
Abstract
Introduction
E
There is increasing evidence that irrigant agitation within well-shaped canals plays a critical role in cleaning and disinfecting the root canal system, including the dentinal tubules. Traditional syringe delivers the irrigant only 1 mm deeper than the needle tip and a vapor lock at the apical third limits irrigant delivery at the apical area. 7 The efficacy of irrigation has been enhanced beyond the conventional syringe by the development of different agitation systems. 7,8 The V-Clean™ endodontic agitator (SS White, Lakewood, NJ) is a newly launched endodontic microbrush that is constructed of medical-grade polymer. This highly flexible instrument is used manually in a rotary motion to enhance canal debridement. The EndoMaster (ENC System, Seongnam, Republic of Korea), which uses a hand file to create sonic vibrations, is supposed to enhance root canal disinfection. In addition, passive ultrasonic irrigation was shown to provide better root canal debridement at the apical 3 mm level compared with a conventional syringe due to generated acoustic microstream. 9 Recently, intracanal agitation by neodymium-doped:yttrium aluminum garnet (Nd:YAG) or Er:YAG laser energy has been reported to be effective at smear layer removal or sealer penetration into dentinal tubules. 10 –12 When lasers are activated in water, elliptical vapor bubbles form and expand, which causes high pressure, and they exhibit cleaning effects. However, the Er:YAG laser requires a water spray to avoid rapid overheating, which makes it challenging to maintain irrigant concentration. The Nd:yttrium aluminum perovskite (YAP) laser with 1.34 μm wavelength that was introduced by Blum and Abadie 13 is believed to be well absorbed in water, 14 although little is known about its irrigant agitation effects.
The effectiveness of different irrigation techniques and devices has been mostly evaluated by debris scoring using the sectioning method, scanning electron microscopy, or histology. 15 –18 However, the antibacterial effect achieved by endodontic treatment is more likely affected by deep infiltration of irrigant to scavenge bacteria residing inside dentinal tubules and by sealer infiltration to entomb bacteria within the tubules. 19 Therefore, the aim of this study was to investigate the effect of different agitation methods on irrigant and sealer penetration into human dentinal tubules. The intratubular penetration of both irrigant and sealer was assessed within the same sample to provide more objective and concurrent comparisons. The null hypothesis was that there are no significant differences in the penetration of irrigant and sealer into dentinal tubules with different agitation techniques.
Materials and Methods
Tooth selection and preparation
Approval was obtained from the Institutional Review Board of Seoul National University Dental Hospital, Seoul, Korea (CRI15011). Human single-rooted maxillary premolars were selected (n = 60), which were free of caries and prior root canal treatment. They were cleaned of extraneous tissue with an ultrasonic scaler and stored in 0.5% sodium azide solution. Each tooth was examined radiographically to confirm that the canals were not calcified and that their curvatures were less than 20° according to the Schneider technique. 20 The teeth were then decoronated with a diamond disc to produce a standardized root length of 12 mm to facilitate instrumentation. After access cavity preparation, a 21-mm #10 K–file (Dentsply Maillefer, Zurich, Switzerland) was inserted into each canal until it was just visible at the apical foramen and working lengths established at 1 mm short of these lengths. The canals were then instrumented in a crown-down technique with ProTaper Next® NiTi rotary files (Dentsply Maillefer) up to an X4 (apical size 40) at working length. Between successive files, the canals were irrigated with 1 mL of 5.25% sodium hypochlorite (NaOCl) and 17% ethylenediaminetetraacetic acid (EDTA), which were delivered through 30 G irrigation needles (Vista-Probe; Vista Dental, Racine, WI) with an up-and-down motion to within 1 mm short of working length.
Final irrigation with different agitation protocols
After the completion of chemomechanical preparation, the teeth were randomly divided into five groups according to the irrigant agitation protocols (12/group). As a final irrigant, 5 mL of 5.25% NaOCl mixed with 0.1 wt% fluorescent rhodamine B isothiocyanate (Sigma-Aldrich, St Louis, MO) was supplied into the root canals by conventional syringe to enhance visualization within dentinal tubules by confocal laser scanning microscopy (CLSM). Irrigant was deposited when the coronal reservoir was depleted. The agitation groups were as follows:
Group 1: Conventional syringe irrigation (control); Rhodamine B-labeled 5.25% NaOCl was continuously delivered for 30 sec through a 30 G irrigation needle (Vista-Probe) at 1 mm short of working length, with slight up-and-down motion.
Group 2: Sonic agitation; Rhodamine B-labeled 5.25% NaOCl was sonically activated for 30 sec with a #15 K-file mounted in the EndoMaster (ENC System) at H mode setting.
Group 3: Ultrasonic agitation; Rhodamine B-labeled 5.25% NaOCl was ultrasonically activated for 30 sec with an ISO #15 stainless steel ultrasonic file (Sirona Dental System GmbH, Bensheim, Germany) at 1 mm short of working length. The ultrasonic device (PerioScan; Sirona Dental System GmbH) was set at PERIO 3 mode.
Group 4: V-Clean endodontic agitator; Rhodamine B-labeled 5.25% NaOCl was agitated with a V-Clean endodontic agitator (#25/.04 taper; SS White). The agitator was placed at working length and a slight up-and-down motion was exerted for 30 sec, according to the manufacturer's recommendations.
Group 5: Laser agitation; Rhodamine B-labeled 5.25% NaOCl was activated by a 1.34 μm Nd:YAP laser (Lokki dt, Vienne, France) at 280 mJ at a 10-Hz pulse repetition rate as recommended by the manufacturer (power density, 5.73 W/cm2; energy density, 892 J/cm2). The teeth were held upright by an operator and laser was irradiated with a 200-μm flexible endodontic fiber placed 3 mm away from the apex. It was activated four times for 5 sec with a 10-sec interval in an apical-to-coronal motion along the long axes of the canals.
Root canal obturation
All canals were dried with ProTaper Next paper points and obturated with ProTaper Next gutta-percha X4 (Dentsply Maillefer) and AH plus sealer (Dentsply DeTrey, Konstanz, Germany) by using the continuous wave of condensation technique. Before use, the sealer was mixed with fluorescein isothiocyanate (FITC; Sigma-Aldrich) at 0.1 wt% to display a green fluorescence under CLSM. The FITC-labeled sealer was thoroughly dispersed into the canal by using a lentulo spiral and by lightly coating a prefitted gutta-percha cone. The coronal gutta-percha was then removed with a heated plugger (SuperEndo-α2; B&L Biotech, Ansan, Republic of Korea), and the remaining apical third compacted with a stainless steel plugger for 10 sec. Then, the middle and coronal portions of the canal were backfilled with warm injectable gutta-percha (SuperEndo-β; B&L Biotech) and vertically compacted at the canal orifice. The roots were sealed with Caviton (GC Corporation, Tokyo, Japan) and then stored in an incubator at 37°C and 100% humidity for 24 h to allow complete setting of the sealer.
CLSM observation
Each root was embedded in an acrylic resin block. Transverse sections were made with a slow-speed, water-cooled diamond saw (Isomet Low Speed Saw; Buehler, Lake Bluff, IL) at 2 mm (apical), 5 mm (middle), and 8 mm (coronal) levels from the root apex. The apical and coronal surfaces of the sections were then standardized to 500 μm in thickness by polishing with 1200, 2400, and 4000 grit silicon carbide abrasive papers (Struers, Westlake, OH). These sections were mounted on glass slides and examined by a confocal laser scanning microscope (Zeiss LSM-Pascal; Carl Zeiss, Göttingen, Germany) with an He/Ne G laser (543 and 632 nm). Magnified images ( × 50 and × 70) were captured in the fluorescent mode and analyzed with Zeiss LSM Image Examiner software (Carl Zeiss).
The maximum depth of irrigant and sealer penetration into dentinal tubules ( × 70 images) and the percentage of penetration into dentinal tubules ( × 50 images) were calculated by using a method previously described. 21,22 In brief, each image was imported into the Zeiss LSM Image Examiner, and the circumference of the root canal wall outlined and measured. The areas along the canal circumference where rhodamine B-labeled NaOCl (red fluorescence) and FITC-labeled sealer (green fluorescence) had penetrated into the dentinal tubules were outlined and measured. The percentage of dentinal tubules penetrated (%) was calculated from the ratio of the arc of the canal wall where irrigant had penetrated to that of the entire canal wall circumference. The maximum irrigant penetration depth (μm) was measured as the distance from the tubule orifice at the canal wall to the deepest point of penetration along the dentinal tubule. These measurements were made by an investigator who was blinded to the agitation protocols and they were repeated three times to ensure consistency and reproducibility.
Statistical analyses
Kruskal–Wallis analyses were performed for overall comparisons of penetration, followed by Mann–Whitney tests for multiple comparisons (p = 0.05). The Friedman test was used to compare the differences at the apical, middle, and coronal levels, and the Bonferroni correction applied for pair-wise comparisons between levels (p = 0.017). The Spearman correlation coefficient (r) was calculated at each level to determine correlations between irrigant and sealer penetration according to the categorization of Dancey and Reidy. 23
Results
For irrigant, maximum penetration depth and penetration percentage are shown in Fig. 1a and b, respectively. At 2 mm from the apex, there were no significant differences in maximum irrigant penetration depth between groups (p > 0.05). At the 5 and 8 mm levels, there was significantly more penetration depth in the laser group than the syringe, ultrasonic, and V-clean groups (p < 0.05). At 8 mm, the laser group attained the highest penetration depth among all groups (p < 0.05). For all groups, penetration depths at the 2 mm level were significantly less than those at 5 and 8 mm, according to the Wilcoxon signed-rank test (p < 0.017).
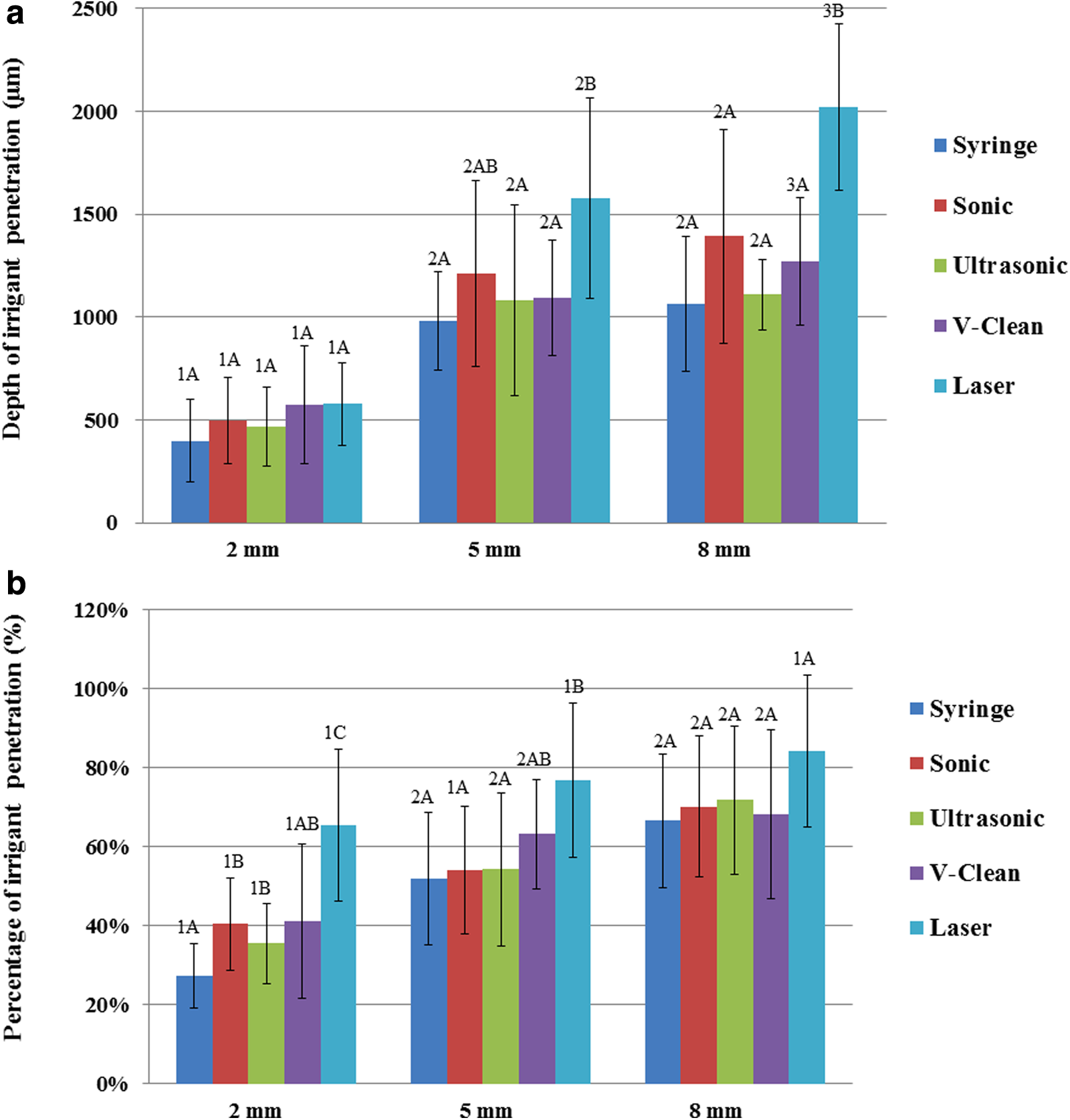
There were no significant differences in penetration percentage between the three levels in the laser group or between the 2 and 5 mm levels in the sonic group (p > 0.017). However, significantly lower penetration percentages were found at the 2 mm level among the other three groups (p < 0.017). At the 2 mm level, the sonic, ultrasonic, and laser groups showed significantly higher penetration percentage than the syringe group (p < 0.05). At the 5 mm level, the laser group obtained the highest penetration percentage, but the Mann–Whitney test indicated that there was no significant difference between the laser and V-Clean (p > 0.05). Additionally, there were no significant differences at the 8 mm level for all groups (p > 0.05).
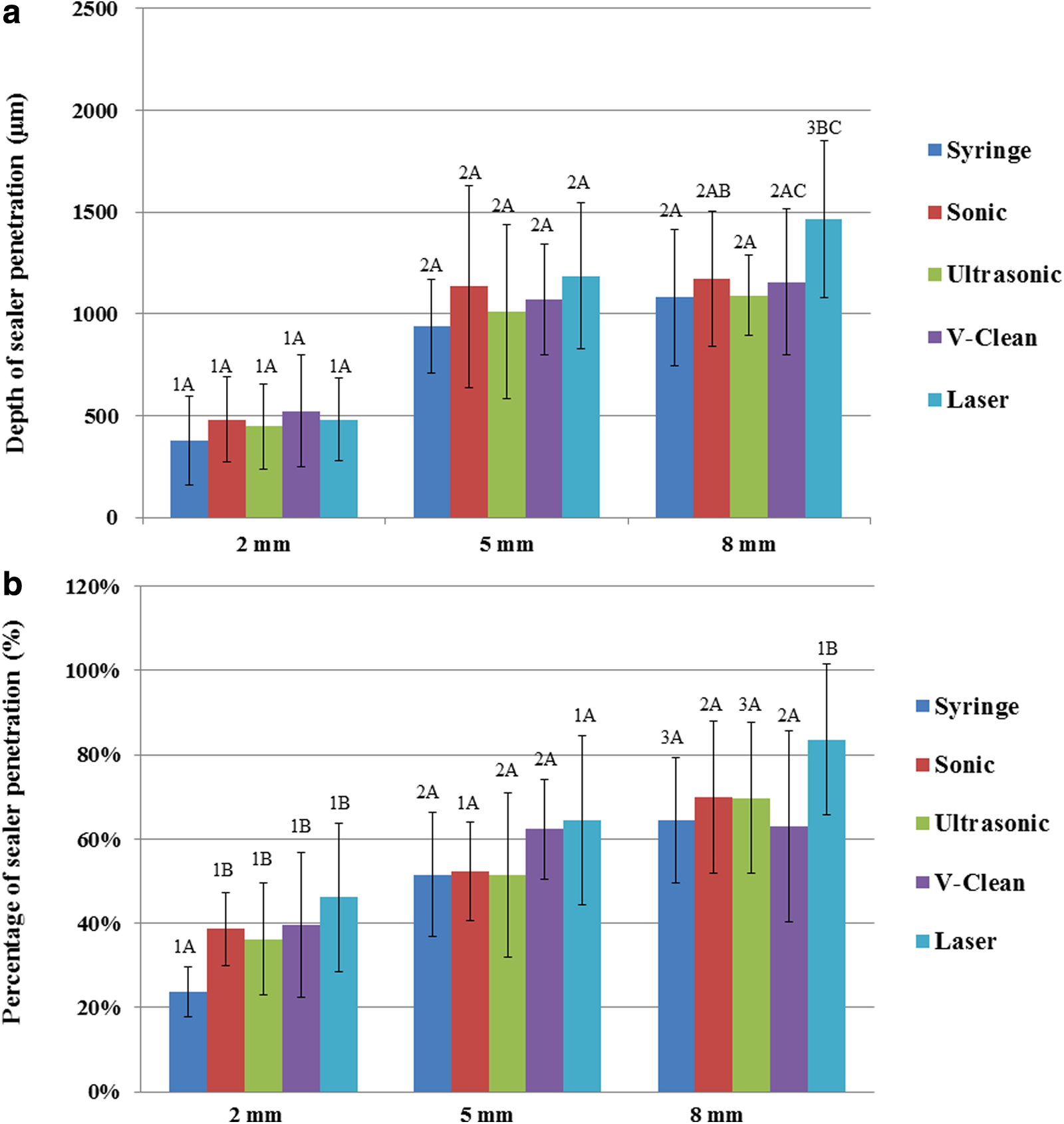
For sealer, maximum penetration depth and penetration percentage are shown in Fig. 2a and b, respectively. The laser group gained the highest penetration depth and percentage at all three levels, but significant differences were only found at 8 mm for penetration depth and 2 and 8 mm for penetration percentage (p < 0.05). For all groups, the penetration depth of sealer at the 2 mm level was the smallest, according to the Wilcoxon signed-rank test (p < 0.017). For all groups except sonic and laser, the penetration percentages at 2 mm were significantly different from those at the 5 and 8 mm levels.
A Spearman correlation analysis indicated that there were significant correlations between the maximum penetration depth and percentage of irrigant and sealer at each level (Table 1). Representative CLSM images of irrigant and sealer penetration into dentinal tubules for the five experimental groups at each level are presented in Fig. 3.
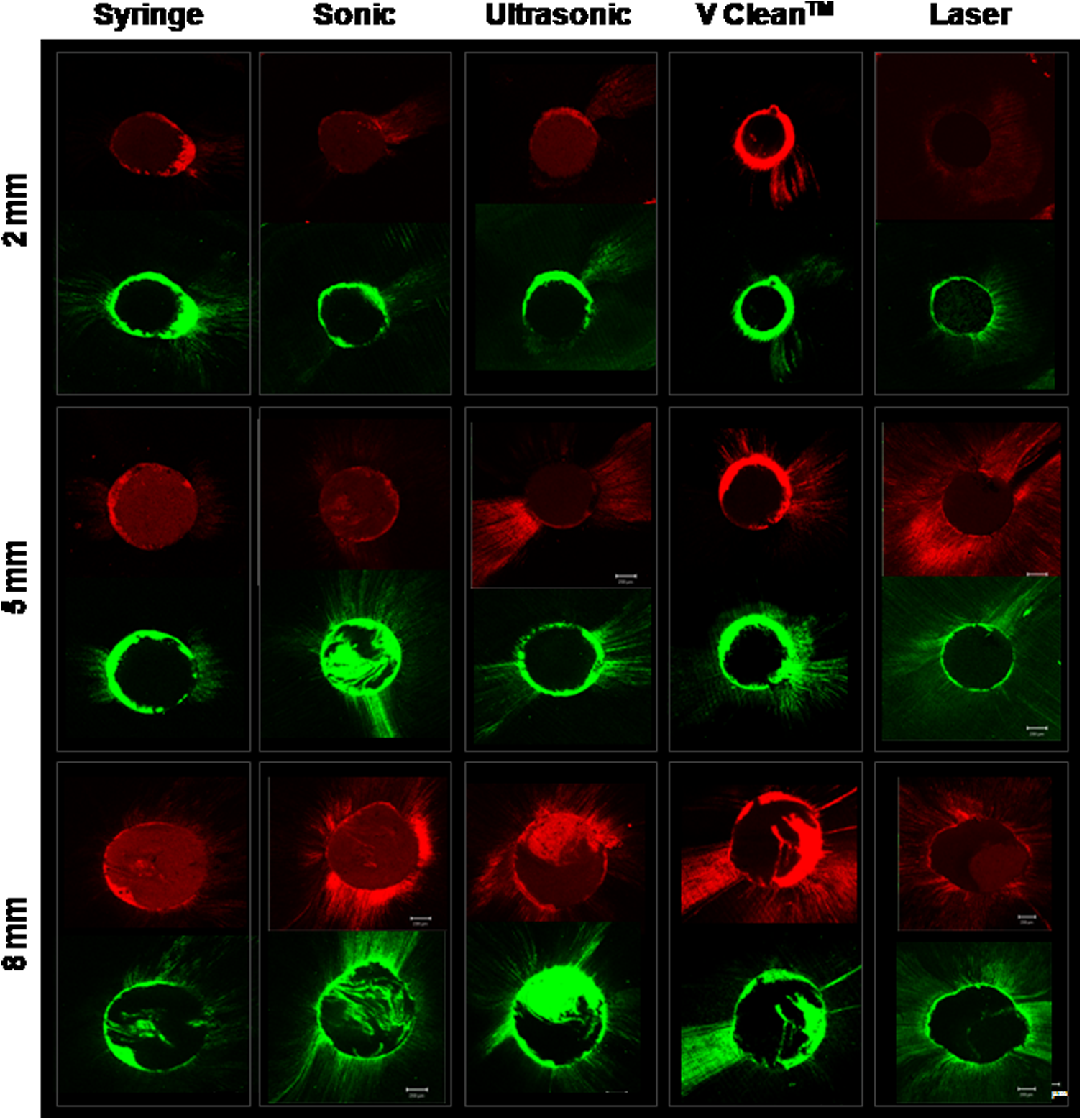
Representative CLSM images of both irrigant and sealer from five experimental groups (original magnification, × 50) at 2, 5, and 8 mm levels. The upper images (red) represent rhodamine B-labeled NaOCl, while the lower images (green) represent FITC-labeledroot canal sealer. CLSM, confocal laser scanning microscopy.
“r” represents the Spearman correlation coefficient; 0.70–0.99 indicates a strong correlation (Dancey and Reidy's categorization 2004).
Discussion
The purpose of this study was to investigate the efficacy of different agitating techniques in terms of dentinal tubule penetration of irrigant and sealer to achieve improved disinfection and sealing of root canal system. 24 The effect of each agitation technique was assessed as percentage, depth, and area of dentinal tubule penetration that were concurrently measured for both irrigant and sealer. As a result, laser agitation attained superior penetration depth and percentage of irrigant and sealer than other agitation techniques.
Several factors can influence the penetration of irrigant and sealer into dentinal tubules. Zou et al. showed that temperature, contact time, and concentration influenced the penetration of NaOCl into tubules. 25 Anatomical features may also limit irrigant penetration into dentinal tubules. The tubules are larger and more densely packed within the coronal and middle thirds of the roots, and tubular sclerosis begins within the apical area, 26 which may partly account for the lower penetration of irrigant and sealer at the apical 2 mm level, which was seen in this study. Further, since canal curvatures can also limit irrigant penetration, this study was restricted to relatively straight canals (curvatures <20°). Similar findings were reported for different sealer systems and obturation techniques. 2,27
Previous studies have compared various intracanal agitation techniques and the conventional syringe for irrigant penetration of dentinal tubules. 21,22 However, the present study used two distinct fluorescent dyes to distinguish and quantify irrigant and sealer penetration of dentinal tubules concurrently under CLSM by using the method introduced by Gharib et al. 28 Based on this methodology, the Nd-YAP laser clearly attained the highest values for irrigant and sealer penetration of dentinal tubules when compared with other agitation techniques. Similarly, Kundabala et al. showed that an 810 nm diode laser significantly improved irrigant penetration depth when compared with the conventional syringe. 29 A previous study also reported that the Nd:YAG laser with 1320 nm wavelength was better than either NaOCl or EDTA alone for sealer penetration. 10 Other studies showed that the Er:YAG laser was effective at dentin debridement and smear layer removal. 11,12 However, the Er:YAG laser requires a water spray to avoid rapid overheating, which makes it challenging to maintain irrigant concentration. In this study, we used 280 mJ at 10-Hz repetition. Other researchers who studied the same equipment at 260 mJ and 5 Hz also confirmed the effect of Nd:YAP laser during canal irrigation. 13,14 Further, the laser was the only technique for which the percentage of dentinal tubules penetrated was not significantly different at the three levels. This could be attributed to fluid dynamics and imploding vapor bubbles generated at their fiber tips and shock wave effects of the laser. 29 However, at the 5 and 8 mm levels in the laser group, the penetration depth of sealer did not reach that of the irrigant. In fact, the penetration depth of sealer was similar in all groups at the 5 and 8 mm levels, which suggests it was limited by the rheologic properties of sealer and the obturation technique that was used in this study. 30
Sonic and ultrasonic devices have been proposed for maximizing irrigant hydrodynamics and distribution within the root canal system, and a prior study found that they improved irrigation of lateral canals. 31 However, in the present study, sonic agitation appeared more effective in promoting irrigant and sealer penetration of dentinal tubules than the ultrasonic technique. This underperformance of the ultrasonic device may have been due to the shorter time for agitation and inadvertent contact between the ultrasonic file and canal walls, which may have dampened its effectiveness. 32,33
The more recently introduced V-Clean endodontic agitator is uniquely designed to provide a dual-action scrubbing/scraping process that removes the smear layer, dislodges and removes debris from the canal, and concurrently agitates irrigating solutions. The V-Clean has a similar design to the CanalBrush (Coltene/Whaledent GmbH+Co. KG, Germany) that is a rotary engine-driven instrument, and Kamel and Kataia showed that a CanalBrush with chelating agent increased debridement and smear layer removal. 34 On the contrary, our results revealed that the V-Clean endodontic agitator did not show any significant improvement over the conventional syringe for irrigant penetration of dentinal tubules. This is in accordance with the study of Garip et al. who found that the CanalBrush did not show any significant improvement in smear layer removal from the canal walls when compared with conventional irrigation. 35 It is speculated that manual activation of V-Clean generates limited vortex of irrigant compared with other machine-assisted devices, and complex anatomical variations of the root canal system impede its contact with the canal wall. 36 Further, the manual scrubbing or scratching motion could cram debris into dentinal tubules, which may also explain the underperformance of V-Clean in this study.
The influence of the smear layer on irrigant and sealer penetration into dentinal tubules is an ongoing debate that is still unraveling. Therefore, since the smear layer was not intended to be a major focus of our research, it was intentionally left unperturbed in our experimental design. Our rationale was based on the study by Paqué et al., 26 which showed that irrigant penetration was largely dependent on the presence of tubular sclerosis in the dentine, rather than the absence of a smear layer. Therefore, we examined the relationship between irrigant and sealer penetration patterns into dentinal tubules when using different intracanal agitation techniques. Since NaOCl molecules are smaller than AH 26 Plus sealer particles and have better flowability, greater irrigant penetration of fine structures was anticipated. However, the Spearman correlation coefficient revealed that there were significant correlations between the penetration pattern of irrigant and sealer at each of the three levels. This might be due to the improved canal cleanliness rendered by intracanal irrigant agitation. Additional studies that employ a smear layer model are needed to confirm this finding.
Conclusions
Intracanal agitation could enhance the penetration of root canal irrigant and sealer into dentinal tubules. The Nd:YAP laser was superior to other agitation techniques in dentinal tubule penetration of root canal irrigant and sealer at one or more sectioned levels from root apex. The penetration patterns of root canal irrigant and sealers correlated significantly with each other.
Footnotes
Author Disclosure Statement
No competing financial interests exist.