
Abstract
Introduction
C
Diabetic individuals can develop impaired wound healing due to alterations in one or more biological mechanisms of the healing processes. Impaired wound healing can be activated by hyperglycemia, chronic inflammation, micro- and macro-circulatory dysfunction, hypoxia, autonomic and sensory neuropathy, and impaired neuropeptide signaling. 3 According to the American Diabetes Association (ADA) and the World Health Organization (WHO) criteria, 4 a fasting blood glucose higher than 126 g/dL is an important risk factor for postoperative sternal complications that can increase morbidity and mortality. 5 Additionally, undergoing CABG surgery that involves the anastomoses of the left internal mammary artery (LIMA) to the left anterior descending artery is believed to increase the risk of deep sternal wound infections. 6
Studies on diabetic and non-diabetic animals and human clinical trials have been conducted to evaluate the low-level laser therapy (LLLT) photobiomodulation on wound healing, 7,8 including saphenectomy after CABG. 9 LLLT has become an effective therapeutic resource for promoting tissue repair; some researchers have asserted the advantages of this coherent light source, because it provides more power density in the target tissue, and it maximizes irradiance by reducing reflection and increasing penetration into tissues with regard to light collimation. 10 In contrast, light-emitting diode (LED) devices are systems that produce non-coherent, monochromatic, and clean light when energized. They have also been increasingly studied to assess their therapeutic properties. 11,12 Some laboratory and clinical studies have reported that LED therapy exhibits a wide variety of effects, including pain relief, 13 inflammation reduction, 13,14 and tissue repair in both diabetics and non-diabetics. 15,16 LED therapy and LLLT at red wavelengths and energy density around 2.5–10 J/cm2, or even more, have been used to irradiate surgical incisions and accelerate postoperative recovery. 17,18
This study aimed at analyzing the healing effects of LLLT (λ620 nm, 6 J/cm2) and LED therapy (λ640 nm, 6 J/cm2) on the longitudinal sternotomy incisions of hyperglycemic and normoglycemic patients who underwent CABG.
Materials and Methods
All of the subjects signed a written declaration of informed consent, and their rights were protected. The protocol for this study was approved by the local research ethics committee CAAE 0180.0.415.000-11 and registered at the Brazilian Clinical Trial Registry and the International Clinical Trials Registry Platform of the WHO under RBR-38wgx6 and Universal Trial Number U1111-1128-9666, respectively.
This was a randomized, double-blind clinical trial containing both a placebo and a control group. The study was conducted in a private hospital that performs cardiac surgery for the Brazilian public health system. All of the patients admitted to the hospital during the study period who were scheduled for CABG and met the inclusion criteria were invited to participate. The study included 120 volunteers who were randomly allocated into one of four different groups of equal size (n = 30 each group): control, placebo, laser, and LED groups. Each group was also separated into subgroups of hyperglycemic and normoglycemic subjects, based on their preoperative fasting blood glucose levels, according to the ADA and WHO criteria. 4
The study participants underwent elective coronary artery bypass surgery with a longitudinal sternotomy incision and extra-corporeal circulation, with anastomoses of the LIMA to the left anterior descending artery. When necessary, saphenous vein grafts were used to anastomose the other coronary arteries. Patients between 18 and 75 years of age, of both genders, who were hemodynamically stable and had a body mass index (BMI) <29.9 kg/m2 were included. The exclusion criteria were: (1) a diagnosis of type I diabetes mellitus; (2) a diagnosis of type II diabetes mellitus made within the past 2 years, or not being under regular treatment with hypoglycemic drugs; (3) previous thoracic surgery; (4) emergent or urgent coronary artery bypass surgery; (5) respiratory insufficiency after surgery manifesting as hypoxemia with a partial pressure of oxygen in arterial blood <60 mmHg; (6) renal insufficiency with serum creatinine ≥1.8 mg/dL after surgery; (7) low cardiac output syndrome with ST segment elevation in multiple electrocardiogram leads, cardiac arrhythmias, or hypotension, according to the American College of Cardiology Foundation and the American Heart Association; 19 and (8) clinical complications that demanded changes in the analgesic protocol. Individuals who could not be followed during the first month after the operation were also excluded.
The randomization was completed by simply drawing cards marked 1 for the control group, 2 for the placebo group, 3 for the laser group, or 4 for the LED group. The drawing was performed during the patient's hospital admission, which always occurred at least 24 h before the surgery. The researchers themselves were either therapists or evaluators. The therapists were the assistants who were responsible for conducting the therapy and registering the procedures, and the evaluators were responsible for assessing the patients and their results. Each patient was identified by a code that was registered by one of the therapist researchers, who ensured that the evaluating researchers remained blinded until the final statistical analysis was performed. The patients were blinded to the study by the use of opaque goggles during the laser and LED irradiation treatments.
On the day before the surgery, the patients underwent a preoperative assessment, which consisted of an explanation of the procedures and the study inclusion and exclusion criteria. The exclusion criteria were reviewed every postoperative day, and they included (1) clinical assessment; (2) arterial blood sampling, performed on the radial artery, to measure the partial pressure of oxygen; (3) serum creatinine; (4) electrocardiogram monitoring; (5) mean arterial blood pressure measurement; and (6) fasting blood glucose test. The analgesic protocol was the one routinely used by the hospital and consisted of tramadol hydrochloride and dipyrone administered intravenously on a fixed 6-h schedule. Morphine sulfate was administered on an as-needed basis. Patients who received morphine were excluded from the study.
The experimental groups (laser and LED) underwent irradiation immediately after surgery and on postoperative days 2, 4, 6, and 8. The irradiation was performed at eight spots along the incision that were 2 cm from each other. The probe was positioned perpendicularly and in contact to the skin, and it was protected by a translucent film. The equipment characteristics and irradiation parameters are described in Table 1. The placebo group underwent the LED application process but with the equipment turned off. The control group only underwent the assessment protocol and the follow-up.
SAEF, power output × time treatment per point × point numbers/total treated area.
Manufacturer: MMOptics, Jardim São Carlos, São Carlos.
Manufacturer: Microdont, São Paulo, Brasil.
LED, light-emitting diode; SAEF, spatial average energy fluency.
The outcomes evaluated were incision healing as measured by hyperemia and incision closure, based on the evaluators' review of the photographs registered on the first day after hospital discharge, which occurred on the eighth postoperative day.
The evaluating researchers completed a training program to guarantee intra- and inter-examiner agreement and to calibrate their level of concordance. The incisions were photographically registered immediately after the surgery and 8 days afterward for the retrospective analysis. A 14-megapixel resolution Alpha 390 Sony camera was used, which automatically focused macro perpendicularly to the chest incision. The researchers developed a score scale according to the following signs: (a) hyperemia: zero normal skin color, one pink skin, two red, and three purple; (b) incision edge closure: zero complete closure, one minor bleeding, two minor dehiscence, and three complete dehiscence. The images were analyzed by three different people (A, B, and C). The results were blindly registered by the researchers and statistically analyzed by an independent statistician who organized the data into groups for comparison. The patients were followed for 1 month after surgery, and the incidence of sternum dehiscence was evaluated during this period.
The study results were evaluated using the software STATISTICA 7.0 StatSoft©. Kappa concordance test was conducted for three different measurers (A, B, and C) who assessed the incisions for hyperemia and surgical wound closure based on the photographs registered on the first day after hospital discharge. Intergroup comparisons were performed by the Kruskal–Wallis test, and multiple comparisons were performed by the Dunn's test. The intragroup comparison was performed using the Mann–Whitney U-test. All of the significance levels were set at p ≤ 0.05.
Results
A total of 120 patients were enrolled in the study, and their anthropometric characteristics are described in Table 2. No significant differences in age, weight, height, or BMI were found among the groups. Individuals with a fasting blood glucose higher than 126 g/dL were considered hyperglycemic according to the ADA and WHO criteria. 4 There were 12 hyperglycemic subjects in the control group, 11 in the placebo group, 11 in the laser group, and 11 in the LED group. According to preoperative clinical records, all of the participants were receiving antihypertensive agents; the different drug classes included thiazide diuretics, calcium channel blockers, angiotensin II receptor antagonists, and beta blockers.
BMI, body mass index.
Concordance test for photographic analysis
Three different measurers (A, B, and C) blindly reviewed the photographs of the sternotomy incisions that were registered on the first day after hospital discharge; their agreement was measured by the Kappa concordance test (Table 3), and it demonstrated a strong concordance (minimum 0.721 and maximum 0.959), p ≤ 0.0001.
Values higher than 0.7 represent a strong concordance. All comparisons presented p ≤ 0.001.
Kruskal–Wallis test intergroup by three different measurers
The photographs were organized and printed on cards and they were then randomly mixed for the measurers. The patients were identified by their specific codes. Figure 1 demonstrates that on the eighth postoperative day, the patients who received LLLT and LED therapy had better improvements in hyperemia and incision closure, as well as in their total score, when compared with the control and placebo groups (p ≤ 0.05). The results were similar in both the hyperglycemic and normoglycemic subgroups.
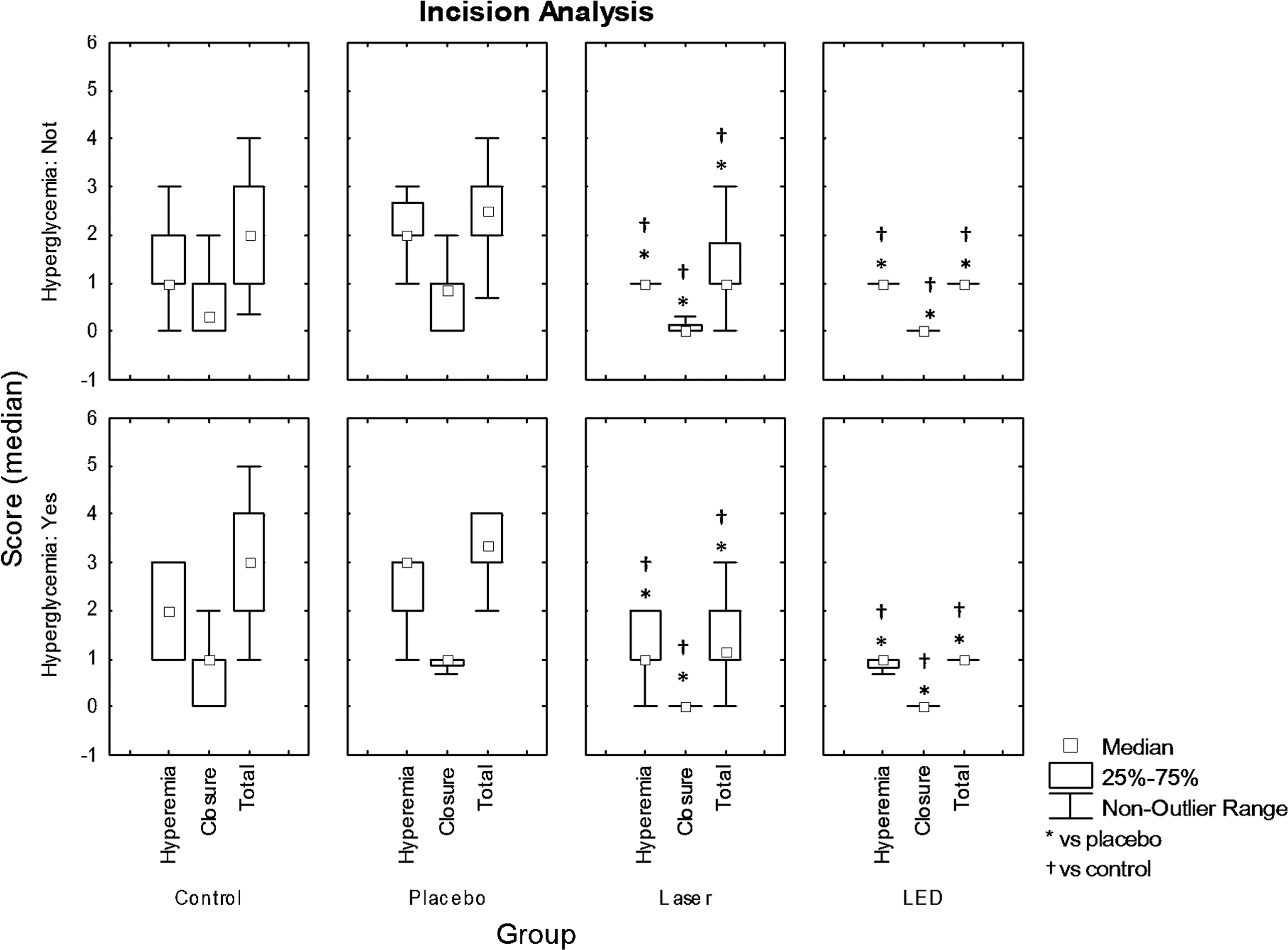
Incision healing analysis graphs, examining hyperemia and wound closure in hyperglycemic and normoglycemic patients, comparing the placebo, control, laser, and LED groups. A Kruskal–Wallis test and a multiple-comparison test by Dunn were performed for the mean of the values registered by three different measurers. Values are given as the mean ± 0.95 × standard error. LED, light-emitting diode.
Normoglycemic and hyperglycemic intragroup comparison
Table 4 illustrates the Mann–Whitney U-test results comparing the hyperemia response and incision closure in the normoglycemic versus hyperglycemic intragroups. The results suggest that there were no statistical differences between these subgroups. These findings indicate that normoglycemic and hyperglycemic individuals had similar responses, regardless of whether they received phototherapy or not. Nevertheless, statistical evidences were not observed in the test; clinically normoglycemic patients had better results when compared with hyperglycemic patients. It is important to note that each evaluator blindly assessed the images and independently registered their assessments. The reported results were then compared between the normoglycemic and hyperglycemic subgroups. The same analysis was performed on each group independently (control, placebo, laser, or LED).
Mann–Whitney U-Test. Marked tests are significant at p <0.05.
The results of the sternotomy assessments comparing the hyperglycemic and normoglycemic subgroups on the first day after hospital discharge are illustrated in Fig. 2.
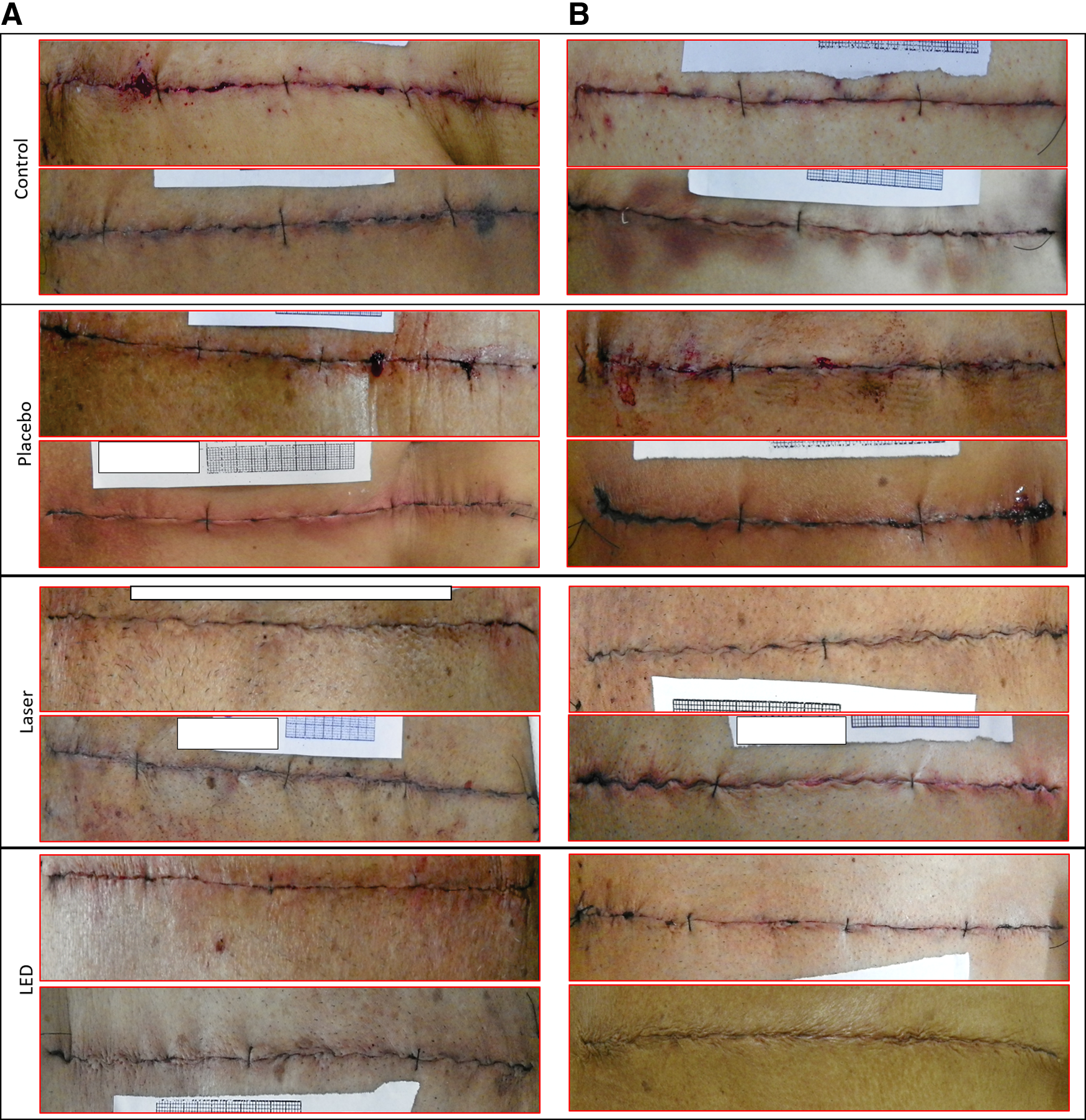
Images of incisions analyzed in terms of hyperemia and incision closure. The images were registered on the first day after hospital discharge, which occurred on the eighth day postsurgery.
No patients were withdrawn from the study due to surgical complications such as respiratory or renal insufficiency, low cardiac output syndrome, or any clinical complications that demanded changes in the analgesic protocol. Sternotomy dehiscence occurred in one individual in the placebo group and in two of the control group patients during the first month after the operation. None of the patients who underwent LLLT or LED therapy developed dehiscence. At the 1-month follow-up evaluation, all of the patients who did not experience dehiscence demonstrated good incisional healing without edema, erythema, other signs of inflammation, or wound healing delay.
Discussion
The present study analyzed the healing effects of LLLT and LED therapy on the longitudinal sternotomy incisions of hyperglycemic and normoglycemic patients who underwent CABG with LIMA. Hyperglycemia may be responsible for postoperative complications after CABG, such as wound healing delay as well as pain, due to its neurological involvement. Further, the surgical approach that involves anastomosing the LIMA to the left anterior descending artery is believed to increase the risk of deep sternal wound infection, 6 which can delay the healing process, aggravate inflammation, and increase pain.
According to Gurtner et al. 20 problems with wound healing in humans include either delayed wound healing or excessive healing. Delayed wound healing can be due to diabetes or radiation exposure. Postoperative sternal complications, such as wound infection, mediastinitis, and suture dehiscence, can increase mortality, prolong hospital length of stay, and increase the costs of treatment. 21,22 Prevention of sternal complications is essential to make the surgical procedure safer. 17
Hyperglycemia can impair wound healing by affecting one or more of the biological mechanisms in the healing processes. Most often, it is triggered by hyperglycemia, chronic inflammation, micro- and macro-circulatory dysfunction, hypoxia, autonomic and sensory neuropathy, and impaired neuropeptide signaling. 3 Delayed healing describes wounds that fail to close in a reasonable period; usually, wounds that fail to heal after a 12-week period are considered chronic. 23
Dyslipidemia, high blood pressure, and a high BMI increase the risk of diabetic neuropathy. Most of the participants in the present study were overweight (Table 2) and had concomitant hypertension, placing them at higher risk for postoperative complications such as impaired sternotomy healing, although none of the participants presented with decompensated hyperglycemia. Nonetheless, according to Bădescu et al., 24 diabetic peripheral neuropathy can develop despite intensive hyperglycemic control. There are two theories about how hyperglycemia affects nerve conduction: One suggests a metabolic mechanism, and the other suggests a vascular mechanism. The metabolic theory presumes that complex processes such as oxidative stress and glycosylated proteins reduce the speed of nerve conduction. 25 The vascular theory presumes that arteriolar narrowing, venous distension, arterial and venous shunts, and vascular neo-formation result in hyperplasia and hypertrophy, denervation, and reduced neuropeptide expression in epineurial vessels. 26 Since hyperglycemic patients have a higher risk of sternotomy dehiscence, it is crucial to have their incisions carefully monitored.
Numerous researchers have reported on the use of photography to assess wound healing. In fact, one of the most basic and yet powerful tools in any wound clinic is the visual observation of the wound site. Images of whole wounds can offer much greater information than single-target diagnostics, 27 particularly with the technological advances in digital images. Even though it is a reliable technique, one of its limitations is the subjective assessment of the qualitative wound characteristics, whether viewed in person or through digital photographs, which can influence wound assessment agreement. 28 Notwithstanding the subjective limits of this technique, in the present study, the Kappa concordance test (Table 3) of the three blinded evaluators demonstrated a strong concordance among them, indicating that this assessment procedure for wounds was reliable for the sternotomy incision analysis.
Figure 1 depicts the results of the three blinded evaluators who assessed the incision images of the intergroup. The images of the hyperglycemic patients were separated from those of the normoglycemic patients, and the analyses were performed independently. The reported results demonstrated that the laser and LED groups experienced greater improvements in hyperemia and incision closure than the placebo and control groups did (p ≤ 0.05), according to the Kruskal–Wallis analysis, with multiple comparisons analyzed by the Dunn's test. Comparable results were found in both the hyperglycemic and normoglycemic subgroups. These outcomes indicate that LLLT and LED therapy can beneficially accelerate the process of sternotomy healing. These complementary, photobiomodulation techniques presented similar effects with LLLT and LED therapy, which suggest that these two therapeutic techniques have analogous effects (Fig. 1).
The analysis of the hyperemia response and incision closure in the intragroup comparison of the normoglycemic versus hyperglycemic patients (Table 4) indicated that there were no statistical differences between them (p ≥ 0.05), according to the Mann–Whitney U-Test. These outcomes indicate that there were similar healing responses in both the normoglycemic and hyperglycemic individuals. Nevertheless, overall, the irradiated groups had better results. These findings are comparable to the results reported by Dall Agnol et al., 16 which suggest that coherent and non-coherent phototherapy have similar effects. It is important to note that each blinded evaluator assessed the results independent of registering their outcomes. The findings were compared one by one among the normoglycemic and hyperglycemic subgroups. The analyses were performed within each group independently (control, placebo, laser, or LED).
Many researchers have reported on the use of coherent (LLLT) and non-coherent (LED) phototherapy for tissue healing in diabetic and non-diabetic rats 8,16 and humans, 7,29 and they have concluded that photobiomodulation with laser and LED produces similar effects. Doses in the range of 0.3–19 J/cm2 (median dose 7.5 J/cm2) have been used in studies that are aimed at inflammation and pain modulation with LED therapy and LLLT. 30 Oliveira 12 used LED therapy 6 J/cm2 and Carvalho 31 used LLLT at the same dose, and they observed inflammation modulation and tissue repair, which resulted in an increase in tissue resistance to rupture and deformation. In a clinical trial with 40 participants, Chavantes and collegues 17 studied LLLT for the prevention of sternotomy dehiscence. Their results indicated that patients in the placebo group had five times more sternotomy suture dehiscence when compared with the LLLT-irradiated group, and they concluded that the therapy was effective when it was instituted during the initial inflammatory phase after surgery. In their trial involving 90 volunteers who underwent CABG and were irradiated with 640 nm LED on sternotomy incision, Oliveira et al. 32 concluded that LED therapy had an analgesic effect, increased incision healing, and prevented dehiscence. The results with LLLT and LED therapy have been analogous in many studies, indicating that both LLLT and LED therapy can reduce pain and promote tissue modulation and wound healing in multiple ways.
The mechanisms involved in enhanced tissue repair with LLLT and LED therapy include an increase in the number of dividing cells and increases in the levels of inducible nitric oxide synthase, keratinocyte growth factor, and keratinocyte growth factor receptor, which may facilitate earlier and thicker re-epithelization. 33 At doses of 5–6 J/cm2, LLLT can stimulate the production of bFGF, a multi-functional polypeptide that supports fibroblast proliferation and differentiation. Further, high doses suppress bFGF. 34 The effects of the laser and LED sources were comparable when equal therapeutic doses of light were applied. The result was an improved healing process, which can be observed on sternotomy incisions after a protocol of irradiation.
Conclusions
In this study, we investigated the effect of a protocol using LLLT and LED therapy, with 6 J/cm2, on tissue repair in hyperglycemic and normoglycemic patients who underwent CABG with a longitudinal sternotomy. With these therapy parameters, we observed that both coherent light (laser) and non-coherent light (LED) accelerated the sternotomy incision healing assessed on the eighth postoperative day.
The limits of this study were the use of only one parameter of wavelength and energy density for both light sources, the different characteristics of the equipment used, such as wavelength, spot size, and power, and the subjective discernment of the qualitative wound characteristics analyzed through the photographs. Additional studies should be performed that compare glycated hemoglobin (HbA1c) levels, a useful longer-term gauge of blood glucose control, to verify the effectiveness of LLLT and LED on the healing process and pain control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.