaces and it is poorly absorbed by water. 24 Er:YAG laser irradiation results in the formation of an empty space in liquid bubbles, followed by cavitation, 25 whereas in the PIPS technique, each impulse of subablative energy creates expansion of water molecules and cascade of shock waves leading to streaming without causing any heating effect. 26 Another study compared the effects of the Er:YAG and Nd:YAG laser systems and reported no significant alteration in the compositional structure of the dentin surface. 27 In the present study also, the laser systems and parameters employed appear not to have promoted an ultrastructural alteration in root dentin, which might affect the fracture resistance.
PUI relies on transmission of ultrasonic energy through an endodontic file to the endodontic irrigant, creating acoustic streaming and cavitation. 28 PUI activation of EDTA and NaOCl solutions for 1 min per solution has been reported not to alter the mineral level of root dentin surface. 29 To our knowledge, however, there is no study regarding the effect of PUI on fracture resistance of roots, therefore direct comparisons cannot be made as indicated above.
The SAF system is designed to adapt root canal configuration and promote continuous irrigant flow. The adaptive properties of SAF eliminate the risk of overpreparation and weakening of root structures. A literature search revealed no data on the effect of SAF on fracture resistance, although its effects on root canal walls are well studied; 1.5 mm SAF caused no crack in root dentin, 30 whereas 2.0 mm SAF caused incomplete cracks, but lower cracked teeth. 31 A vibrating in-and-out movement and continuous irrigant flow during operation have been correlated with low pressure on root dentin. It has been suggested that 2.00 mm SAF applies more pressure than does 1.5 mm SAF and that the higher pressure causes dentin damage. 31 In the present study, the use of 2.00 mm SAF following retreatment procedures did not affect the fracture resistance of root dentin.
In the present study, several factors were as standardized as possible by including the same type of teeth, standardized root lengths, and same chemomechanical preparation and obturation protocols were followed. Using human teeth as specimens not only reflects clinical conditions but also presents large uncontrollable anatomic variations, such as age of specimens. Another limitation of the present study was the absence of cycling loadings and aging processes.
Within the limitations of the present study, the use of Nd:YAG or Er:YAG laser irradiation, PIPS, SAF, or PUI as additional methods following removal of root canal filling with the R-Endo system to improve cleaning of root canal walls was not found to significantly decrease the fracture resistance of root dentin. Therefore, these additional disinfection protocols might be considered and suggested as safe procedures for retreatment.
Footnotes
Acknowledgments
This study was supported by the Scientific and Technological Research Council of Turkey-TUBİTAK (Grant No.114S052).
Author Disclosure Statement
No competing financial interests exist.