
Abstract
Introduction
U
Materials and Methods
Between May 2003 and April 2013, 25 patients (11 male, 14 female) with UFPs received treatment in our hospital. Patients' age ranged from 15 to 51 years (mean 38.2 years). Twelve patients presented with flank pain and six with gross hematuria. Seven patients had no symptoms and were found to have hydronephrosis in regular health checkup. Ureteral lesions were found on the right in 12 patients and on the left in 13 patients. There were no bilateral patients in our cohort. The foci were in the upper, middle, and lower part in 9, 6, and 10 cases, respectively. All patients underwent intravenous urography (IVU) and type-B ultrasonic check, five patients received CT scan. A urine cytology examination was performed on eight patients. Four patients received cystoscopy because an ultrasonic check suggested tumor in the bladder.
All 25 patients were assigned to the holmium laser group (12 patients) or thulium laser group (13 patients). Before 2007, four patients were assigned to the holmium laser group because we did not own thulium laser. After that, 21 patients were randomly assigned balancing single or multifocal UFPs according to imaging examination. Patients in both groups underwent ureteroscopy operation. We advanced the ureteroscope in the ureter and found the polyp root, and then, we resected the polyp root using holmium laser (VersaPulse PowerSuite™ 100 W; LUMENIS Surgical) at a power of 60 W or thulium laser (RevoLix™ thulium laser system; LISA Laser Products) at a power of 20–25 W. When finishing the operation, we placed a 6F double-J stent in the ureter.
Two or 3 months after operation, the double-J stent was pulled out in cystoscopy. At follow-up, all patients received IVU 1 month after double-J was pulled out, and ultrasonic checks every 3–6 months thereafter to monitor whether they develop more severe hydronephrosis. The follow-up period is 3 years.
Results
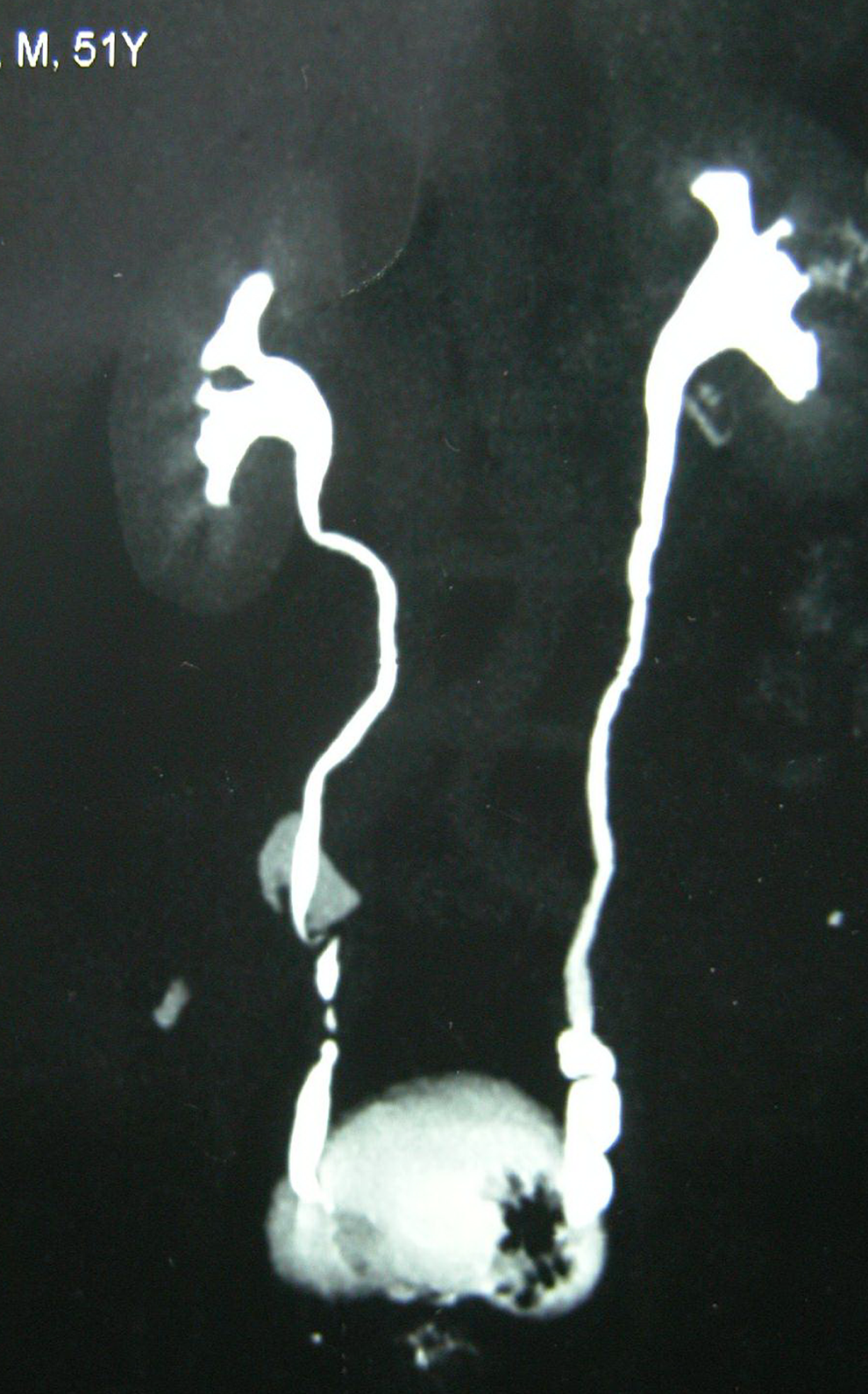
All patients received IVU and type-B ultrasonic check before operation. IVU demonstrated the presence of long and smooth filling defects in the ureter (Fig. 1) or bladder if polyps prolapsed into the bladder. Fourteen of them had mild-to-moderate hydronephrosis, nine of them had severe hydronephrosis, and others had no hydronephrosis. Sonogram showed a vermiform solid mass in the bladder in four patients, and other patients only presented with hydronephrosis or were normal. Five patients received CT scan, which showed a mass in the ureter or bladder (Fig. 2). Urine cytology results were negative in all eight patients receiving this examination. Cystoscopy found smooth pink polyps prolapsing into the bladder through left ureteral orifice in four patients.

Intravenous urography demonstrated the presence of long and smooth filling defects in ureter.
CT showed mass near ureteral orifice in bladder.
All patients received ureteroscopy operation. Ureteroscopic treatment was performed using a small caliber (F6/7.5) semirigid ureteroscope. We found smooth and slender polypoid lesion(s), usually projecting into the distal ureter (Fig. 3). We used holmium or thulium laser to resect polyps. The F6 double-J stent was placed into the ureter at the end of the operation. The average length of the polyps was 1.8 (0.8–4.0) cm. Multifocality was identified in 56.0% (14/25) of our cohort. The operation time of the holmium laser and thulium laser group, respectively, is 83.6 ± 29.0 and 69.2 ± 24.3 min. There was no statistical difference (p = 0.207, independent-sample test, using SPSS 13.0) (Table 1).

A ureteral fibroepithelial polyp projecting into distal ureter in ureteroscope vision.
p = 0.207.
p = 0.096.
p = 0.039.
UFP, ureteral fibroepithelial polyp.
In the holmium laser group, three patients met with minor ureteral perforation around the polyp root because of laser blow, and we just placed the double-J stent in the ureter to manage the complication. No major intraoperative complications developed in the thulium laser group. We used Fisher's exact test to compare ureteral perforation incidences in the two groups and found no statistical difference (p = 0.096, using SPSS 13.0). Six patients developed fever in 3 days and found relief when using a sensitive antibiotic; all patients had hematuria but no one needed blood transfusion. Pathological examinations of masses affirmed the diagnosis of UFP (Table 1).
Double-J stent was removed 2 or 3 months after the operation and IVU was performed 1 month later. Thereafter, all patients underwent type-B ultrasonic check follow-up to monitor if they developed more severe hydronephrosis every 3–6 months. To date, all patients met the 3-year follow-up period; 4 (33.3%) patients in the holmium laser group developed ureterostenosis and it usually happened in the 6th month after the double-J stent was pulled out. No severe long-term complication happened in the thulium laser group. UFP recurrence was excluded in ureterostenosis patients, so none of the patients had a relapse. We treated ureterostenosis by open surgeries. We used Fisher's exact test to compare the ureterostenosis incidences of two groups and found a statistical difference (p = 0.039, using SPSS 13.0).
Discussion
UFPs are rare and thought to be either congenital slow-growing lesions or lesions that develop as a result of chronic urothelial irritants, such as infection, inflammation, or obstruction. 2 A study from the Mayo Clinic identified only 27 patients with UFPs between 1945 and 2008. Mean age at diagnosis was 40 years. Polyps were more common in the left (68%) than in the right ureter. There were no bilateral patients; 59% were proximal, 18% were in the middle area, and 18% were distal. Six patients (27%) had multiple polyps. 3 Most polyps are smaller than 5 cm; however, larger polyps have been reported. The most common presenting signs and symptoms are hematuria and/or flank or abdominal pain.
Most of our data are in line with aforementioned data, but we have a higher ratio of multiple polyp cases. We also notice that if the polyp is single, it usually grows bigger and longer (often longer than 3 cm), and if the polyps are multiple, they usually are shorter and thinner, usually growing in clusters but sometimes dispersedly. Also, urinary calculus are absent beside polyps, indicating that the polyps are not stimulated by calculus. We usually see polyps beside calculus when treating urethral calculus, and these kind of polyps are multiple, thinner, and smaller than UFPs, grow into a circle, never grow dispersedly, and can be absorbed after stone removal.
Radiographic diagnosis is crucial to surgical management. Polyps may be imaged by CT, ultrasound, magnetic resonance urography, IVU, and retrograde pyelogram. Ultrasound may show evidence of hydronephrosis or hydroureter, although dilation is typically mild, or a mildly echogenic structure with a polypoid projection without acoustic shadow. However, diagnosis is usually established by IVU. Continuous filling defect(s) with smooth edges is a trait in IVU and retrograde pyelography (Fig. 1). This differs from the “moth-eaten” appearance of filling defects in cases of upper tract urothelial carcinoma. 4 Nevertheless, a definitive diagnosis relies on biopsy specimens.
Ureteroscopy combined with holmium lasers has been reported treating UFPs. Thulium laser is a new surgical laser, whose wavelength is 2013 nm. This wavelength is strongly absorbed by water, with a low tissue penetration, <0.3 mm. 5 With these advantages, we think thulium laser could also be useful in delicate ureter operations. From the results we know that both holmium and thulium laser could resect UFPs smoothly, and that UFPs did not recur. We did not find ureterostenosis happening in the thulium laser group. However, in the holmium laser group, the incidence of ureterostenosis after operation was 33.3%, and the difference was statistically significant. Although there is no statistical difference in ureteral perforation incidences, we still think that thulium laser is better than holmium laser based on the following reasons. First, thulium laser has a higher absorption of the laser radiation resulting in more efficient and rapid tissue cutting, and has more excellent hemostasis and accurate incision effects. 6 Second, when holmium laser is working, the fiber trembles slightly, and thus, we think holmium laser is less accurate and that is why three patients in the holmium laser group had ureteral perforation. Third, thulium laser is capable of reducing thermal damage compared with the holmium laser. Minimizing thermal damage may be important in reducing scar formation and stricture recurrence after laser incision of the ureter and urethra. 7 Fourth, thulium laser's operation time is shorter than that of holmium laser, although there was no statistical difference. We think it is partly because the holmium laser group has more multifocal UFPs than the thulium laser group. Fifth, we find that the wound surface of holmium laser is rougher than that of thulium laser, which partly causes ureterostenosis. Finally, the first 4 patients assigned to the holmium laser group may be related to higher ureterostenosis incidence of holmium laser. However, we still preferred thulium laser to holmium laser, especially when treating multifocal UFPs.
Because of the benign nature of UFPs, resection should be neither too deep nor wide. The resection should be limited to the mucosa or submucosa. Furthermore, the main disadvantages of ureteroscopy resection are as follows. The difficulty often results from the inability to access the base of the stalk because the pedunculated body usually hangs inferiorly from the stalk for several centimeters and can occupy the entire lumen of the ureter. Visualization can also be poor and working space limited, making it difficult to differentiate the ureteral wall from the polyp itself. This can lead to incomplete polyp resection or ureteral perforation. 8 In practice, we have noticed aforementioned disadvantages and have attainment some experience as follows. (1) We use the F6/7.5 ureteroscope to accomplish this operation. This size of ureteroscope has a smaller caliber than the F8/9.8 ureteroscope, but has enough working channel for 3F foreign body forceps and 365 nm laser optical fiber passing through together. With it, we can get a better visualization and working space, maybe a smaller renal pelvic pressure additionally. (2) If the UFP root is not seen clearly, we may use 3F foreign body forceps to catch and push (or pull) the UFP stalk first, so that we can distinguish the ureteral wall from the polyp itself easily. Then, we stick in the fiber to resect the polyp root with the tension from forceps pushing/pulling stalk. After resection of polyps, the lumen is still smooth and wide. (3) If the resected polyp is too big to be pulled out through the ureteral orifice, we catch the polyp with foreign body forceps and then mince the polyp into several tissue blocks with laser. After that, we can pull the polyp out. Also, care should be taken not to let the polyp go into the renal pelvis because the proximal ureter could be dilated and the ureterovesical junction is narrow. (4) If there are multiple polyps, we use the same method to resect them one by one.
In this study, the follow-up period is 3 years, and we will continue to follow up and get long-term results.
Conclusions
UFPs are rare benign tumors and its diagnosis is usually established by IVU. Ureteroscopy operations, combined with holmium or thulium laser resection, are both effective methods treating UFPs, but thulium laser is better in reducing the incidence of urethral stricture.
Footnotes
Author Disclosure Statement
No competing financial interests exist.