
Abstract
Introduction
P
The erbium, chromium: yttrium–scandium–gallium–garnet (Er,Cr:YSGG) laser has a wavelength of 2.78 μm, and most commercial units provide up to 6.5 W of power, enough for removal of tooth structure and cavity preparation in restorative dentistry. 4 The wavelength of light energy provided by erbium lasers is highly absorbed by water so when the laser is directed at biological tissues, the water within the hard or soft tissues rapidly heats and turns into steam, producing an ablation of the tissue surface to a depth related to the laser wavelength and the water content of the tissue. However, the lower power settings of commercially available Er,Cr:YSGG lasers are suitable for soft tissue cutting and coagulation. Further, commercial versions of the Er,Cr:YSGG laser provide a cooling water spray that is directed with the laser, minimizing overheating of hard and soft tissues. During subgingival debridement with laser energy, it is hypothesized that the water spray will aid the physical separation of the plaque and calculus in the periodontal pocket, and it has been shown that high-speed jet flow facilitates fast cleaning and prevents the laser from causing thermal damage. 5,6 Recently, a series of studies have indicated that erbium lasers can be used as an effective therapy for removal of plaque, calculus, and diseased cementum. 7 –10 Er,Cr:YSGG therapy has also been demonstrated to have bactericidal effects on the surfaces of roots affected by periodontal disease 11 and to stimulate new bone formation in the furcation area in experimental periodontitis. 12
To assess the clinical effect of the Er,Cr:YSGG lasers in the treatment of moderate-to-advanced root furcation lesions involved in chronic periodontitis, in this study, the clinical efficiency of an Er,Cr:YSGG laser was compared to that of conventional manual subgingival debridement in patients with chronic periodontitis.
Materials and Methods
Subject selection
Thirty-one patients were recruited from the Department of Periodontology, Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine. The study was conducted in accordance with the ethical standards of the Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine. Signed informed consent was obtained from all patients before the start of the treatment.
Inclusion criteria: (1) a clinical diagnosis of moderate-to-severe chronic periodontitis based on the new periodontal disease classification system released in 1999 13 ; (2) the extent of the periodontitis included at least 4 M in at least two dental quadrants where periodontal probing depths (PD) ≥4 mm in the area of the root furcations were associated with moderate (degree II) or severe (degree III) furcation involvement of the molars; (3) no fewer than 18 teeth remained in each patient's mouth; (4) no systemic diseases were present that would affect periodontal treatment; (5) female patients were not pregnant and had no intention of becoming pregnant during the study; (6) no history of smoking; and (7) no use of antibiotics during the month immediately before the study.
Study design
The study was performed according to a split-mouth design (Fig. 1). All patients who were candidates for the study were educated about dental health and supragingival scaling. One week later, an ultrasonic scaling instrument (Electro Medical Systems) was used to remove the subgingival calculus on all teeth in the mouth. All patients were re-examined 2 weeks later to record the PD measuring the distance in mm from the gingival margin to the bottom of the periodontal pocket at six sites (mesiofacial, midfacial, distofacial, mesiolingual, midlingual, and distolingual) around the perimeter of each tooth. Baseline values of PD, clinical attachment level [clinical attachment loss (CAL) in mm], and bleeding on probing (BOP) were recorded for every site.
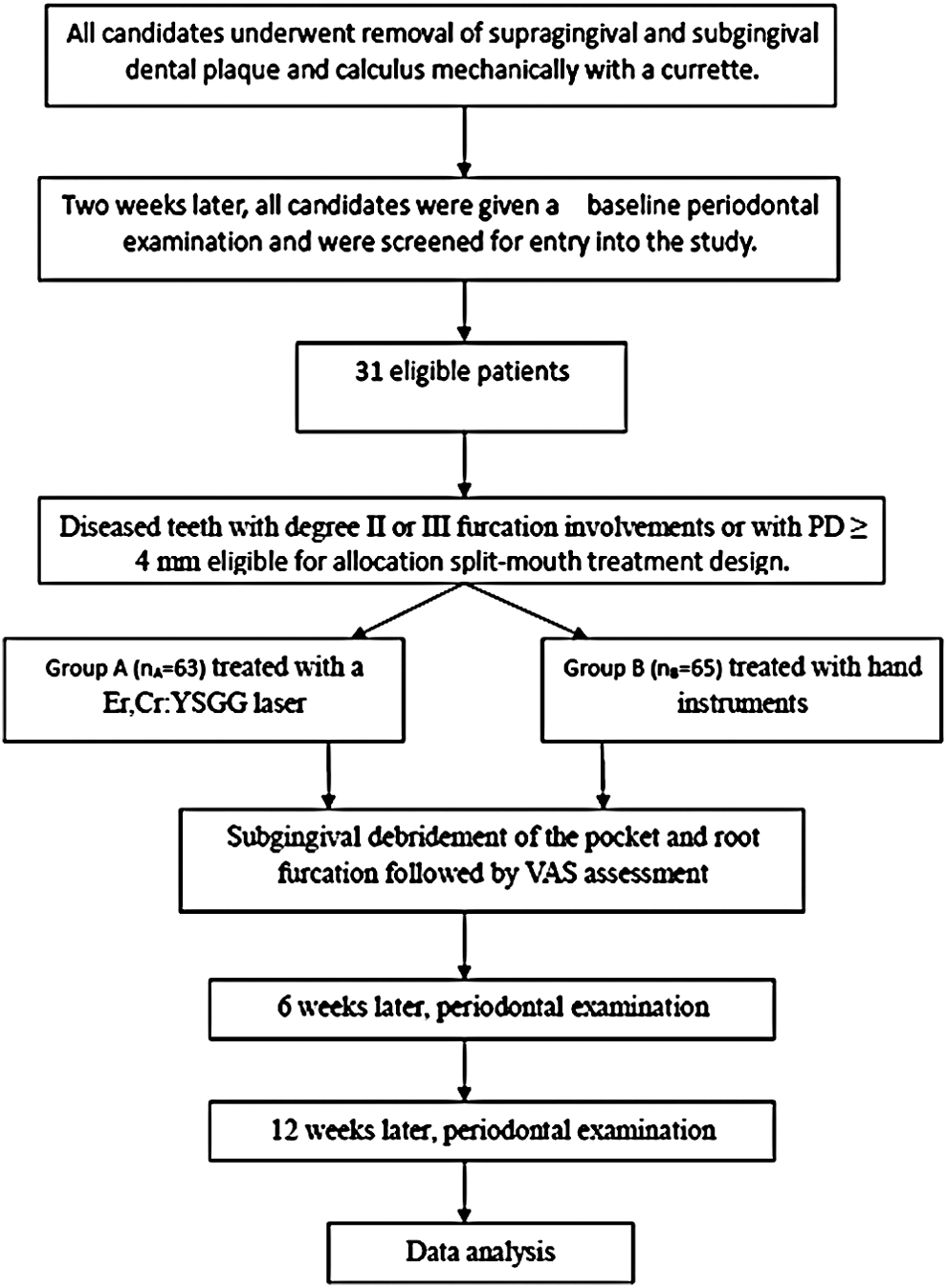
Study design from screening to completion of the trial. After baseline treatment, screening, and periodontal examination, diseased teeth were randomly assigned to group A or B. Patients were treated with Er,Cr:YSGG laser or with hand instruments (Gracey curettes) for subgingival debridement of periodontal pockets and root furcations and then re-examined 6 and 12 weeks later. Clinical periodontal parameters of gingival BOP, PD, and CAL at each examination were obtained and analyzed. BOP, bleeding on probing; CAL, clinical attachment level; Er,Cr:YSGG, erbium, chromium: yttrium–scandium–gallium–garnet; PD, probing depth.
For the candidates who met all of the inclusion criteria and were recruited into the study, split-mouth treatment conditions were randomly assigned. Sites with moderate-to-advanced disease parameters (Class II and III furcation involvements with PD ≥4 mm) on one side of the mouth were considered Group A and treated with the Er,Cr:YSGG laser (BIOLASE Technology, Inc., San Clemente, CA), while the sites with these moderate-to-advanced disease parameters on the other side of the mouth were considered as Group B and treated with hand instruments (Gracey curettes). Assignment of diseased teeth on each patient's left or right side to Group A or B was determined by random number assignment (odd/even) using the Microsoft Excel software.
A commercially available Er,Cr:YSGG laser system (Millennium System; BIOLASE Technology, Inc.) with a 2.78 μm wavelength equipped with an RFPT 5–14 fiber optic tip of 14 mm in length and a tip diameter of 500 μm was used in the study. The parameters of the laser were set as follows: output power of 1.25 W, pulse mode H for soft and hard tissue with bell-shaped, asymmetrical pulses (pulse width 60 μs), and a pulse frequency of 30 Hz, using a water spray volume of 25 mL/min.
For all diseased teeth included in the split-mouth design, the fiber optic head was moved around the periodontal pockets and across the surface of the root furcations, while debris was washed out of the periodontal pockets with flowing water and collected by a separate vacuum system. No local anesthetic was given at any time. Treatments were rendered by two separate periodontists; one periodontist performed hand instrumentation for every subject and the other periodontist performed laser therapy for every subject.
A visual analogue scale (VAS) assessment was performed immediately after treatment. 14 A 100 mm line was presented with its end-points representing “painless” and “severe pain.” The patient drew a perpendicular line to indicate the severity of pain he or she felt.
PD, CAL, and BOP of diseased teeth included in the split-mouth treatment design were recorded 6 and 12 weeks after treatment. To minimize variance in clinical probing data, all clinical measurements of diseased teeth in groups A and B were made by a single, well-trained, examiner using a Hu-Friedy PCP UNC 15 color-coded periodontal probe. The examiner was blinded to the treatment assignments.
Statistical analysis
Analyses were performed with a Statistical Analysis System (SAS 6.12; SAS Institute, Cary, NC) and clinical measurement data are expressed as mean ± standard deviation. PD, CAL, and BOP measurements made 6 or 12 months after laser or mechanical treatments were compared to baseline values in all diseased teeth using paired t-tests within each subject. The differences in variables between Group A and Group B were also compared directly at each time point using paired t-tests. Statistical significance was set at p < 0.05.
Results
General condition of subjects
Thirty-one patients with chronic periodontitis having bilateral molars with Class II or III furcation lesions and meeting all other criteria were included in the study. One patient was later excluded because that patient was given local infiltration anesthesia during treatment and could not complete the VAS. Diseased teeth in Group A (n A = 63) were treated with an Er,Cr:YSGG laser and diseased teeth on the other side of the mouth in Group B (n B = 65) were treated with hand instruments. Patients ages ranged from 24 to 72 years old (average 35.2 ± 9.8 years) and 17/30 were females. As shown in Table 1, the baseline clinical data showed no significant differences between Group A and Group B teeth. No adverse events were reported during the study.
Designates mean change in measurement within each site.
Compared with baseline.
Comparison of the changes of both groups.
Proportion of teeth with BOP.
*p < 0.05; † p < 0.01.
BOP, bleeding on probing; CAL, clinical attachment loss; PD, probing depth.
Clinical comparison of response to debridement with laser versus mechanical instrumentation
Following the split-mouth treatments of the diseased teeth, the treated teeth were clinically examined 6 and 12 weeks later to record PD, CAL, and BOP. The overall results are presented in Table 1.
For diseased molars with Class II or III furcation lesions and diseased sites with PD ≥4 mm at baseline, both treatment modalities were associated with inflammation reduction and periodontal tissue repair (Fig. 2). PD, CAL, and BOP in both groups were significantly decreased at week 6 and 12 after treatment compared with baseline (p < 0.01). The reduction of PD in the laser-treated group was greater than in the control group at both week 6 (p < 0.01) and week 12 (p < 0.05). CAL showed no significant difference between the two groups at week 6 or 12 (p > 0.05). The percentage of sites with demonstrated BOP in the laser-treated group (Group A) was significantly lower than the proportion with BOP in group B at week 6 and 12 (p < 0.05).
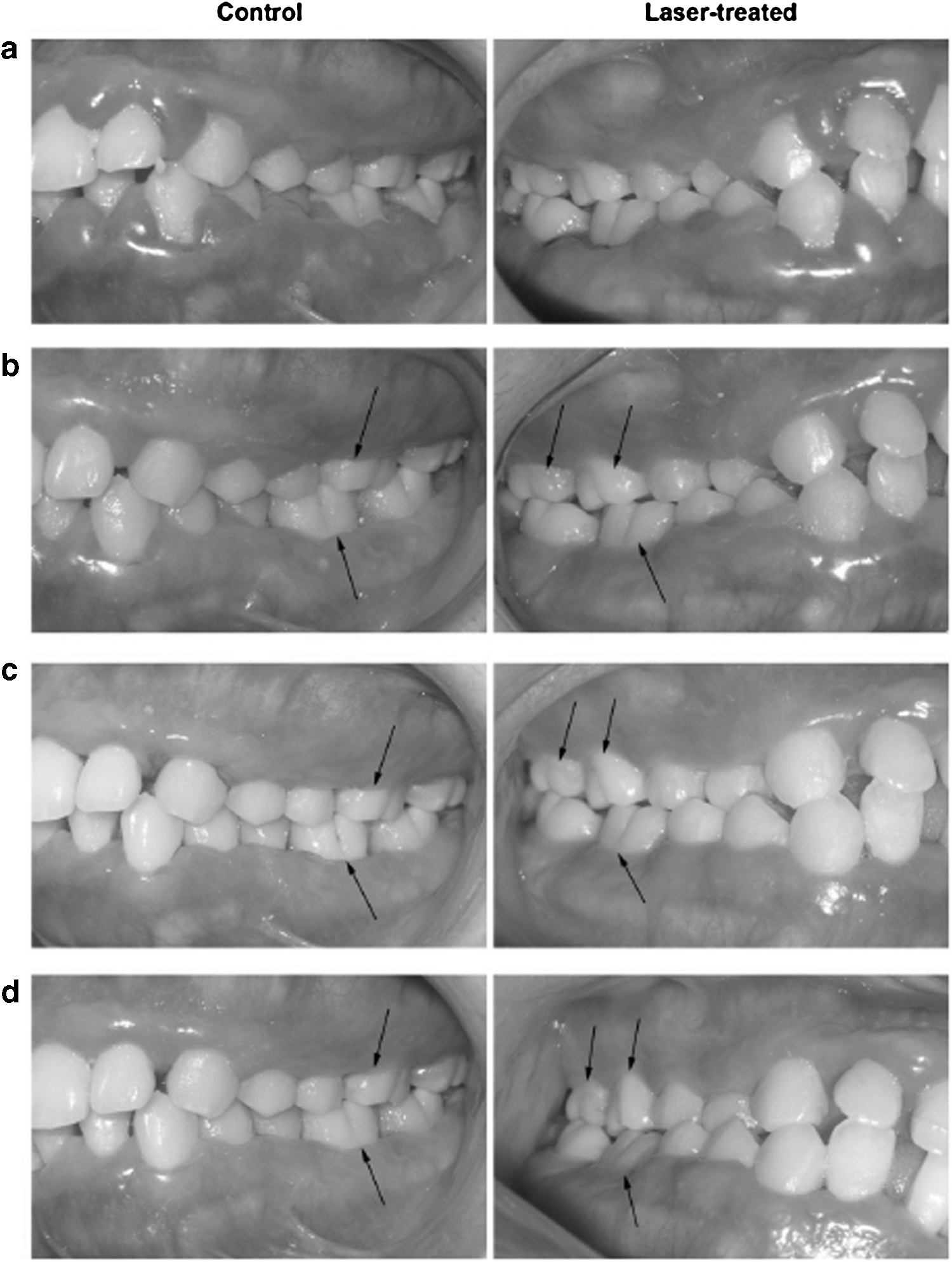
Pre- and postoperative clinical images of furcation involvements.
The number of sites in each group that presented with PD measurements of 3 mm or less was recorded at the 6- or 12-week follow-up examinations. Group A had 12 and 29 teeth dropping below the 3-mm pocket depth at 6 and 12 weeks after the treatment, respectively. Group B had fewer teeth dropping below the 3-mm pocket depth, the number being 5 and 16 for week 6 and 12, respectively.
Comparison of VAS evaluation between two groups of teeth
The VAS value for the laser-treated group (3.17 ± 0.79) was significantly lower than for the manually treated group (6.80 ± 1.21; p < 0.01).
Discussion
The concave anatomy of the root furcation renders it vulnerable to dental plaque accumulation, which can lead to development of a furcation lesion, periodontal pockets, and alveolar bone resorption. The disease process hastens as the lesion deepens and, with incomplete treatment, may cause loosening or loss of teeth. The development and prognosis of root furcation lesions are closely related to the anatomical and structural features of the roots of the involved teeth such as the length of the root trunk, the angle and width at the bifurcation, and the concave shape of the surface of the root. 15
The beginning of periodontal treatment is the most critical stage in the treatment of periodontal disease, and scaling, curettage, and subgingival debridement are the most important parts. During conventional periodontal treatment after supragingival calculus is removed with a scaler or ultrasonic device, a variety of sharp curettes allow the clinician to reach below the gingival margin to remove subgingival calculus and to remove the contaminated cementum surface of the root in a process called root planing. Root planing with curettes may inadvertently damage the root surface creating areas for bacterial accumulation or may completely remove cementum exposing the underlying dentinal tubules, which leads to sensitivity during and after treatment. Even though curettes can remove the unhealthy granulation tissue from the periodontal pocket, scraping and stretching of the soft tissue during treatment may induce the release of histamine and cause bleeding, edema, and pain. Also, therapeutic efficiency is limited for some anatomical locations deep within the periodontal pocket (such as the root furcation) that cannot readily be reached by traditional instruments. Longitudinal studies of periodontal therapy have confirmed that the prognosis for diseased teeth with furcation lesions is worse following traditional scaling. 16 According to a previous report, 17 58% of first molars have root furcation entrances smaller than 0.75 mm. The width of the blade of common subgingival curettes is 0.75 mm making it difficult to enter and clean the furcation entrance with these hand instruments. Further, the hard blade of the curettes is very different in shape from the concave root surface at the furcations. For this reason, even with open curettage, it is almost impossible to completely remove the dental calculus and plaque from sites with complex root anatomy using this kind of instrument. However, the removal of the calculus and infected cementum is a necessary precondition for a satisfactory outcome in periodontal therapy. 18,19
Periodontal laser therapy, as a supplementary means of traditional periodontal treatment, has seen widespread application. In several in vitro studies, Er,Cr:YSGG lasers were proven to be effective in removing calculus without causing detrimental effects to the surfaces of the roots. 20 They have also been found to exert bactericidal activity in root canals in addition to the mechanical removal of biofilm. 20,21 Moreover, the use of Er,Cr:YSGG laser has been shown to stimulate bone formation in the furcation area following subgingival treatment with the laser, indicating it may facilitate post-therapy bone healing. 12 However, few studies have been done to assess the clinical application of Er,Cr:YSGG laser in basic treatment of periodontal disease.
The current study has shown that pocket debridement using both laser and conventional methods can significantly decrease PD, CAL, and BOP in periodontal patients (p < 0.01, compared to baseline). The laser treatment showed better effects on PD changes at week 6 (p < 0.01) and week 12 (p < 0.05) and a greater reduction in BOP (p < 0.05) compared to hand instrumented sites in the same patient. No significant difference was observed in CAL between the two groups (p > 0.05). For this reason, it was here concluded that both Er,Cr:YSGG lasers and manual scaling could exert a notable therapeutic effect in periodontal pocket debridement, and laser treatment provided a better clinical outcome than did manual instrumentation. No short-term effect on periodontal regeneration was observed. Schwarz et al. reported that 6 months after treatment, both laser and hand-instrumented groups showed significant improvement in clinical parameters compared to baseline, and the improvement of BOP and CAL in a laser-treated group was better than in a hand-instrumented group. 22 Such results were generally consistent with observations made in the present study. In a previous study, results showed that for sites with baseline PD ≥6 mm, the reduction of PD at week 12 after treatment with the Er,Cr:YSGG laser was better than measured in control sites. 23 Together, these reports, including the present data, suggest that the Er,Cr:YSGG laser can provide a clinically effective outcome at complex anatomical sites such as deep periodontal pockets and root furcations.
An additional advantage of Er,Cr:YSGG lasers in periodontal pocket debridement is that thermal injury can be avoided (e.g., carbonization of root surface or fusion) so long as sufficient water mist cooling is used. 24 This helps prevent patients from feeling uncomfortable. An international VAS was used in this study to evaluate the degree of pain. In the split-mouth design used in this study where the initial degree of periodontitis severity on both sides was comparable, results showed that the VAS value for laser-treated and manually treated groups was 3.17 ± 0.79 and 6.80 ± 1.21, respectively, demonstrating significantly less pain perception for laser-treated teeth (p < 0.01). This was consistent with most previous reports 25,26 and suggests that the use of Er,Cr:YSGG may significantly increase compliance with periodontal treatment by reducing pain during periodontal treatment.
The Er,Cr:YSGG laser used in the study had an RFPT (Radially Firing Perio Tip) optical head specifically designed for dentistry. It allows vertical and radial (360°) excitation synchronously. The radial and vertical excitation account for 85% and 15% of the total excitation output, respectively. This output design can enable better coverage of the lesion within the periodontal pocket while treating the root furcation even when the angulation of the vertically directed laser cannot be made near tangential to the surface of the root. The laterally directed laser energy from the tip helps to ensure removal of inflammatory plaque while enhancing the safety of operation. While the design of the present study did not allow meaningful differential analysis between buccal, lingual, mesial, or distal furcations, given the simultaneous vertical and radial lesion coverage during instrumentation with the RFPT, it will be interesting to directly compare manual instrumentation outcomes with this laser therapy in future studies by us and others.
Conclusions
In this study, data indicated that the Er,Cr:YSGG laser was a safe, comfortable, and effective treatment for periodontal pocket debridement at root furcations and in deep periodontal pockets in patients with chronic periodontitis. While the Er,Cr:YSGG laser was clinically more effective than conventional hand instrumentation, it was also successful in initial periodontal therapy because it involved less pain and promoted good patient compliance. Long-term follow-up observations are warranted for further assessment of Er,Cr:YSGG lasers in periodontal clinical application.
Footnotes
Acknowledgments
This study was supported by the fund of Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine (2012-08).
Author Disclosure Statement
No competing financial interests exist.