
Abstract
Introduction
F
Periodontal diseases are often described in FA patients. 4 –6 Periodontitis results from inflammation of supporting structures of the teeth in response to chronic infections caused by various periodontal pathogenic bacteria. Inflamed periodontal pockets could contain as many as 400 species of colonizing microorganisms. 7 Subgingival biofilms in inflamed periodontal pockets can serve as a reservoir from which the bloodstream is permanently flooded with bacteria and bacterial products such as lipopolysaccharide and proinflammatory cytokines that could also affect distant sites and organs. 8 Bacteria that are closely associated with periodontal disease are Aggregatibacter actinomycetemcomitans and red complex bacteria: Porphyromonas gingivalis, Tannerella forsythia, and Treponema denticola. 9 Other species may also contribute to periodontal destruction, in particular bacterial species from the orange complex (which includes Prevotella intermedia).
The main goal of periodontal therapy is to eliminate bacterial deposits by mechanically removing the supra- and subgingival biofilms. 9 For this purpose, ultrasonic and/or hand instrumentation is used. Mechanical debridement leads to a reduction in the levels and proportion of some periodontal pathogens, but does not seem to modify the composition of the subgingival biofilm sufficiently. 10 Therefore, other forms of adjunctive therapies have to be used in conjunction with mechanical debridement to potentiate the effects of this treatment. Administration of local or systemic antibiotics has been proposed in periodontal treatment. 11 However, due to the structure of the biofilm, the penetration of an antibiotic through it is problematic. It is also difficult to maintain the therapeutic concentration of the antibiotic in the periodontal pocket, and in addition, there is an increased concern regarding the development of antibiotic resistance. Further, side effects related to the use of antibiotic should not be overlooked.
In the last decade, antimicrobial photodynamic therapy (PDT) has demonstrated additional clinical benefits. The efficiency of the use of a diode laser is mainly due to the fact that it activates dye molecules of the photosensitizer attached to the bacterial wall, thus producing highly reactive singlet oxygen and subsequently killing periodontal pathogenic bacteria. Recent studies have shown improvement in clinical periodontal parameters, especially in the reduction of the proportion of bleeding on probing (BOP) sites 12 and sites positive for periodontal pathogenic bacteria. 13,14 Unlike with the use of antibiotic, no side effects are connected with the use of PDT.
In view of the lack of data reported in the literature, the aim of this article was to evaluate the effect of repeated PDT on periodontal parameters and microbiological composition of subgingival microbial flora in an FA patient with periodontitis. To the best of our knowledge, this is the first report on periodontal treatment of a patient with severe neutropenia and thrombocytopenia after utilizing antimicrobial PDT.
Materials and Methods
Patient medical condition and previous oral treatment
A Caucasian female, aged 12 years, was referred to the Department of Pediatric and Preventive Dentistry for the purpose of extracting her second primary molar with extensive periodontal inflammation. The referral came from the University Children's Hospital where she had been admitted due to severe neutropenia (total number of leukocytes was 3.1 × 109/L and absolute neutrophil count 372/mm3) and thrombocytopenia (number of thrombocytes 62 × 109/L). She was of short stature, otherwise healthy looking, and properly developed, with no significant signs of hemorrhage diathesis. A couple of months after her first visit, she was diagnosed with having FA; in the patient, the biallelic mutations in the FANCA gene were confirmed.
Intraorally, extensive inflammation of the gums was noted. In the lower dental arch, a lack of space for the incisor and canine teeth was reflected in extensive periodontal tissue inflammation. She had permanent dentition with the preserved and pathologically mobile second lower primary molar on the right side (a tooth 85). The orthopantomogram revealed the absence of tooth germs of teeth 35, 45, and 37. Tooth 85 was extracted under antibiotic prophylaxis with amoxicillin.
The patient was instructed on maintaining quality oral hygiene and diet and invited to further visits every 2–3 months (5–6 visits/year). During each visit, supra- and subgingival dental biofilms were removed professionally, and chlorhexidine and fluoride varnishes (Cervitec and Fluorprotector, Ivoclar Vivadent, Liechtenstein) were applied to the surface of her teeth.
During individual visits, her periodontal status was reevaluated; the periodontal disease gradually progressed, despite the fact that she followed the instructions thoroughly. Therefore, an additional 10-month periodontal treatment protocol was proposed. The protocol was explained in advance to the patient and her parents, who agreed with the proposed treatment in writing. The treatment protocol was also approved by the National Medical Ethics Committee (No. 144/02/11).
Periodontal examination and treatment protocol
The 10-month protocol foresaw the same periodontal examination and therapeutic procedure during each visit; initially at the baseline, then additionally every 2 months. Before each visit, the patient received antibiotic prophylaxis and antifibrinolytic to prevent heavy bleeding during and after the periodontal treatment. As a drug for antibiotic prophylaxis, she received amoxicillin (1500 mg 1 h before and 1000 mg 6 h after the periodontal therapy), and for antifibrinolytic prophylactic therapy, tranexamic acid (Cyklokapron; MEDA Manufacturing GMBH), with a first dose of 750 mg and all subsequent doses of 500 mg every 8 h for 3 days before the periodontal treatment. In addition, she received prophylaxis with trimethoprim–sulfamethoxazole (three times weekly) and fluconazole (daily) due to the persistent severe neutropenia; at the age of 16 years and 1 month, the total number of leukocytes dropped to 2.2 × 109/L, the absolute neutrophil count to 176/mm3, and thrombocytes to 34 × 109/L.
During every periodontal examination, the following periodontal parameters were evaluated: dental biofilm (plaque index) PI, gingival index (GI), probing pocket depth (PPD), BOP, and clinical attachment level (CAL). Each periodontal parameter was assessed at six sites on each tooth of the patient. All measurements were performed by a single experienced dentist (U.M.). Thereafter, one subgingival biofilm sample was collected from each of five periodontal pockets (at teeth 16, 21, 26, 41, and 46). Plaque samples were collected with sterile paper points after the supragingival plaque at the sampling site had been removed.
A full-mouth professional plaque elimination began with dental cleaning, using a rotating brush, and was followed by the patient's 2-min mouth rinsing with a 0.2% chlorhexidine solution. Then, the oral cavity disinfection procedure was continued with an ultrasonic device (NSK Varios 970; NSK Europe GmbH) and completed with PDT. The photosensitizer phenothiazine chloride (HELBO-Blue Photosensitizer) was applied from the bottom of the periodontal pocket toward the crown on all affected teeth. After 3 min of action, the photosensitizer was rinsed with sterile distilled water. Each pocket was then exposed to a diode laser light (Helbo TeraLite; Bredent Medical; 660 nm, 60 mW/cm2) for a period of 1 min per tooth. At the baseline, the initial PDT was followed by two further episodes of PDT on the third and the seventh day after ultrasonic debridement. The described procedure of full mouth debridement was completed by a single episode of PDT every couple of months.
Microbiological assessment
The presence of the following periodontal pathogens was qualitatively determined in subgingival biofilm samples: Aggregatibacter actinomycetemcomitans (Aa), Porphyromonas gingivalis (Pg), Prevotella intermedia (Pi), Tannerella forsythia (Tf), and Treponema denticola (Td). Each sample was subjected to a polymerase chain reaction, followed by hybridization against species-specific DNA probes using a commercially available microDent® test (Hain Lifescience, Nehren, Germany) according to the manufacturer's instructions, as described earlier. 15
During each examination, a cheek swab of oral mucosa was taken to evaluate the presence of fungi Candida albicans. The cotton swab was transported with Amies Transport Medium (Meus, Piove di Sacco, Italy). Growing media used for fungal culturing were Sabouraud Dextrose Agar (BioMérieux, Marcy l'Etoile, France) and CHROMagar CANDIDA (Mast Diagnostica, Bootle, UK). The samples were incubated aerobically for 3 days 16 in Sabouraud agar at 37°C and in Chrom agar at 30°C. After 10 days, the results were assessed. The result was negative (−) if there were no colonies after 10 days. The scores 1+, 2+, and 3+ indicate up to two colonies and 3–10 more than 10 colonies, respectively.
Results
Periodontal clinical outcomes
During the survey period, mean values of PI were low and visible only after using a periodontal probe. GI was reduced from severe to moderate inflammation of gingiva (Table 1). During the 10-month period, a significant PPD reduction was observed; nevertheless, CAL increased slightly. BOP dropped from 100% at the baseline to 60% after 10 months.
BOP, bleeding on probing; CAL, clinical attachment level; GI, gingival index; PI, plaque index; PPD, periodontal probing depth.
In Fig. 1, the proportion of shallow (<4 mm), moderate (4–6 mm), and deep (>6 mm) pockets at the baseline at 2, 4, 6, 8, and 10 months after the treatment is presented. Two months after introducing the PDT, none of the periodontal pockets would be classified as deep pockets. Moderate pockets declined to zero after 8 months.
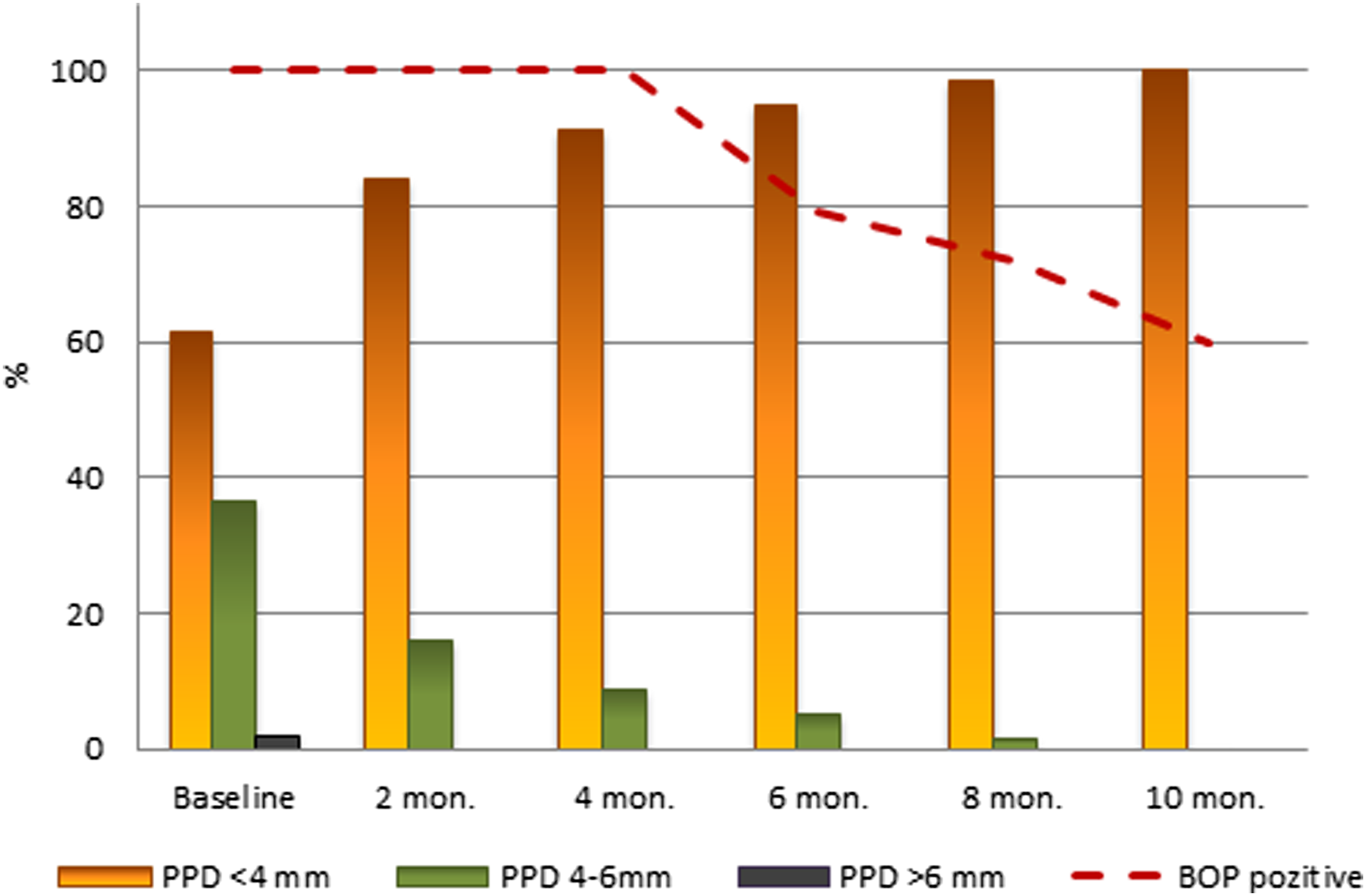
Proportion of examined sites with estimated shallow (<4 mm), medium (4–6 mm), and deep (>6 mm) pockets, and proportions of examination sites that are BOP positive. After 10 months of treatment, all periodontal pockets were in a group of shallow pockets and BOP decreased to 60%. BOP, bleeding on probing.
Microbiological analysis
Figure 2 shows the presence of periodontal pathogens at each time interval when PDT was repeated. At the baseline in each of the collected five biofilm samples, positive results were found for the presence of all pathogens investigated, except for P. intermedia. The results of the presence of P. intermedia were negative throughout the survey. A. actinomycetemcomitans and P. gingivalis were graded 2 in all five samples from the baseline to 4 months. After that time interval, A. actinomycetemcomitans was negative and the P. gingivalis presence was halved. After 6 months, a complete reduction of all pathogens was observed.
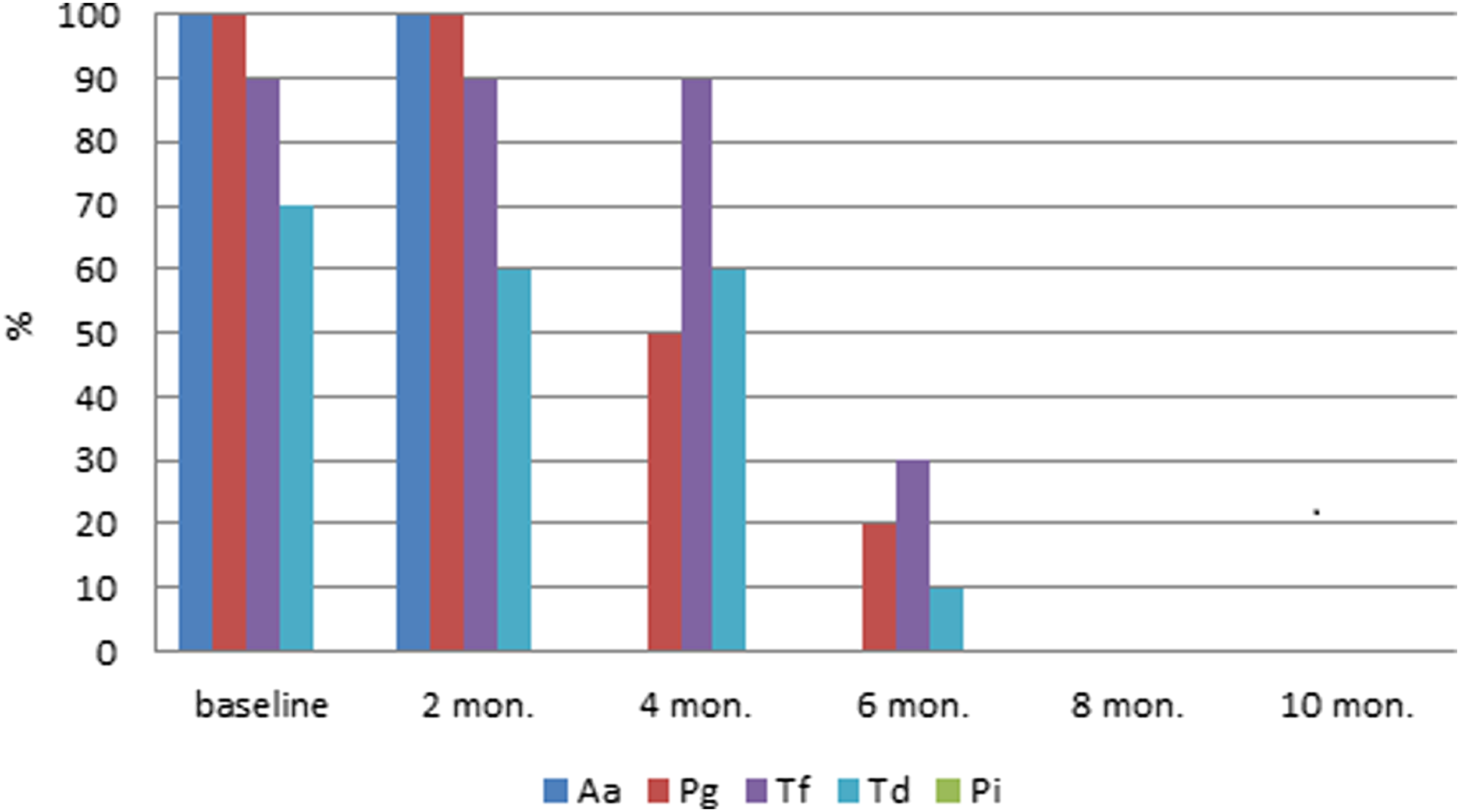
Semiquantitative periodontal pathogen evaluations during the 10-month period. Each column represents cumulative value for the selected bacterial species of all five samples taken at each examination (grade 2 represented as 20%, grade 1 as 10%, and grade 0 as 0%). A decrease of pathogen proportion for all bacteria was observed after 4 months, with complete reduction after 6 months. The presence of Prevotella intermedia (Pi) was negative throughout the treatment protocol.
The profound influence of the described treatment protocol utilizing PDT has also been shown on C. albicans. At the beginning of the study, the growth on microbiological culture media of C. albicans was evaluated with the highest score possible (3+). Two months later, the result of growth of C. albicans was negative. Further microbiological testing, performed 4, 6, 8, and 10 months after the baseline examination, confirmed further negative results of C. albicans growth.
Discussion
Periodontal disease is one of common oral manifestations in patients with FA. The development of infection with C. albicans is also a frequent finding in FA patients and even more likely as the patient received antibiotic prophylaxis before each of the visits. For that reason, it was decided to monitor also the presence of C. albicans. Although periodontal disease presents an inflammation focus, which seriously jeopardizes the patient's health and can subsequently result in loss of affected teeth, for FA patients, no selected treatment protocol is recommended in the literature. Its treatment remains unclear in terms of both the selected form of periodontal therapy and number of repetitions and/or the time intervals between treatment sessions. Undoubtedly, for these patients, the most appropriate form of treatment is an effective, but minimally invasive, method. The PDT of periodontal pockets, followed by ultrasonic scaling, resulted in microbial reduction and improved periodontal treatment outcomes. In addition to favorable bactericidal effects, the diode laser application aided in faster periodontal healing due to its biostimulation effects. 17
The PDT utilized in this study proved to be an effective and safe adjunct treatment of periodontitis with no unwanted side effects. The effectiveness was observed both in clinical terms and through microbiological results. During this period, the inflammation of gingiva decreased from severe to moderate form. The mean values of PPD and BOP were 3.4 mm and 100% at the baseline, while 10 months later, they dropped to 2.4 mm and 60%, respectively. All periodontal pathogenic bacteria and C. albicans were reduced to undetectable values after 8 months from the beginning of implementation of the treatment protocol.
The development of periodontal disease is particularly associated with A. actinomycetemcomitans (with the most virulent serotype b) and so-called red complex bacteria (which include P. gingivalis, T. forsythia, and T. denticola) and, to some extent, with orange complex species. A. actinomycetemcomitans is found in significantly higher proportions in subjects with aggressive periodontitis in comparison with chronic periodontitis or periodontal healthy subjects, while the red complex species are present in higher proportions in patients with aggressive as well as in patients with chronic periodontitis. 10 The red complex bacteria are detected in higher proportion in diseased sites of patients with periodontitis and are strongly associated with PPD and BOP. 10 In this study, the results of all subgingival biofilm samples obtained at the baseline were scored positive (grade 1 or 2) on A. actinomycetemcomitans and all three red complex species. After PDT, all studied periodontal pathogens dropped significantly; in all plaque samples, the results were negative for A. actinomycetemcomitans 4 months after the baseline and for P. gingivalis, T. forsythia, and T. denticola 8 months after the baseline measurements. The results for P. intermedia were negative throughout the survey.
Unlike in systemically healthy patients, periodontal tissue inflammation in patients with immune system deficiency does not develop primarily due to dental biofilm. It is suggested that the defects in neutrophil chemotaxis may be the key etiological factors in the pathogenesis of aggressive periodontitis. 18 Nevertheless, in patients with immune system deficiency, supra- and subgingival biofilms also have a significant impact on the progression of periodontal inflammation. By careful control of dental biofilm, progression of the periodontal inflammatory process can be stopped or at least slowed down. The patients' appropriate education and motivation to practice his/her excellent daily oral hygiene are of great importance; an ultrasoft toothbrush and rinsing with an antiseptic (e.g., chlorhexidine, iodine, fluoride) are recommended for home use. 19 Periodontal disease could be controlled if adequate hygiene is maintained and regular visits to the dentist at intervals of 2–3 months are paid. 20 Following this recommendation, a thorough full oral cavity disinfection was given to the patient at intervals of 2–3 months for 4 years. During the last 10-month period, when the patient received additional PDT, an important improvement in her periodontal condition was observed, especially in terms of reduction of gingival inflammation, PPD, and BOP.
In patients with FA, periodontal diseases are rather common. In a group of 33 patients with FA, gingival bleeding (48%), gingivitis, or periodontitis (36%) was reported. 5 In another study, investigating the oral health status of 15 children with FA, aggressive periodontitis was described in 2 of 15 children. 21 Nowzari et al. reported about an 11-year-old FA patient with severe gingival inflammation, some gingival overgrowth, and various degrees of CAL on most of erupted teeth. 4 Saleh and Stephen found generalized gingival recession, deep periodontal pockets, and visible furcation areas on most posterior teeth, as well as pathological mobility of the teeth and loss of alveolar bone in a 16-year-old male with FA. 6 Opinya et al. reported on periodontal pockets more than 10 mm deep and grade three furcation on remaining molars and maxillary premolars in a 24-year-old FA patient; he had only 19 teeth remaining in the mouth, most of them with grade three mobility. 22
The FA patients are at high risk of developing serious health complications, with prevailing expected progressive bone marrow failure and with increased predisposition to various cancers, hematological and solid tumors (including leukemia, carcinomas, and liver tumors). Periodontal disease could also represent an additional risk for systemic health. The described PDT in the FA patient was performed before the patient received treatment with BMT. Just before BMT, a patient's immune system is always additionally severely weakened. Prior reduction or, if possible, elimination of periodontal inflammation would especially reduce the risk of systemic complications during this period. Treatment of periodontitis with PDT proved to be very effective and without any unwanted side effects, resulting in abolishment of periopathogenic bacteria and improvement of periodontal clinical signs, and could potentially be considered as an important pretreatment procedure before BMT.
Conclusions
During the 10-month period of the periodontal treatment utilizing PDT, a significant improvement of oral health was observed in the patient. Clinically, especially favorable reductions of values of PPD and of numbers of sites positive on BOP were observed. From a microbiological point of view, it seems particularly important that with a sufficient number of repetitions of PDT treatments, an optimal effect is feasible: after 6 months, complete reduction of all observed bacterial species and C. albicans was found. Further investigations are necessary to determine: - whether a 2-month interval is really optimal for the described periodontal treatment with PDT, - what is the most appropriate number of PDT treatment repetitions, and - after what period of time the status of the patient's oral health will begin to deteriorate again following the described successful outcome, if at all.
Footnotes
Author Disclosure Statement
No competing financial interests exist.