
Abstract
Introduction
P
As stated by Jacques, 17 the ability of light to penetrate a tissue and deposit energy through the absorption properties of the tissue is key to therapeutic applications. According to Beer–Lambert's law, if tissue is irradiated with a laser, the fluence rate (W/m2) of the beam inside the tissue decreases exponentially. 18 As described by Welch and Gardner, laser tissue interaction is viewed as the propagation of photons through a volume of randomly distributed absorption and scattering centers. 18 The behavior of scattering and absorption is wavelength dependent. 17 Therefore, the wavelength of the light governs its depth of penetration into a tissue, which is defined as the depth at which the intensity of radiation inside the material falls to (1/e) or ∼37% of its original value. Both the absorption and scattering coefficients of living tissues are higher at shorter wavelengths, therefore near-infrared light penetrates more deeply than red light. 18 Indeed, the least amount of absorption occurs in the 600–1000 nm band of wavelengths, 18 which corresponds to what is known as the therapeutic window.
A number of studies have examined penetration of light through tissues. In 2005, we examined transcutaneous light penetration to the level of the spinal cord in adult, anesthetized Sprague-Dawley rats. 19 An incoherent broadband white light was applied to the surface of the skin over the thoracic vertebrae. A smart, tissue-activated optical fiber probe 19 was inserted sequentially into the skin, subcutaneous connective tissue layer, deep connective tissue layer, the dorsal muscle mass, and the spinal cord within the vertebral column. At each of these layers, a transmission spectrum in the range of 500–1200 nm was collected. Analysis of the transmission spectra revealed that the range of transmission was highest through all tissue layers overlying the spinal cord and through blood between the 770 and 850 nm wavelengths with a peak at 810 nm. The 810 nm wavelength was minimally absorbed by blood and water. These data show that 810 nm wavelength light is within the optimal range for transcutaneous light transmission to tissues deep in the body. 19 Several studies have compared penetration of continuous wave (CW) 904–810 nm wavelength light and none demonstrated greater depth of penetration of the 904 nm wavelength. 19,20
In 2012, Joensen et al. investigated the relative penetration of CW 810 nm wavelength light and 904 nm wavelength superpulsed light through skin samples taken from the region overlying the Sprague-Dawley rat's gastrocnemius muscle over 150 sec. 21 With the CW 810 nm wavelength laser probe in skin contact, the amount of penetrating light energy was stable at 20% of the initial output power during the 150-sec irradiation. Irradiation with the superpulsed 904 nm wavelength laser had a linear increase in the penetrating light energy (percentage of mean output power) from 38% to 58% during the 150-sec irradiation period. Based on these results, the authors speculated that the superpulsed 904 nm wavelength light penetrates two to three times easier through the rat skin than the CW 810 nm wavelength light. The authors concluded that the superpulsed light may be causing photobleaching of some element such as collagen in the skin over the collection time. 21
It is important to note that although Beer–Lambert's law assumes a CW laser beam, it also holds for pulsed irradiation. 18 Therefore, pulsing has no effect on the depth of penetration of a given wavelength. Pulsing can affect the number of photons per unit time or therapeutic dose delivered to a tissue along the depth dictated by the wavelength, but does not change the depth of penetration. 22 In fact, we recently reported in a study of trans-scalp 808 nm wavelength light penetration gradients into human cadaver brains that no difference was observed in the normalized fluence rates measured with the laser operating sequentially in CW mode, pulsed at 10 Hz, 20% duty cycle, and pulsed at 100 Hz, 20% duty cycle. 23
Aim
Because of our experience with light transmission of various wavelengths in human cadavers and anesthetized rats and due to the discrepancies in the literature about the facts of pulsing on depth of penetration, we decided to investigate light transmission of CW 810 nm wavelength light and 904 nm wavelength superpulsed light using an anesthetized Sprague-Dawley rat model. Our goal was to determine if a previously reported increase of penetration of 904 nm wavelength superpulsed light 21 over time occurred in our model.
Materials and Methods
Devices
The output power was measured using a LabMaster Ultima power meter with LM-3 HTD sensor (Coherent, Inc., Santa Clara, CA). The fluence rate was measured by a near-infrared detector, which was designed and built by B&W Tek, Inc. (Newark, DE). For this detector, a small photosensor (2.0 × 2.5 mm) was sealed in a glass tube (Fig. 1a). The output voltage of the sensor was calibrated such that a reading of 1 mV represented 1 mW/cm2. This sensor was used to determine irradiance outside of the tissue and fluence rate within the tissue.
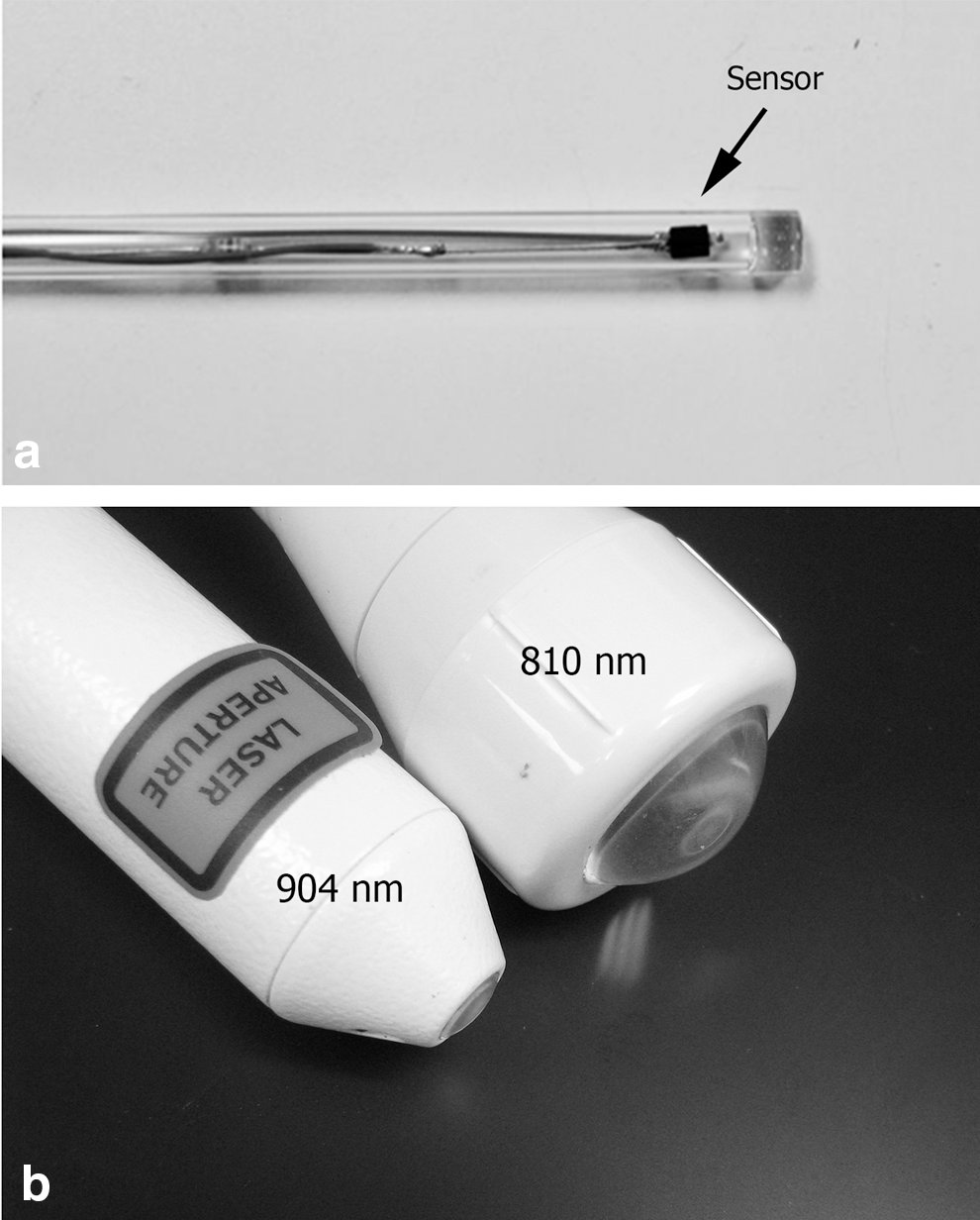
A near-infrared detector used to measure fluence rate
Two laser devices were used in this study: (1) 810 nm wavelength CW mode (Model BWF5-808-20; B&W Tek, Inc.), the output power of the 810 nm wavelength laser was set at 1 W; (2) 904 nm wavelength superpulsed mode (Model MID-laser; Irradia, Stockholm, Sweden) with a peak power of 20 W and mean output power of 60 mW, with a frequency of 6 kHz (manufacturer's specifications). The 904 nm wavelength superpulsed laser automatically shuts off after 5 min. Note that the 904 nm wavelength superpulsed laser used in this study is the same model laser used in the Joensen et al. investigation. 21 Both laser probes have a convex lens (Fig. 1b). To measure the output irradiance of the lasers, the lens of each probe was placed in contact with the glass tube that houses the photosensor. The distance between the lens and the photosensor was ∼2 mm. Since the sensor reads the irradiance, the probe was moved until the location of the highest reading within the beam was identified.
Animals
Three male Sprague-Dawley rats (Charles River Laboratories International, Inc., Wilmington, MA) were used in this study under an approved Uniformed Services University IACUC protocol. Rats were singly housed and kept on a 12-h light/12-h dark cycle. Food and water were provided ad libitum.
Surgery and light penetration measurements
The rats were anesthetized with 4% chloral hydrate. The hair was shaved from the left thigh region. To measure transmission through the gastrocnemius muscle and overlying skin, a longitudinal incision (∼2 cm) was made caudal to the posterior border of the muscle. With this approach, the detector could be placed in the fascial plane deep into the gastrocnemius muscle without disrupting the muscle or the overlying skin. After these measurements were complete, the detector was placed in the fascial plane below the dermis to measure light transmission through the skin. Once the detector was in place, the laser probe was positioned in contact with the surface of the skin. The laser was turned on and the probe moved until the location of the highest reading was identified. The probe was kept in that position for the duration of the measurements.
For the initial measurements, the lasers were turned on and after operating for 20 sec, the data were collected at 0, 10, and 30 sec, and then every 30 sec for a total of 4 min. The 0-sec collection time represents the first measurement taken within 5 sec of turning on the laser. For the 904 nm wavelength superpulsed laser, these 4-min data collection sessions were repeated three consecutive times by turning off the laser for 2 min and then repeating the measurements. It was noted that the 810 nm wavelength laser output power was stable after 20 sec of operation. For the measurements addressing the stability of the 904 nm wavelength superpulsed laser, the laser was turned on for 5 min. When the laser turned off automatically at 5 min, it was immediately turned on again and data were collected at 0, 10, and 30 sec, and then every 30 sec for a total of 5 min. The laser was turned on for a third time and fluence rate measurements were collected for another 5 min as described. For the measurements of light transmission through the skin, the lasers were turned on for 10 min to assure the stability of their output power before the fluence rate measurements were collected. The output power of the laser was considered stable when its fluctuation was within the 5% range. The laboratory lights were lowered during data collection. The rats were euthanized after the measurements were completed.
Determination of stability of laser output power
To measure the stability of the 810 nm wavelength laser and the 904 nm wavelength superpulsed laser, the output power was measured every minute through four 5-min sessions for a total of 20 min. The 904 nm wavelength superpulsed laser shuts off automatically at 5 min. Immediately after the auto shutoff, the laser was turned on again to continue measuring the output power. To keep the measurement conditions consistent, the 810 nm wavelength laser was shut off every 5 min and turned on again for the same periods of time during data collection.
Results
An increase in transmission of 904 nm wavelength superpulsed light does not occur after a minimum operation period of 10 min
In anesthetized rats, the detector was placed deep into the gastrocnemius muscle with all the tissue above the muscle intact. A series of fluence rate measurements were collected over 4 min for the 810 nm wavelength laser and 904 nm wavelength superpulsed laser. The fluence rate measurements for the 810 nm wavelength laser were stable over the 4 min (Table 1). However, the fluence rate measurements for the 904 nm wavelength superpulsed laser were stable for the first 3 min and then had an increase of 18% in the last minute of data collection (Table 1, 904 nm laser first 4 min). The laser was turned off for 2 min and then the measurements were repeated (Table 1, 904 nm laser second 4 min). The initial measurement during the second 4 min was 0.0313 mW/cm2 and was similar to the initial measurement of 0.0326 mW/cm2 in the first 4-min measurement series. However, the values of the measurements started to increase earlier at 90 sec of laser operation. The percentage of increase in the fluence rate for the second 4 min of measurements was 21%. The same process was repeated a third time (Table 1, 904 nm laser third 4 min). During this third series of measurements, the irradiances started to increase at 30 sec and the increase in irradiance over the 4 min was 21%.
The values of the 904 nm wavelength superpulsed laser increased earlier over three 4-min measurement sessions (indicated by bold values).
Since the increase in the fluence rate measurements started earlier and earlier when operation time went longer, it was concluded that the increases in the measurements were caused by instability of the laser mean output power due to an insufficient warm-up period. Therefore, another set of measurements was done to increase the operation time of the 904 nm wavelength superpulsed laser and measure the stability of the fluence rate measurements. The laser was turned on and run for 5 min, which is the longest operation time before the auto shutoff. The laser was immediately turned back on and data were collected. (Table 2, 904 nm laser second 5 min). When the laser turned off, it was turned on a third time and measurements were collected for another 5 min (Table 2, 904 nm laser third 5 min). Only an 8% increase in the fluence rate occurred during the second 5 min of measurements and, during the third 5 min of measurements, it was stable. These data demonstrated that fluence rate measurements were stable if the 904 nm wavelength superpulsed laser was turned on for a minimum of 10 min before the measurements were done. Therefore, the reported increase in penetration of 904 nm wavelength superpulsed light was an artifact of the laser reaching stability during the first 15 min of operation.
Note that the third 5-min measurements were stable.
Transmission of CW 810 nm wavelength light through skin is greater compared with 904 nm wavelength superpulsed light
Transmitted fluence rate of light through the skin was measured by placing the detector in the fascial plane below the dermis of the skin and laser probe in direct contact with the surface of the skin in the anesthetized rat. To ensure that the 904 nm wavelength superpulsed laser had reached a stable output power, the laser was turned on for two 5-min cycles before collecting the data. The 810 nm wavelength laser, which reached stability after a short on time, was turned on for 30 sec before data collection. With appropriate warm-up periods, both lasers had stable output power, which was reflected in the stable fluence rate measurements over 4 min (Table 3). These data again demonstrated that the 904 nm wavelength superpulsed laser, after a proper warm-up period, did not cause an increase in light transmission through the skin over time.
The fluence rate of the lasers was measured using a proper warm-up protocol as described above. The percentage of transmitted fluence rates of 810 nm wavelength and 904 nm wavelength superpulsed light through skin and muscle and skin alone was calculated (Table 4). The percentages of transmitted fluence rates through muscle and skin were 7.42% and 4.01% for 810 nm wavelength light and 904 nm wavelength superpulsed light, respectively. The percentages of transmitted fluence rates through skin were 24.63% and 19.94% for 810 nm wavelength light and the 904 nm wavelength superpulsed light, respectively (Table 4). These percentages through the skin were stable over 4 min of measurements (Fig. 2). These data demonstrate that transmission of superpulsed 904 nm wavelength light through muscle and skin or skin only is lower than transmission of CW 808 nm wavelength light. Therefore, the reported increase in penetration of 904 nm wavelength light from a superpulsed laser over time was an artifact due to insufficient warm-up time.
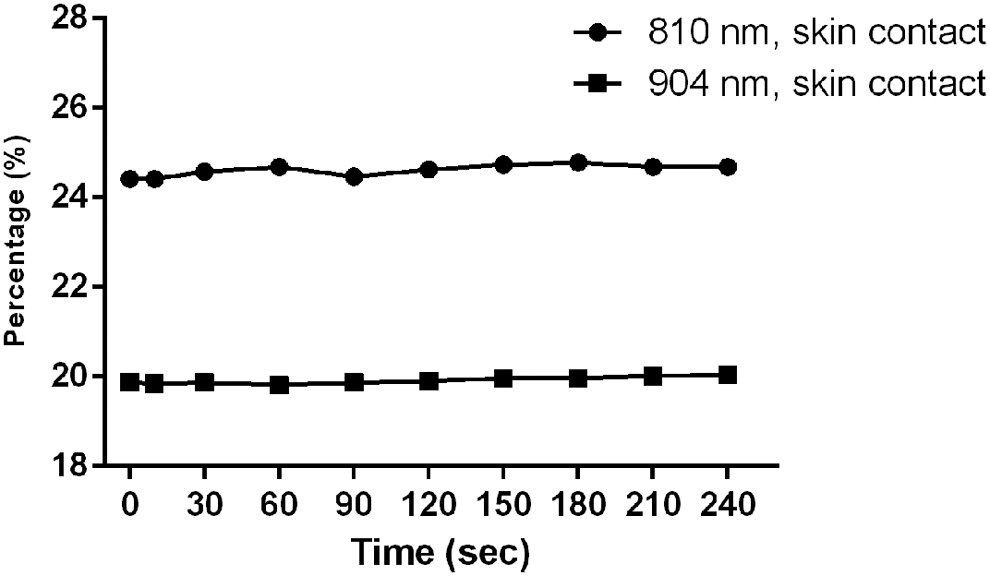
Comparison of the percentage of transmitted fluence rates of 810 nm wavelength CW and 904 nm wavelength superpulsed light penetration through the skin from one set of measurements. The detector was placed in the fascial plane deep into the dermis and fluence rates were measured at 0, 10, and 30 sec, and then every 30 sec for a total of 4 min. Both lasers had stable fluence rate measurements over 4 min after a proper warm-up period.
CW, continuous wave.
Output power of the 904 nm wavelength superpulsed light stabilizes after an operation period of 13 min
The output power of the 810 nm wavelength laser and the 904 nm wavelength superpulsed laser was measured for 20 min (four 5-min sessions). The output power of 810 nm wavelength laser was stable over the 20 min of measurements. The output power of the 904 nm wavelength superpulsed laser was relatively stable for the first 5-min session, but began to increase after 9 min and continued to increase by 29% through 13 min of measurements, at which point it stabilized (Fig. 3). The same pattern of initial stability of the laser, followed by an increase, then stabilization was found for both the fluence rate and output power measurements. Therefore, the observed increase was due to the laser reaching stability during the first 15 min of operation.
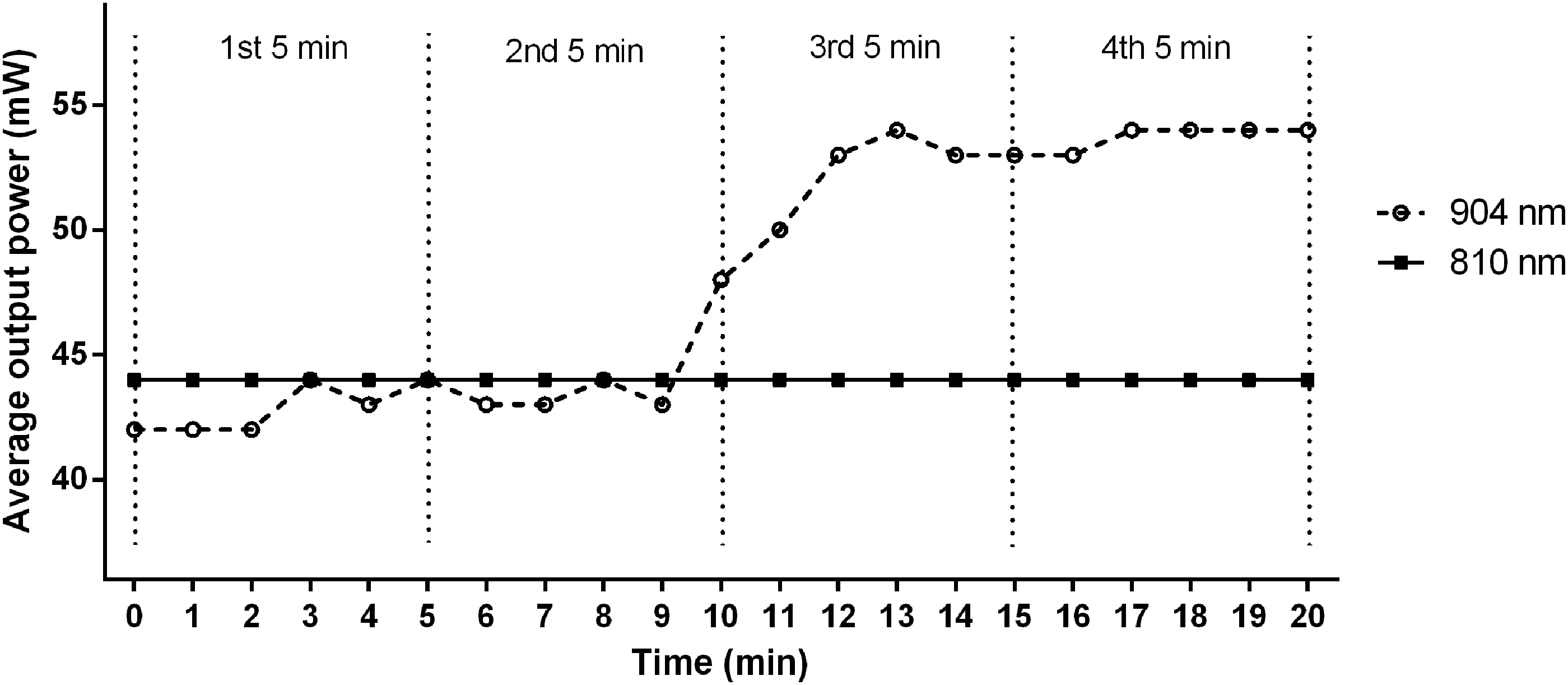
Comparison of stability of output power for 810 nm wavelength CW and 904 nm wavelength superpulsed lasers. The output power of both lasers was measured every minute through four 5-min sessions for a total of 20 min. The output power of 810 nm wavelength laser was stable over the 20 min of measurements. In contrast, the output power of the 904 nm wavelength superpulsed laser began to increase after 9 min and continued to increase by 29% through 13 min, at which point it stabilized for the remainder of the measurements.
Discussion
The data in this article demonstrate that transmitted fluence rate of superpulsed 904 nm wavelength light through muscle and skin or skin only is not increased over time due to photobleaching of the skin. The initial increase in light transmission measurement values of the superpulsed 904 nm wavelength laser was due to the fact that during the first 10 min of operation, the laser was warming up and had not stabilized at its maximum mean output power. Once the laser output power stabilized, there was no increase in the transmitted light fluence rate measurements. Further, the data prove that the transmission of CW 810 nm wavelength light through muscle and skin and skin alone is greater than the transmission of superpulsed 904 nm wavelength light. It is important to note the similarities and differences between Joensen's and the current experimental design. The 904 nm wavelength superpulsed laser used in this study is the same model laser used by Joensen et al. 21 The differences in the two measurement methods are in the current study, living anesthetized rats were used instead of excised skin samples; measurements in this study were made with the sensor at two locations in the rat's thigh, under the skin and under the gastrocnemius muscle; and the current data were based on transmitted fluence rate instead of the percent of transmitted output power.
The interpretation of the data made by Joensen et al. is understandable 21 based on the fact that their measurements were collected immediately after turning on the lasers and the data collection was restricted to 150 sec. However, based on that interpretation, the authors introduced time into the concept of light penetration and referred to the increased light penetration that they observed as penetration–time profiles. 21 They defined this term as linear increase in amount of energy passing the skin during an irradiated dose from a superpulsed laser and concluded that processing time is an interesting parameter of PBM with superpulsed lasers. 21 In a nonpeer-reviewed publication, this concept was expanded upon and referred to as the depth of penetration–time profile. 24 However, it is important to stress the following: (1) when the laser reached stability in our experiment, there was no linear increase in light transmission values of the superpulsed 904 nm wavelength light and (2) the equation for penetration depth, (δ)v = √{1/[3 μa (μa + μs(1−g))]}, where μa = absorption coefficient, which is dependent on wavelength, μs = scattering coefficient, which is dependent on wavelength, and g = anisotropy of the tissue, does not include any time dependence.
As mentioned previously, a number of studies have demonstrated that CW 904 nm wavelength light does not penetrate deeper into tissue than 810 nm wavelength light. 19,20 This fact led the authors to hypothesize that the increased penetration they observed was due to the superpulsing causing photobleaching of some skin element. A pulsed laser in the msec to 10 msec range can achieve localized heating of blood vessels, so there can be an enhanced effect on vasculature, while sparing overall heating of the tissue. 25 A femtosecond laser used with 100-femtosecond pulses could interact with local clusters of absorbing chromophores to cause transient photobleaching. However, the GaAs diode lasers are in the 100–200 ns range. Pulses in this range are probably too slow to cause transient photobleaching of chromophores (personal communication with Dr. Steven Jacques).
In a study on the relationship between penetration of superpulsed 904 nm wavelength light and skin pigmentation, light penetration (expressed as % of output power) through the thenar web of the hand of human volunteers was measured. 26 The volunteers had a range of skin color values based on the Fitzpatrick scale. 26 Light penetration significantly decreased with increasing melanin content. According to Jacques, the volume fraction of the epidermis occupied by melanosomes is 1.3–6.3% in light-skinned adults, 11–16% in moderately pigmented adults, and 18–43% in darkly pigmented adults. 27 The authors concluded that for each Fitzpatrick scale point of skin pigmentation after a value of 2, there was a 6% decrease in penetration and no photobleaching effects were noted. 26
PBM and PBMT are an emerging and rapidly expanding area of photonic research and therapeutic development. Currently, the risk to growth and acceptance of PBMT as an effective and safe therapy is the development and marketing of devices without a concurrent development of expertise and dissemination of fundamental knowledge in biomedical optics and photonics. For this field to continue to grow, scientific accuracy in PBM basic research, clinical translation, and device development must be assured. Therefore, it is essential that depth of penetration of various wavelengths of light and the effects of pulsing on tissue be thoroughly investigated.
Conclusions and Summary
The data in this article clarify that transmission of superpulsed 904 nm wavelength light through muscle and skin or skin only is not increased over time and there is no observation of photobleaching of the skin. The initial increase in transmitted fluence rate measurement values of the superpulsed 904 nm wavelength laser was due to the fact that during the first 15 min of operation, the laser was warming up and had not stabilized at its maximum mean output power. Once the laser was stabilized and the measurements were done, there was no increase in the fluence rate measurements. Further, the data prove that the transmission of CW 810 nm wavelength light through muscle and skin and skin alone is greater than the transmission of superpulsed 904 nm wavelength light.
Footnotes
Acknowledgments
The opinions and assertions contained herein are the private ones of the authors and are not to be construed as official or reflecting the views of the Department of Defense or the Uniformed Services University of the Health Sciences. The authors thank B&W Tek, Inc., and Irradia for providing the lasers used in this study. B&W Tek, Inc., also designed, produced, and supplied the near-infrared detector. Our sincere thanks to Ilko Ilev, PhD, CDRH, FDA, for his expert and thoughtful discussions and editorial comments on this article.
Author Disclosure Statement
J.J.A. received grant funding and Cooperative Research and Development Agreement (CRADA) between USUHS and LiteCure LLC, Lumithera, Inc., PhotoThera, Inc., and Nitto Denko, Inc.; received equipment from B&W Tek, Inc., Irradia, LiteCure, Nitto Denko, and PhotoThera; travel expenses were paid by Companion Animal Health®, LiteCure LLC; received royalties from Banyon Biomarkers and PhotoThera; holds intellectual property rights with Henry M Jackson Foundation; serves on the Advisory Board for Companion Animal Health, LiteCure LLC and Lumithera, Inc.; and served as Officer or Director for ASLMS. X.W. received salary support through a CRADA between USUHS, The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., and LiteCure, LLC.