
Abstract
Introduction
O
Low-level laser therapy (LLLT) acts through photophysical and chemical responses that promote biomodulation effects in the treated tissues and cells. This photobiomodulation can cause two types of effects, that is, biostimulation and/or bioinhibition responses. 2
Electromagnetic radiation interactions occur mostly in unstable redox environments (typically in physiological stress situations); these interactions stimulate photoacceptor molecules in the cellular membrane and in mitochondrial receptors, thereby aiding injured tissue to reach homeostasis. 3,4
LLLT has been clinically applied to reduce edema by modulating the inflammatory response; LLLT has been shown to increase phagocytosis and collagen synthesis, reduce pain, and promote tissue repair and re-epithelialization. 5 –7
Goals
The goals of this study were to investigate responses to LLLT applied in the early postoperative period in patients who had undergone bariatric surgery, with a specific focus on the short- and medium-term effects on inflammation and cicatrization.
Methods
A randomized, placebo-controlled clinical trial was conducted in 85 patients of both genders, ranging in age from 18 to 65 years. The patients were divided into two groups, that is, the placebo and laser therapy groups. All patients were admitted to the Hospital Complex of Mandaqui (São Paulo, SP, Brazil) to undergo open gastroplasty and were evaluated by anamnesis and physical examination.
LLLT was used in three sessions: immediately postoperative (IPO) and on the first and seventh PO days. The laser device was placed over the abdominal wound, with ∼1 cm spacing along the perimeter. The CW diode laser (MMOptics) was applied with the following parameters: λ = 808 nm; fluence = 10 J/cm2; power = 100 mW; intensity = 495 mW/cm2; time = 20 s per point; E = 2 J; beam diameter = 0.5 cm; and spot area = 0.20 cm2.
Patient blood samples were analyzed for levels of inflammatory markers, including C-reactive protein, creatine kinase (CK), lactate dehydrogenase (LDH), and erythrocyte sedimentation rate (ESR), during the pre- and postoperative periods. Temperature was also measured with a digital thermometer (non-contact LCD IR laser infrared thermometer; it measures temperature range from −50°C to 200°C with an accuracy of ±1°C) IPO and on the first and seventh PO days on two sites, close to and 20 cm away from the surgical wound. The patients were randomized as follows: an individual who was blinded to the patients and the proposed treatment tossed a fair coin in the air; depending on how the coin landed, 0 or 1 was corresponding to laser or placebo groups.
The visual analogue scale for pain was used to assess each patient IPO (after recovering from anesthesia) and on the first and second PO days; these assessments were conducted by the same professional who was blinded to the randomization. The surgical wounds were assessed on the first and seventh PO days for edema, erythema, and hematoma via both clinical evaluation and digital photography. Follow-up evaluations of the surgical scar for keloid formation, dehiscence, and seroma were performed before the laser was applied IPO and on the 1st, 7th, and 30th PO days.
Results
From November 2014 to October 2015, 86 patients underwent open bariatric surgery at the Bariatric Surgery Reference Center at Mandaqui's Complex Hospital. One patient was withdrawn from study due to the development of respiratory failure and coagulopathy during the postoperative period, leaving 85 patients remaining in the study.
Out of these 85 patients, 78 (91.8%) were females aged from 23 to 65 years (median, 44 ± 10). In the laser group, 39 (90.7%) were females aged from 23 to 65 years (median, 44 ± 10). In the placebo group, 39 (93%) were females aged from 25 to 63 years (median, 44 ± 10). The overall median body mass index (BMI) was 46 ± 4; the median BMI in the laser and placebo groups was 46 ± 4 and 46 ± 5, respectively.
Regarding the comorbidities in the laser group, 28 patients (65%) were hypertensive. In the placebo group, 23 (55%) were hypertensive, as shown in Table 1 with the median and standard deviation.
BMI, body mass index; HAS, hypertension.
In this study, a significant drop in temperature was observed in patients where the LLLT was applied, when compared to placebo, as shown in Fig. 1.
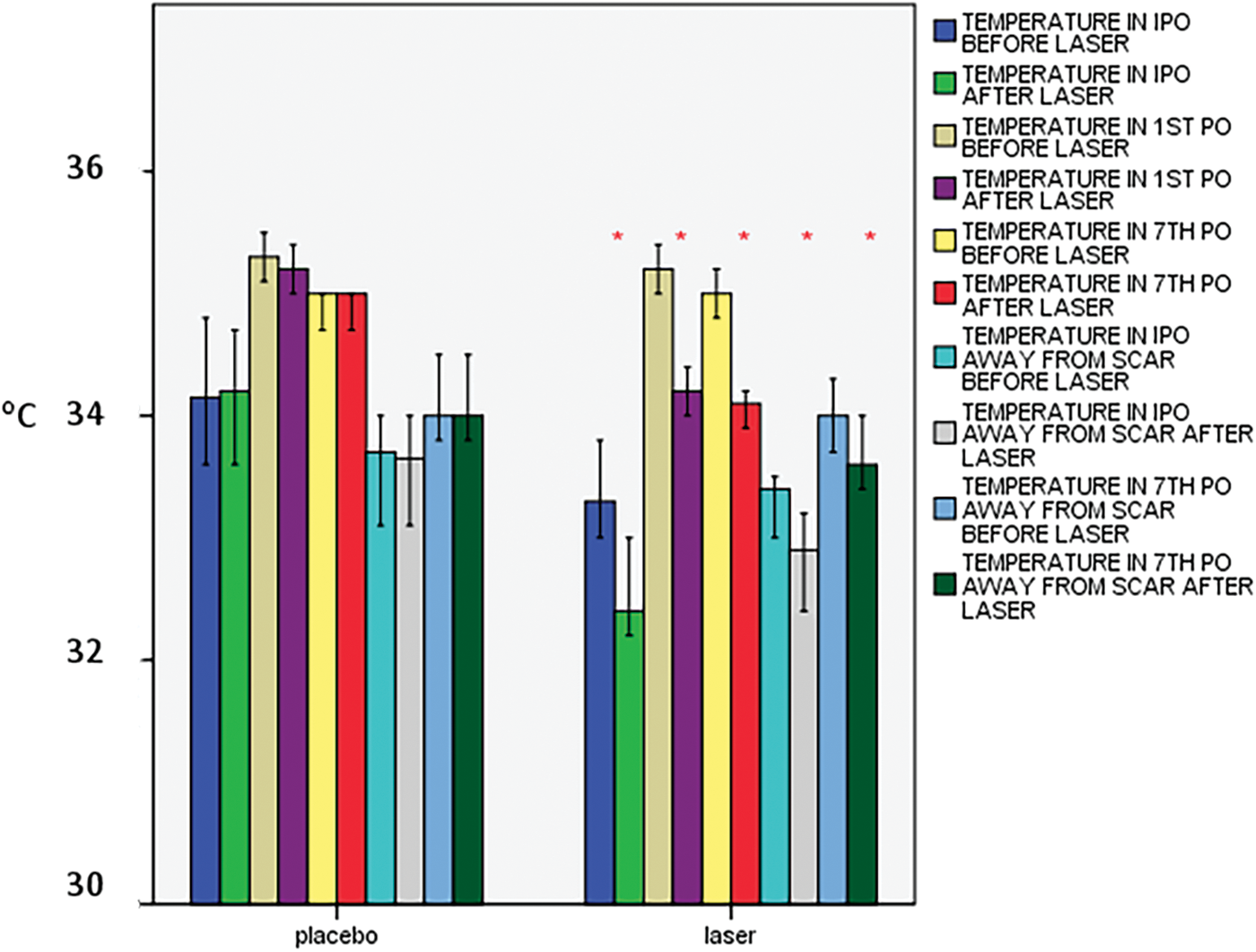
In the inferential analysis to assess the temperature, we observed a significant p (*p < 0.05) in scar in IPO, in first and seventh PO days, and away from the scar (20 cm away) in IPO and seventh PO day, showing that there was a decrease in temperature after laser therapy, and in the first away from the scar, there was a decrease in temperature with laser therapy but without statistical significance. The first bars group is represented by the placebo group and there is no statistical difference in temperature measurements either before or after inferential temperature analysis. However, when observing the second bars group, the laser group, the temperature measures drop. PO, postoperative; IPO, immediately postoperative.
It was also observed that the patients' pain in the laser group was lower compared with the placebo group, as shown in Fig. 2.
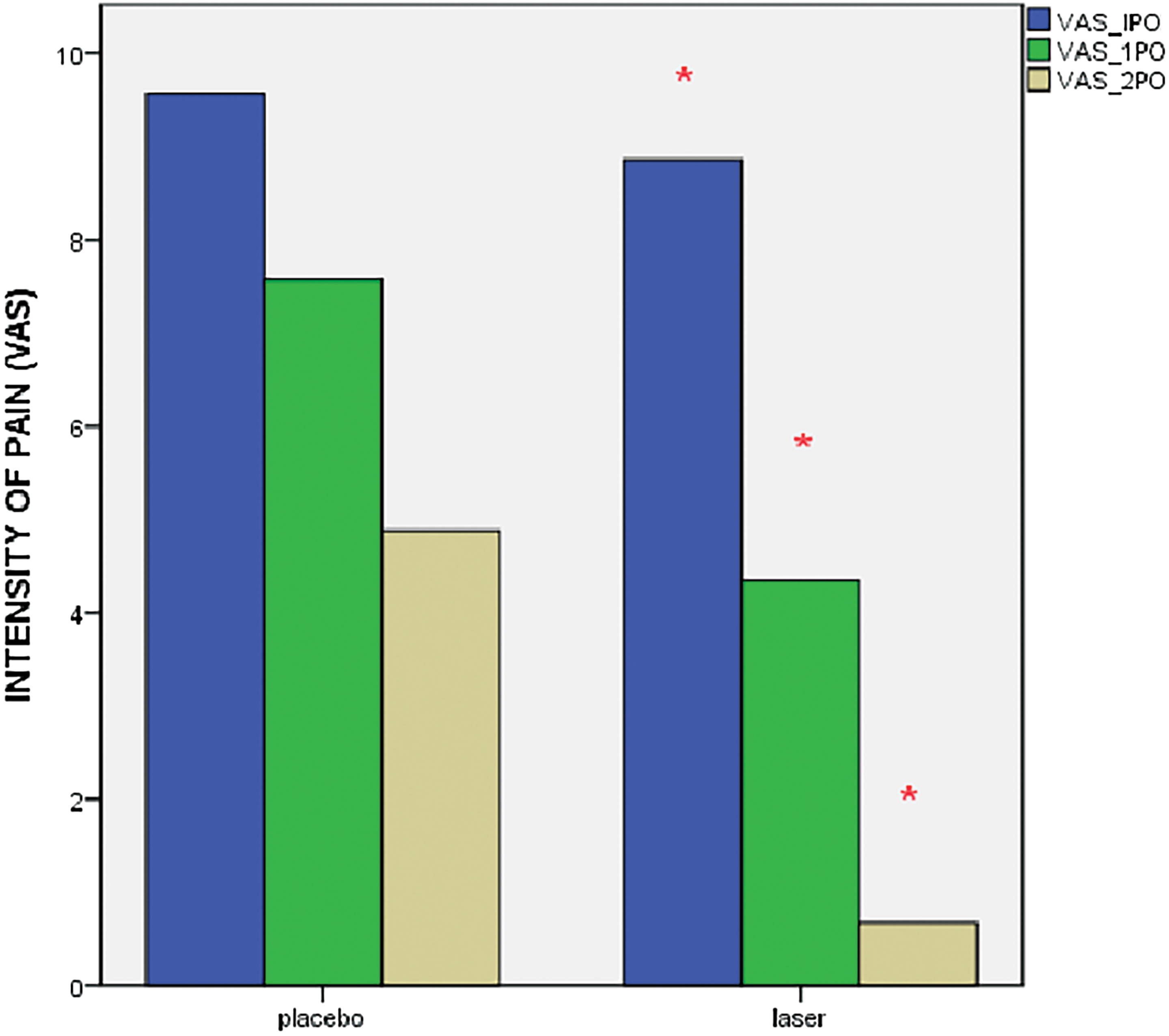
Assessing the VAS, it was observed that the p value was statistically significant (*p < 0.05). There was statistical difference in VAS of pain in patients who received laser therapy both in IPO and in first and second PO days. We observed a reduction of more pronounced pain in the three periods of laser application compared to the placebo group. The bars group first represented the placebo, observe the immediate PO period, followed by the first and second PO postoperatively. We observed a decrease in pain in both groups, which is natural in the course of postoperative time, but in the laser group, pain reduction was more pronounced, which facilitates the reduction of comorbidity such as atelectasis, thrombosis, pulmonary embolism, and infections. VAS, visual analogue scale; PO, postoperative; IPO, immediately postoperative.
The biochemical analysis showed a reduction in the ESR post-LLLT, and also a decline in complication rate in both seroma and hematoma was observed (Fig. 3).
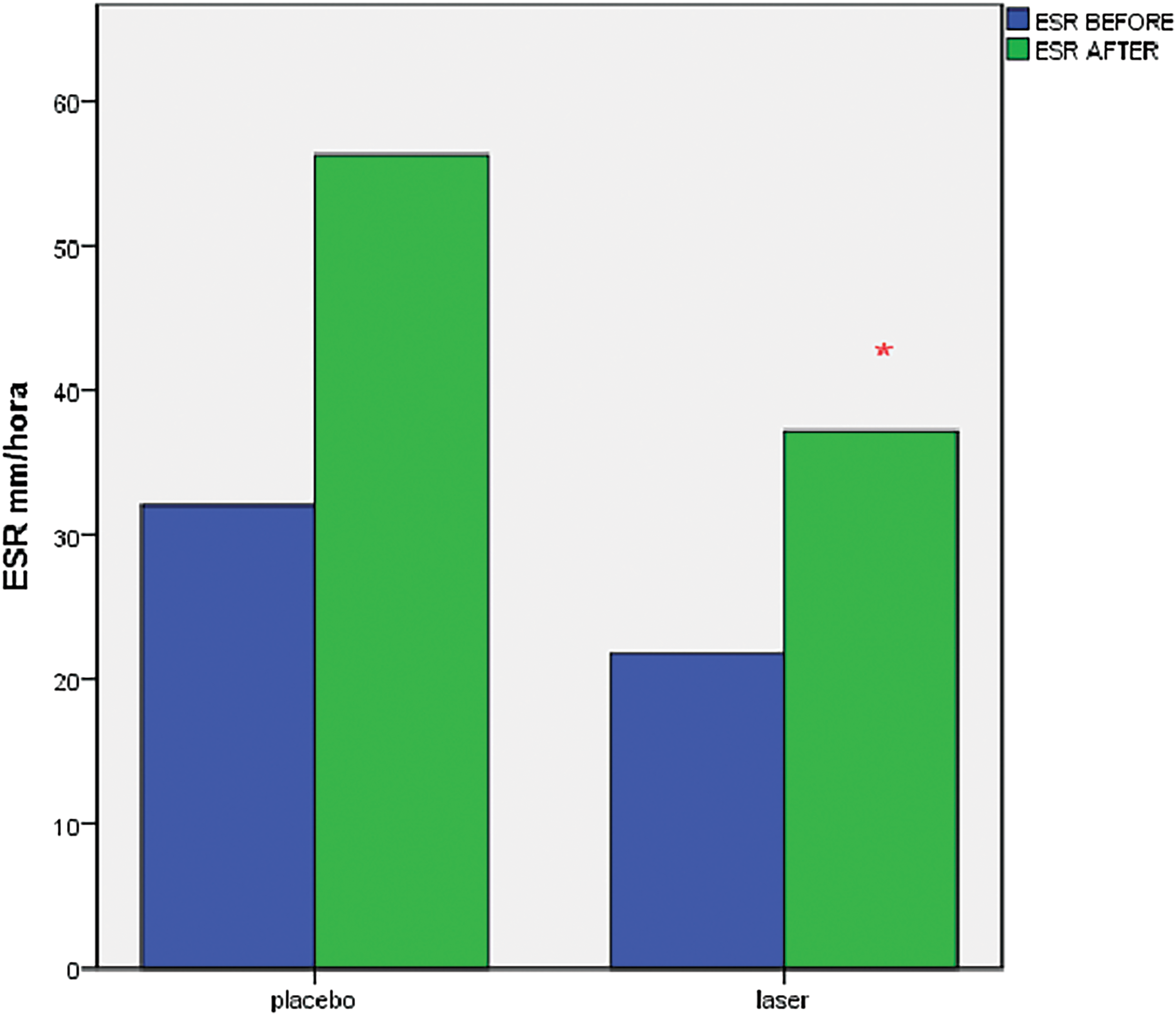
Biochemical analysis showed a decrease in ESR, decreasing seroma and hematoma. We can see the difference with statistical significance in ESR after laser therapy compared to placebo, represented by the asterisk. Showing a reduction of the inflammatory process. ESR, erythrocyte sedimentation rate.
Also, the biochemical analysis presented an increase in postoperative CK and LDH values in the laser therapy group, which may have been related to faster muscle healing in this group; however, these differences were not significant.
In relation to the clinical analysis, on the first PO day, a decrease in erythema and edema was seen and documented photographically; on the seventh PO day, a lack of erythema was observed, as well as better coaptation edges and less seroma production in patients in the laser group indicated better wound healing (Fig. 4).
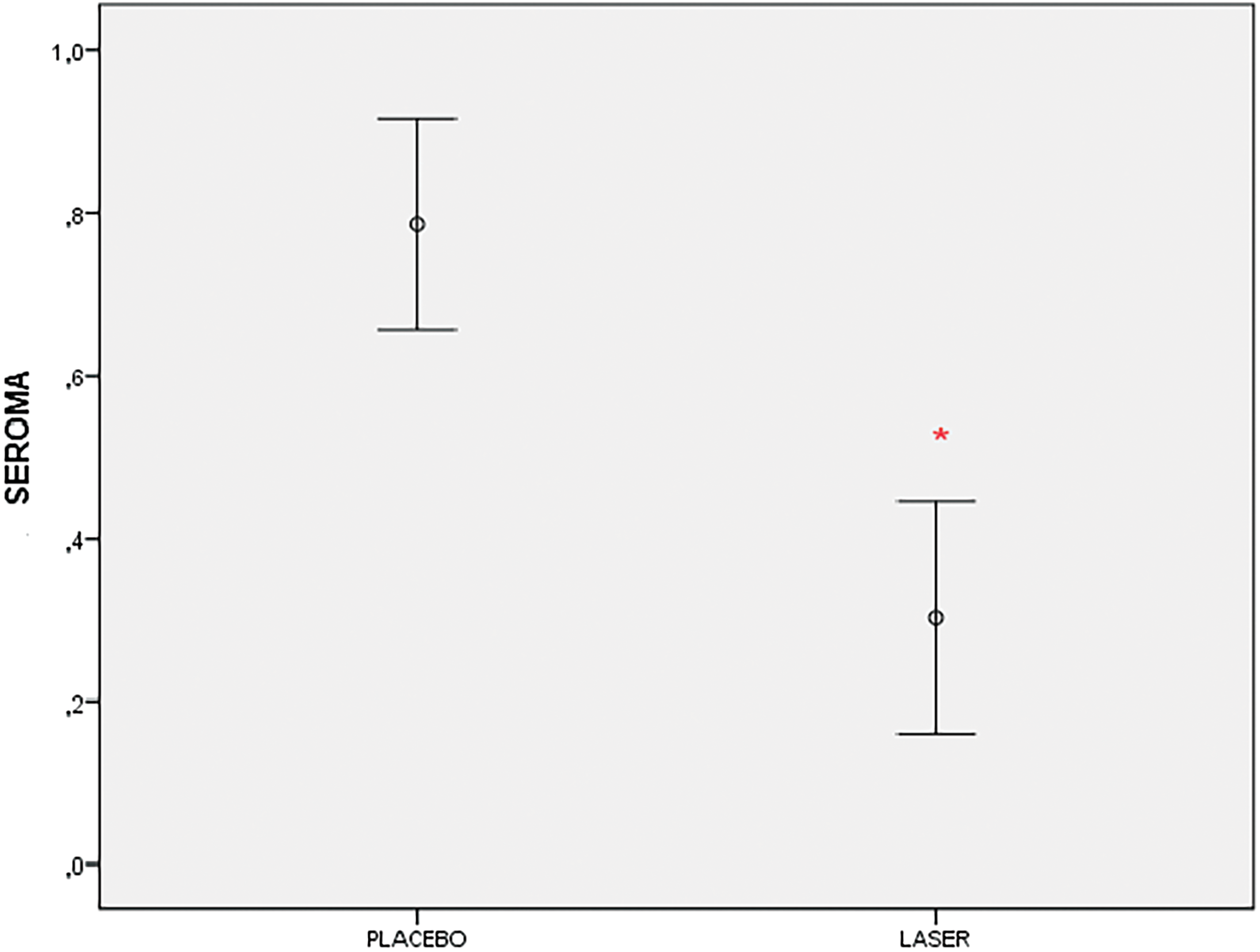
We also noticed that LLLT prevented seroma. In the laser group, seroma occurred at 30% and in the placebo group, it was 76%, showing statistical significance with *p < 0.05. Regarding infection, dehiscence, and keloid, there was no statistical significance. Shown clearly in the graph, LLLT decreased seroma, which facilitated management of the patient after surgery. LLLT, low-level laser therapy.
On the 30th PO day, the scars of patients who received LLLT exhibited better visual aspects and were thinner; the pain scores were also reduced in these patients. This analysis was performed by two plastic surgeons who were blinded to the treatment groups (Fig. 5).
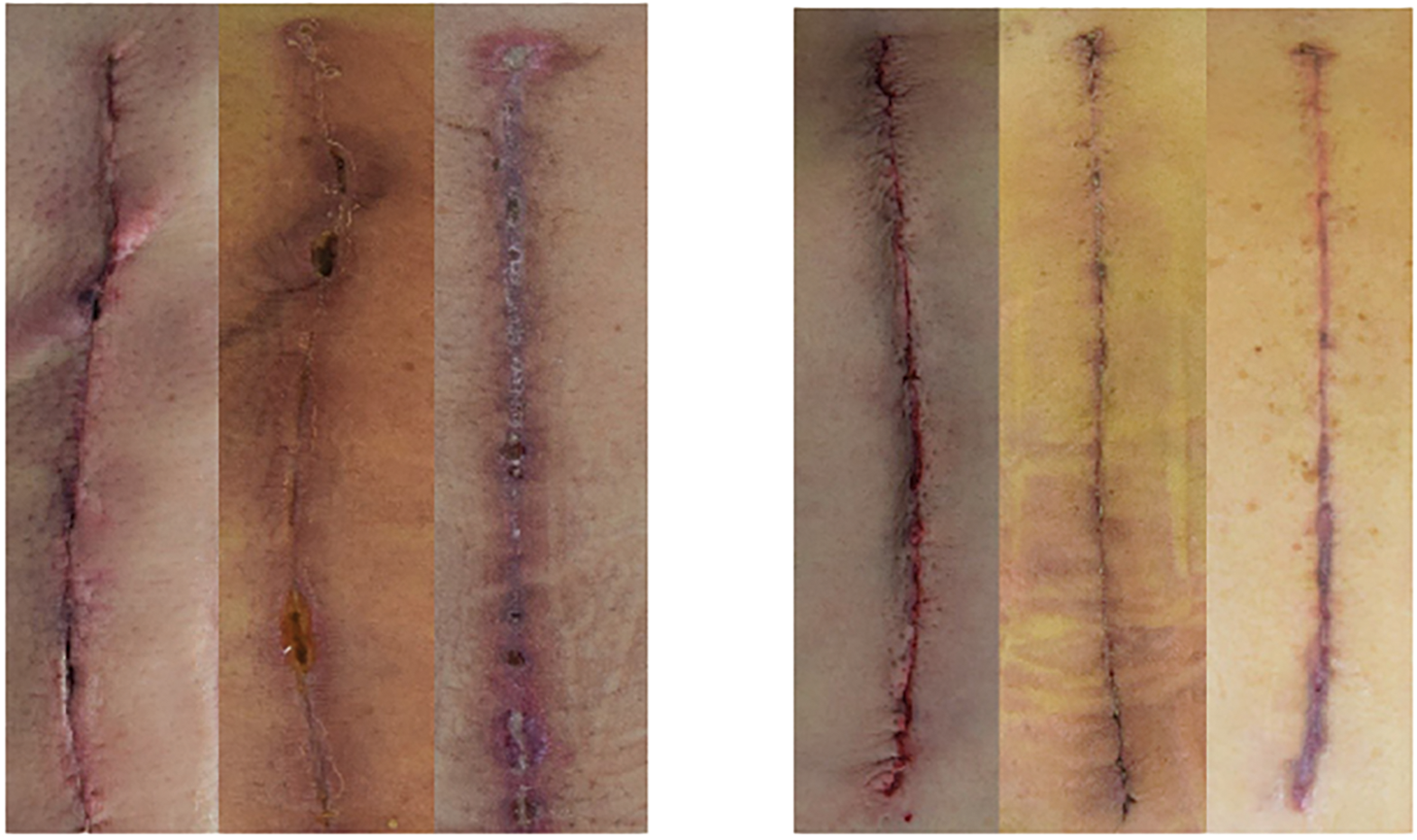
Shows the difference of healing, edema, and hyperemia in different stages of placebo group compared to the laser group, and we found the pictures of the IPO, and 7th and 30th PO days grouped in each figure. The first series of figures are the placebo group and the second series of figures are the laser group. Analyzing the figures is the clear observation of less hyperemia, less swelling, and a better coaptation of the wound edges in the laser group, with minor dehiscence and seroma. IPO, immediately postoperative; PO, postoperative.
Discussion
According to the literature, LLLT has been increasingly used due to its ability to control aspects of the inflammatory response, including edema and pain, as well as to improve the healing process; overall, LLLT is noninvasive, secure, and painless. Most studies indicate that LLLT is effective, but none has investigated the LLLT application in the digestive tract or bariatric surgery. 8 –12
Bariatric surgery is considered the most successful method for treating morbid obesity; however, in Brazil, it is still performed to a large extent using open techniques, mainly in the public health system (Sistema Unico de Saude—SUS). As with any other major surgery, this procedure inherently has the potential for complications, particularly considering the presence of obesity; such complications include pain, seroma, wound infection, and wound dehiscence, among others. 13 –15
In the tissue environment, vascular endothelial cell growth and fibroplasia occur simultaneously during the formation of granulation tissue in the first cicatrization phase, which is stimulated mainly by macrophages and platelet elements. 16
Laser therapy promotes wound healing and prevents the formation of post-surgical dehiscence, resulting in faster functional recovery. LLLT is capable of provoking biomodulation processes depending on the optical properties of the target tissue and the laser parameters used (i.e., wavelength, fluence, intensity, exposure time, and focal length). In fact, LLLT can lead to biostimulation (healing) and/or bioinhibition (pain) responses, consequently assisting the tissue recovery and analgesic processes involved. 5,17
In our study, the healing response seemed to be faster in the laser group than in the placebo group. The observed reduction in the ESR indicated that the LLLT was able to assist and reduce the local edema and inflammatory processes.
It was observed a significant drop in temperature near the wound, indicating also a reduction in local inflammation. The biochemical analysis showed the increased CK and LDH levels after the surgery, which were related to muscle injury.
The pain evaluation demonstrated a faster functional improvement in the laser group than in the placebo group. The patients who were treated with LLLT were more amenable to walking early during the IPO period, which reduced their risk for morbidities. 17
The effective reduction of seroma in patients who received LLLT suggested that faster wound healing contributed to reduced infection and dehiscence rates. Compared to the high incidence of seroma reported in the literature for conventional open techniques, the decline in seroma with LLLT was significant. 13
It is important to point that this study has some limitations. Brazil's public health system still largely uses conventional open methods for RYGB, and laparoscopic interventions are mostly reserved for patients receiving private health services. Despite these limitations, the use of LLLT as a tool for decreasing postoperative pain and seroma and promoting tissue repair is promising in major surgery. 18 An understanding of the cellular/molecular mechanisms that control the surgical wound healing induced by phototherapy will reveal new insights and potential new targets for the development of innovative therapies. Aiding healing in this way could diminish complication and pain, thereby facilitating the mobility of patients after bariatric surgery.
Conclusions
This study demonstrates that LLLT was able to act as an anti-inflammatory mediator in surgical wounds and exert an analgesic effect postbariatric surgery. The results also indicated that LLLT was able to prevent morbidity by reducing seroma, consequently improving the cicatrization process in patients after bariatric surgery and possibly in other major surgeries. Thus, laser therapy also proved its cost-effectiveness by reducing the average time of patients' stay in hospital and improving their quality of life.
Footnotes
Author Disclosure Statement
No competing financial interests exist.