
Abstract
Introduction
T
However, antibiotics, when administered systemically, may evoke unfavorable side effects, and the clinical effect of antibiotics is often limited due to the development of antimicrobial resistance. 6 So, in this context, there is a strong need for new therapeutic strategies and methods.
Antibacterial photodynamic therapy (PDT) has been used as an adjunctive, noninvasive, tissue-protecting alternative for the eradication of bacteria, most likely without triggering microbial resistance or other side effects that may occur after antibiotic therapy. 7,8 An important advantage of PDT application compared to antibiotic treatment is the fact that even antibiotic-resistant bacteria are susceptible to PDT as reported for methicillin-resistant Staphylococcus aureus. 9,10
The PDT killing mechanism involving multiple target structures in bacteria, for example, membrane lipids, proteins, enzymes, and genomic DNA, 11 may contribute to evade the development of resistance in microorganisms. 12 Apart from the antibacterial effect of PDT, it was reported that light sources such as low-energy laser or light-emitting diode (LED) may promote wound healing because of beneficial biological effects during the irradiation or so-called phototherapy. 13
The PDT requires three interactive components: a photosensitizer, a resonant light source, and oxygen. 14,15 Two mechanisms are responsible for the bactericidal effects that occur after suitable light activation in the presence of oxygen. 16 Type I reaction (electron transfer) includes the reaction of the excited photosensitizer in triplet state with the substrate producing free radicals and highly reactive oxygen species (ROS). During this photooxidative process, the photosensitizer will be reduced. In the type II reaction (energy transfer), the excited photosensitizer transfers the energy directly to molecular oxygen resulting in the highly reactive singlet oxygen causing microbial damage by biochemical interactions with cell membranes, proteins, lipids, and DNA. During this type of reaction, the photosensitizer will not be reduced.
The chemical composition of the photosensitizer and the physicochemical interactions with the environment seem to play a major role for antibacterial efficiency of PDT. Generally, the hydrophilicity, low molecular weight, and a positive charge seem to support the binding of the photosensitizer to the bacterial membrane and thus localized membrane damage. 17 However, since the susceptibility of microorganisms to PDT using pure photosensitizers varies, weak antibacterial effects may result. 18 –20 Despite many favorable effects shown by PDT application, the therapeutic benefit of this therapy is still a subject of controversial debate. 20 –22
The underlying specific mechanisms of bacterial resistance against PDT are still not understood in detail. 23 There are various reasons for the antibacterial inefficiency of conventional PDT. The environmental conditions may be suboptimal for antibacterial efficacy of PDT as periodontal application. For example, the photosensitizer may not be able to penetrate inside bacteria or stain them because of complex cell wall structures. 24 The photosensitizer may be inactivated by bleeding during the clinical procedure or in the presence of proteins produced from saliva and gingival crevicular fluid. 17 Dental biofilm-associated microorganisms may be protected against phototoxic attack by the surrounding extracellular polysaccharide matrix as physical barrier. 23
Because of the wide variety of clinical benefits of PDT, it seems worthwhile to improve the efficacy of PDT by looking for new approaches and modifications.
The aim of the present study was to improve the antimicrobial effectiveness of PDT on periopathogens by oxygen enrichment of phenothiazinium chromophores using two photodynamic systems based on the photosensitizers toluidine blue (TBO) with LED and laser light source as well as a third methylene blue (MB)-based PDT system with laser irradiation. The new modified PDT systems (PDTplus) should be investigated for possible synergistic antibacterial effects in comparison to the corresponding conventional PDT applications against six representative periodontitis/peri-implantitis-associated pathogens organized in planktonic and biofilm life forms.
Materials and Methods
Table 1 summarizes the specifications of the applied PDT systems, Table 2 gives an overview of the light exposure options of the PDT systems, and Table 3 shows the control and treatment groups.
MB, methylene blue; PDT, photodynamic therapy; S, photosensitizer; Splus, modified photosensitizer; TBO, toluidine blue.
LED, light-emitting diode.
CHX, chlorhexidine; L, light source; S, photosensitizer; Splus, modified photosensitizer.
Microorganisms and growth conditions
The following six microorganisms were used after a 24-h growth at 37°C in 3% Trypticase Soy Broth (TSB; Becton Dickinson, Heidelberg, Germany) under anaerobic conditions: Aggregatibacter actinomycetemcomitans (ATCC 43718), Actinomyces viscosus (DSMZ 43798), Fusobacterium nucleatum (ATCC 10953), Porphyromonas gingivalis (ATCC 33277), Veillonella atypica (ATCC 17744), and Streptococcus gordonii (ATCC 33399; DSMZ, Braunschweig, Germany). For anaerobic cultivation of the microbial cultures (planktonic cells, biofilm samples and inoculated agar plates), the samples were transferred into special containers (BD GasPak™ EZ; Becton Dickinson) supplied with AnaeroGen sachets (Oxoid, Wesel, Germany) reducing the oxygen concentration inside the container to below 0.1% within 2.5 h.
The TSB broth was supplemented with hemin (0.759 mmol/L; Sigma-Aldrich Chemie GmbH, Taufenkirchen, Germany), vitamin K1 (10.92 mmol/L; Sigma-Aldrich Chemie GmbH), and menadione (vitamin K3) (29.04 mmol/L; AppliChem GmbH, Darmstadt, Germany) and the pH was adjusted to 7.5. Fifty microliters of streptococci cells were inoculated in 5 mL Schaedler broth (BBL Schaedler broth; Becton Dickinson) and incubated anaerobically for 17 h at 37°C. Of the five anaerobes, 50 μL of each was inoculated in 9 mL sterile supplemented TSB medium and incubated anaerobically for 24 h at 37°C.
Anaerobic multi-species planktonic model
After the 24-h growth, the single-strain bacteria were pooled, harvested by centrifugation (6000 g, 2 min), suspended in fresh, supplemented TSB medium, and homogenized by vortex mixing. The resulting anaerobic multi-species cocktail was used for planktonic treatments (500 μL). Initial microbial cultures used for antiseptic exposure or biofilm formation were prepared with a bacterial density of 9.15 log10 CFU (colony forming units) equivalent, to standardize microbiological starting conditions.
Anaerobic multi-species biofilm model
The biofilm formation of periodontitis-associated pathogens was performed by exposing the multi-species cocktail to human tooth slides for 24 h anaerobically at 37°C. The environmental medium for biofilm formation was prepared from 50% sterile human plasma and 50% human saliva. The plasma was collected from human heparinized blood (heparin: 9 I.E./mL solution) and sterile filtered with a 0.45-μm-pore-diameter filter. Paraffin-stimulated whole saliva was homogenized and separated by centrifugation into the bacterial pellet and the cell-free supernatant (12,000 g for 30 min at +3°C, Multifuge X1R; Heraeus, Hanau, Germany) as described earlier. 25 After sterile filtration of the supernatant, the pH of the sterile saliva was adjusted to 7.2. The plasma/saliva suspension was supplemented with hemin, vitamin K1, and menadione like the TSB medium. The pH was adjusted to 7.4.
Control groups
Different control groups for the planktonic and biofilm-associated pathogens were established (Table 3): (1) sodium chloride (NaCl, 0.9%) as negative control (S−L−), (2) 0.2% chlorhexidine (CHX, Chlorhexamed® Forte; GlaxoSmithKline Consumer Healthcare GmbH & Co. KG, Bühl, Germany) as antibacterial-positive control (S−L−), (3) hydrogen peroxide (3%, H2O2) as control for modified PDTplus (S−L−), (4) light exposure only (S−L+), (5) pure photosensitizer only (S+L−), and (6) photosensitizer+H2O2 (3%) without light exposure (Splus+L−). Group 5 served as control for each PDT system (dark toxicity). The chemical controls NaCl, CHX, and H2O2 were applied for 30 sec. The exposure time of bacterial samples to light or photosensitizer as PDT controls was 60 sec.
PDT systems
Three conventional PDT systems were applied (Table 1). The first one was a TBO-based PDT system (PDT1, Photosensitizer S1, light source L1) using LED excitation at 630 nm (FotoSan 630; CMS Dental, Copenhagen, Denmark), the second a TBO-based PDT system with low-energy laser excitation at 635 nm (PDT2, Photosensitizer S2, light source L2) (PACT; CumDente, Tübingen, Germany), and the third an MB-based PDT system (PDT3, Photosensitizer S3, light source L3), including a low-energy laser excitation at 665 nm (HELBO®; Bredent Medical, Waldorf, Deutschland).
The three PDT systems were applied in two different experimental options. The first option was the conventional use of PDT in the default mode according to the manufacturer's instructions (S+L+). The second option implied the three conventional PDT systems being modified by supplementing the specific photosensitizer with 3% hydrogen peroxide (PDTplus, Splus+L+) (Table 2). The experimental irradiation procedures for the three modified systems (PDT1plus, PDT2plus, PDT3plus) were the same as for the conventional PDT systems (Table 3).
Photodynamic treatment of periodontal planktonic bacteria
The multi-species cocktail (500 μL) was centrifuged and the pellet was exposed to 200 μL photosensitizer for 60 sec. The subsequent irradiation with LED/laser was carried out using a perio tip with an immersion depth of 7.5 mm for 60 sec (PDT1, PDT2, PDT1plus, and PDT2plus). According to the manufacturer's instructions for clinical use, following bacterial exposure for 60 sec, the photosensitizer MB was removed by short centrifugation and the sample was resuspended in 1 mL saline. PDT3 and PDT3plus were performed by laser irradiation using a perio tip under conditions similar to PDT1, PDT1plus, PDT2, and PDT2plus. After all PDT administrations, bacteria were suspended in 500 μL fresh supplemented TSB medium for microbiological analysis.
Photodynamic treatment of periodontal biofilm-associated bacteria
After 24 h of biofilm growth, the biofilms were treated in situ. They were shortly rinsed with 1 mL distilled water to remove loosely bound bacteria. Concerning TBO controls and TBO-based PDT systems (PDT1, PDT2), the biofilms were exposed to the photosensitizer for 60 sec. During PDT (PDT1, PDT2, PDT1plus, and PDT2plus), the irradiation of biofilm samples with red LED or laser light was performed using a spherical tip for 60 sec with a distance of 9.5 mm between light source and biofilm surface. MB-associated PDT (PDT3 and PDT3plus) included an additional rinsing step after photosensitizer application according to the manufacturer's instructions.
After 60 sec of MB sensitizing, the samples were gently washed in distilled water to remove excess photosensitizer. Subsequently, the biofilms were transferred into saline and irradiated with laser by use of a spherical tip for 60 sec under similar conditions than the other photodynamic treatments. After these treatments, the biofilms were removed from the substratum by mechanical scraping and the bacterial deposit was suspended in 250 μL sterile supplemented TSB medium. Following homogenization, the samples were analyzed for their microbial viability. The CFU counts of the periodontal biofilms were correlated to the tooth surface area in CFU/mm2.
Microbial viability
To evaluate the antibacterial efficiency of the different treatment groups, the viability of microorganisms was characterized by determination of the total cell counts (BC), the growth parameter CFU of planktonic and biofilm bacteria, and the bacterial vitality proportions (% Vit, live/[live and dead] ratio) as described previously. 26,27 The determination of BC was performed by means of dark field microscopy. CFU growth was determined by using the agar spiral plating technique for the samples on Schaedler agar (Becton Dickinson GmbH) and colony counting after growth for 5 days at 37°C under anaerobic conditions. The bacterial vitality determination was carried out after fluorescent staining with the LIVE/DEAD BacLight Bacterial Viability Kit (Invitrogen, Darmstadt, Germany) by fluorescence microscopy (Axioplan 2; Carl Zeiss Microscopy GmbH, Jena, Germany).
Statistics
Ten different test series were performed for each condition. BC and CFU data were transformed using base-10 logarithms. Statistical analysis of data was performed using 95% confidence intervals (ANOVA) and the post hoc Tukey's test. The significance level (alpha) was set at 0.05 (p < 0.05).
Results
The mean of the total bacterial cell counts (BC/mL) of the starter cocktail for all experimental conditions was 9.45 log10 units of BC/mL.
Planktonic treatment: controls
The bacterial treatment of planktonic cells with the negative control NaCl (9.033 log10 CFU/mL) served as reference for comparison of the antibacterial efficacies achieved by the different treatments (Fig. 1A). The antibacterial standard CHX showed a CFU reduction of pathogenic bacteria of 8.732 log10 units. Hydrogen peroxide reduced the CFU of the planktonic periodontopathogens by 1.256 log10 units (Fig. 1A). The vitality results of the control treatments corresponded to the results of log CFU values (Fig. 1B). The positive control CHX caused 69.3% reduction and H2O2 a 19.0% decrease of vitality in comparison to NaCl exposure.
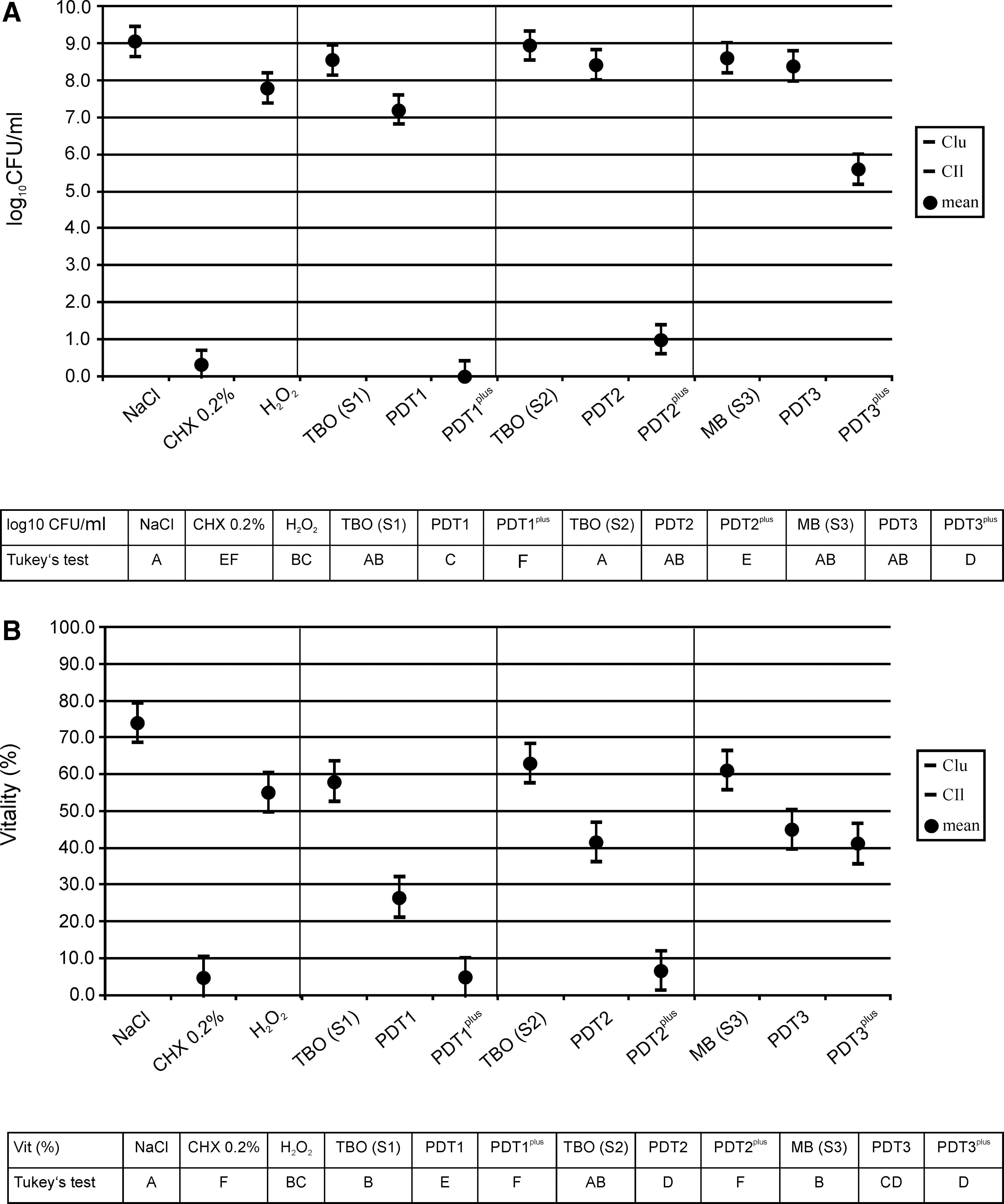
The light exposure group, including LED and lasers applied to planktonic bacteria, revealed the following mean log10 CFU values: 8.878 for LED (PDT1), 8.921 for laser (PDT2), and 8.894 for laser (PDT3). The mean values of the vitality were 66.0% (LED of PDT1), 60.0% (laser of PDT2), and 70.0% (laser of PDT3).
The exposure only to photosensitizers resulted for all applied PDT systems in a similar low antibacterial effect of 0.1–0.5 log10 CFU reduction (Fig. 1A).
The control group (photosensitizer+H2O2) without light exposure showed the following mean log10 CFU values: 5.199 (S1plus), 7.689 (S2plus), and 7.238 (S3plus). The corresponding mean vitality values were 66.7% (S1plus), 66.7% (S2plus), and 70.0% (S3plus).
Planktonic treatment: PDT/PDTplus
Concerning the conventional PDT, only the PDT1 system showed a statistically significant growth reduction (1.84 log10 CFU) in contrast to PDT2 and PDT3. With regard to the modified PDT, including oxygen-enriched photosensitizers, all tested PDTplus systems were significantly more effective in reducing bacterial growth compared to negative control and conventional PDT treatment (Fig. 1A). The TBOplus-LED system (PDT1plus) showed a maximum 9.033 log10 CFU reduction, the TBOplus-laser system (PDT2plus) caused a CFU decrease of 8.051, and the MBplus-laser system (PDT3plus) achieved a reduction of 3.444 log10 CFU compared to the data of the negative control (Fig. 1A).
When comparing the default with the modified PDT, the modified PDT1plus and PDT2plus application resulted in a higher log10 CFU/mL reduction of 7.195 and 7.421 referring to PDT1 and PDT2. PDT3plus administration to pathogens caused a 2.786 log10 CFU reduction, which was stronger than with PDT3 (Fig. 1A).
Concerning bacterial vitality, treatment with photosensitizers, S1 and S3, decreased the vital cell proportions statistically and significantly compared to the negative control (vitality reduction S1: 16.0%, S3: 13.0%) (Fig. 1B). All three default PDT applications induced statistically significant vitality reductions compared to saline [47.5% (PDT1), 32.5% (PDT2), and 29.0% (PDT3)].
However, the exposure of the modified PDTplus systems showed the strongest statistically significant vitality decrease for PDT1plus (69.5% reduction) and PDT2plus (67.5% reduction). PDT3plus achieved 33.0% vitality reduction in comparison to saline and this efficacy on pathogens was similar to that of the conventional systems PDT3 and PDT2. The modified PDT showed for PDT1plus a 22.0% and for PDT2plus a 35.0% increase in vitality reduction compared to the default PDT. The vitality difference between PDT3 and PDT3plus was minimal (4.0%).
Biofilm treatment: controls
The log10 CFU/mm2 value after NaCl exposure (5.801 log10 CFU/mm2) was used as reference for assessing the antibacterial effects of the other treatments on biofilm bacteria. CHX affected bacterial growth statistically and significantly by CFU/mm2 reduction of 2.739 log10 units compared to saline (Fig. 2A). The exposure of H2O2 to biofilm bacteria showed a statistically significant antibacterial effect of 1.525 log10 CFU/mm2 reduction. A similar pattern was detected for vitality and colony growth. The vitality reduction of CHX was 50.5% and of H2O2 was 17.5% (Fig. 2B).
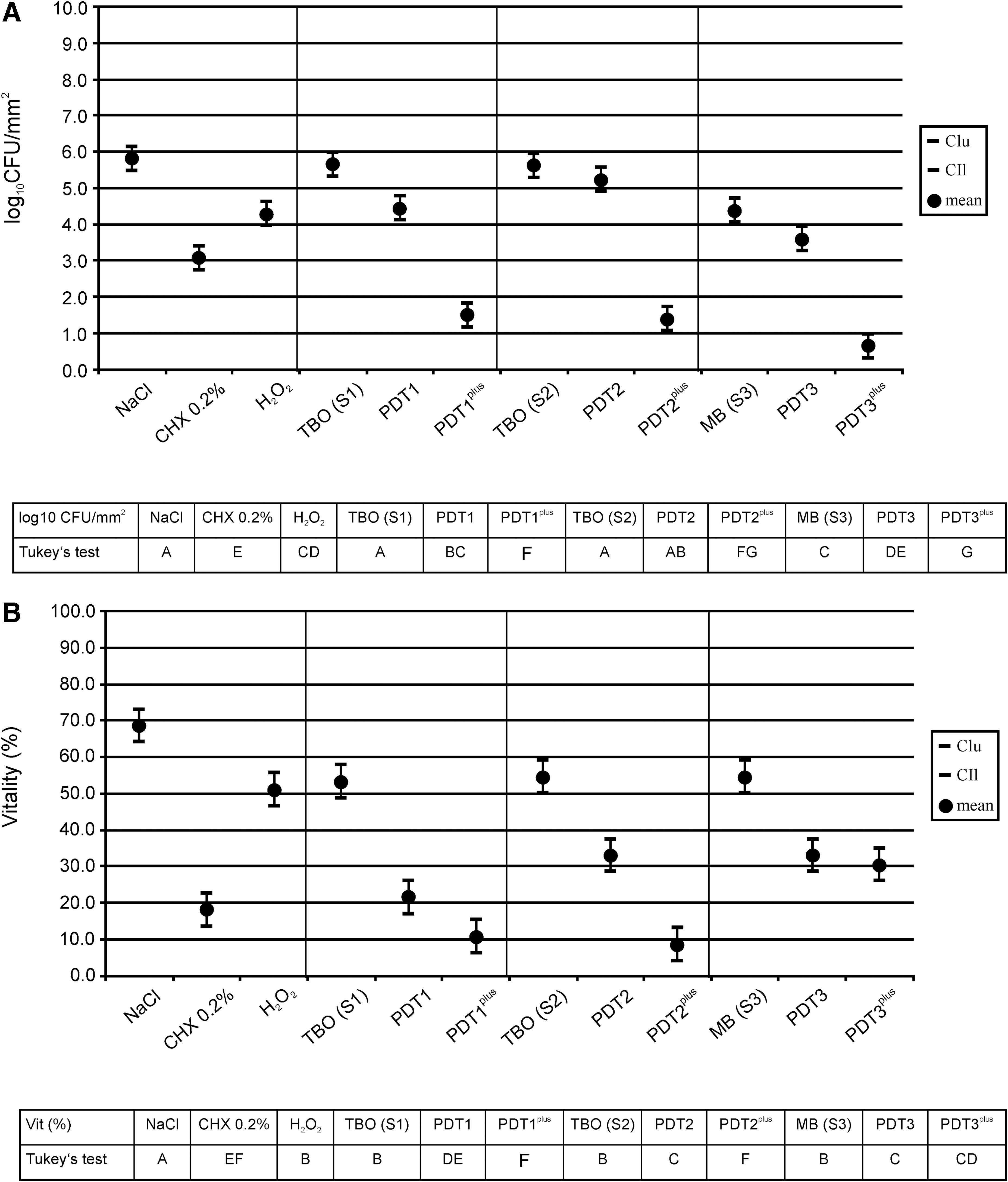
The periodontal biofilms exposed to light only, including LED and lasers, achieved the following mean log10 CFU/mm2 values: 5.311 for LED (PDT1), 5.138 for laser (PDT2), and 5.347 for laser (PDT3). The mean vitality values after light exposure of the biofilms were 61.7% for LED (PDT1), 53.3% for laser (PDT2), and 60.0% for laser (PDT3).
Concerning the application of photosensitizers only, TBO hardly showed antibacterial effect on biofilm samples just like on planktonic bacteria (Fig. 2A). However, MB without irradiation reduced the biofilm-based colony growth statistically and significantly by 1.418 log10 CFU/mm2. Concerning the microbial vitality proportions, similar results were obtained for S1, S2, and S3 although statistically and significantly lower than the mean vitality values after saline exposure (Fig. 2B).
The log10 CFU values of the treatment combination (photosensitizer+H2O2) at darkness were 4.663 (S1plus), 5.080 (S2plus), and 6.259 (S3plus). Biofilm exposure to the supplemented photosensitizers without light showed the mean vitality values: 40.0% (S1plus), 45.0% (S2plus), and 61.7% (S3plus).
Biofilm treatment: PDT/PDTplus
Within the PDT treatment group, PDT1 caused a CFU/mm2 decrease of 1.370, PDT2 of 0.581, and PDT3 of 2.219 log10 units, the latter in a statistically significant way in comparison to the negative control (Fig. 2A). The modification of PDT reinforced the antibacterial effect on biofilm bacteria statistically and significantly compared to the negative control and PDT in the default mode. The mean CFU/mm2 reduction initiated by PDT1plus was 4.312, by PDT2plus was 4.415, and by PDT3plus was 5.159 log10 units referring to saline. Comparing default and modified PDT, the statistically significant superior CFU/mm2 reduction of PDT1plus was 2.942, of PDT2plus was 3.834 and of PDT3plus was 2.940 log10 units.
For all PDT systems the biofilm treatment by conventional application resulted in statistically significant vitality reduction compared to the pure photosensitizers and negative control, similar to the planktonic treatment (Fig. 2B). The mean vitality reduction after PDT1 exposure to biofilms was 47.0% and after both PDT2 and PDT3 application was 35.5%. Bacterial vitality of periodontal biofilms was further significantly decreased by 57.8% (PDT1plus) and 60.0% (PDT2plus) after exposure to the modified PDTplus procedure. PDT3plus caused a biofilm vitality reduction by 38.0% lying within a similar range as the vitality after default PDT administration. Comparing the effect of the modified PDTplus values with those of the conventional PDT, the vitality was reduced by 10.8% (PDT1plus), 24.5% (PDT2plus), and 2.5% (PDT3plus).
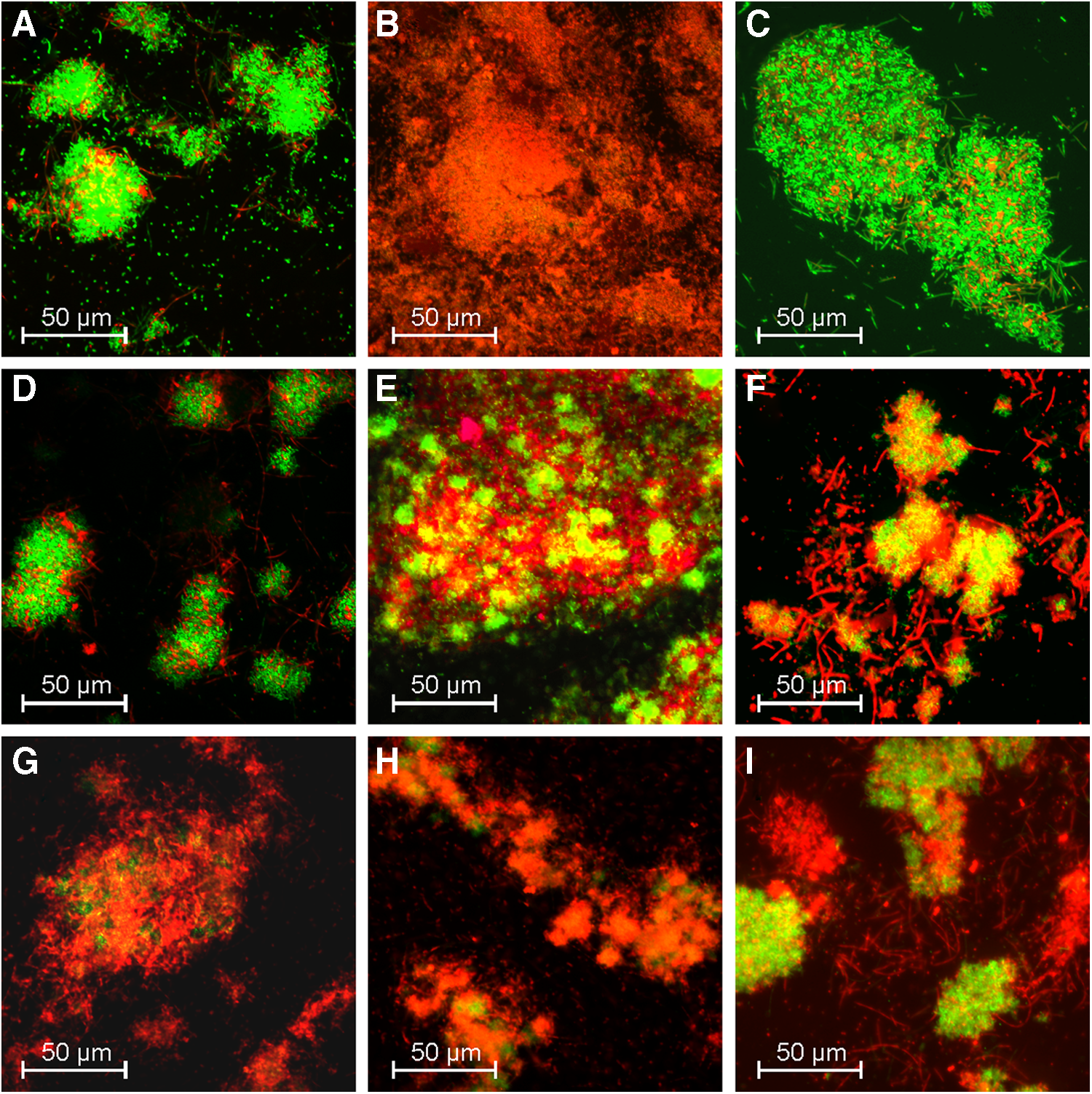
Figure 3A–I includes fluorescence images of detached periodontal biofilms after different exposure procedures.
Discussion
As shown in the present study, three commercially available PDT systems applied to planktonic and biofilm-associated periodontopathogens showed different antiseptic effects. The CFU reductions concerning planktonic and biofilm bacteria ranged from below 1 log10 unit to maximal 2.22 log10 units. Hence, the PDT-mediated antibacterial effect was only moderate and insufficient for complete microbial eradication. These findings are in concert with a study by Dörtbudak et al. 28 The results of this clinical study investigating the antibacterial effect of a TBO-based PDT with laser irradiation on bacterial contaminated implant surfaces of peri-implantitis patients involving A. actinomycetemcomitans, P. gingivalis, and Prevotella intermedia revealed a CFU reduction of 2 log10 units but no complete elimination.
Similarly, another study concerning periodontal pathogens treated with a conventional TBO-based PDT procedure reported a log10 CFU reduction of 2. 29 The study of Pagonis et al. focused on the antibacterial effect of a nanoparticle-based PDT on planktonic Enterococcus faecalis cells. 30 In this context, the combination of red laser light and MB-loaded nanoparticle led to a CFU reduction of 1.5 log10 units. These reports and other studies confirm the partially weak PDT effects on different pathogens underlining the need for developing new strategies to improve the antimicrobial outcome of PDT. 31
With regard to oxygen as an essential requirement for the phototoxic mechanism, the subgingival and also the endodontic environmental milieu have considerable influence to what extent PDT was successful. These bacterial sites of infections are characterized by “hypooxygenic” nature and therefore fail to provide enough molecular oxygen for effective generation of singlet oxygen. 32 Especially, the infection-associated biofilms become depleted in oxygen during their maturation because of oxygen consumption by facultative anerobes, concentration gradients within the biofilms, and presence of an extracellular polysaccharide matrix. 33
The results of the simultaneously administered photosensitizer with H2O2 confirmed a statistically significant higher potential for bacterial photodestruction than the default PDT. Concerning the planktonic cell part, the modified combination therapy resulted in a complete eradication after PDT1plus use (log10 CFU/mL reduction of 9.033), better even than CHX, the gold standard for antibacterial mouthrinses (log10 CFU reduction of 8.732). Eradication was almost complete after PDT2plus application (log10 CFU reduction of 8.051) in comparison to the moderate effect of the corresponding default PDT. From the TBO-based systems, both oxygen-enhanced procedures PDT1plus and PDT2plus achieved also stronger antibacterial efficacies against biofilms (log10 CFU/mm2 reduction of 4.312 by PDT1plus, 4.415 by PDT2plus) referring to the negative control in comparison to the weak antiseptic effect of conventional PDT (log10 CFU/mm2 reduction of 1.370 by PDT1, 0.581 by PDT2). These data include additional log10 CFU/mm2 reductions of 2.942 (PDT1plus) and 3.834 (PDT2plus) on periodontal biofilms caused by the modified photodynamic approaches compared to the corresponding default PDT. The vitality proportions corresponded mainly to the growth inhibition profile after PDT of all systems. The positive control CHX caused a much stronger antibacterial effect than conventional PDT but a weaker effect than the modified PDTplus procedure.
The application of MB-based PDT influenced the bacterial growth of planktonic and biofilm periodontopathogens differently from the TBO-based PDT. Whereas the antibacterial effect of PDT3 on planktonic bacteria showed only a slight growth inhibition effect (log10 CFU/mL reduction 0.658) and higher vitality rates (45%), the PDT3 effect on periodontal biofilms was significantly higher than that of the TBO-based systems and negative control. For planktonic pathogens, the modified MB-based PDT3plus system reduced bacterial growth more effectively than the default PDT3 but significantly weaker than TBO-based modified PDTplus systems.
Concerning the periodontal biofilms, the oxygen-enhanced PDT3plus administration led to the highest antimicrobial effect (log10 CFU/mm2 reduction 5.159), although the vitality proportion (30%) exceeded the values obtained by PDT1plus and PDT2plus. However, a high percentage of vital pathogens do not always mean living reproducible bacteria but may also indicate nondefined transitional life states where cells are still alive but no longer able to grow. 26 Compared to default PDT3, the PDT3plus application on biofilms enhanced the antibacterial effect by 2.940 log10 CFU/mm2.
The phototoxic efficacy of TBO and MB applied in conventional PDT showed inconsistent results in the literature. 34 Both thiazine dyes promoted photodestruction of microorganisms under light irradiation but their photophysical properties and photodynamic activities differed against varying bacteria and under light or dark conditions. 34 Both agents caused molecular damage of lipids and proteins after binding to the outside membranes, but TBO appears to be more effective than MB. 34 Many influencing factors are involved in the complex phototoxic mechanisms, for example, the different cellular localizations of TBO and MB. Further, different planarities and varying abilities to dimerize in solutions may contribute to the different phototoxic effects.
From all these findings it can be concluded that the photosensitizer oxygenation of all three PDT systems achieved a synergistic effect regarding the phototoxicity of PDTplus, which was much stronger than the antibacterial efficacy after single-drug exposure of H2O2 and of conventional PDT and their additive effects.
Differentiating the photosensitizers toluidine and MB, it could be stated that this oxygen-based synergism is particularly strong for TBO, because only the TBO-related photodynamic treatments PDT1plus and PDT2plus maximally reduced the colony growth of both planktonic and biofilm-associated bacterial life forms. The observed minor differences in efficiency between PDT1plus and PDT2plus led to the substantial conclusion that the synergistic effect obtained by TBO with H2O2 seems to be independent from the irradiation light source LED (PDT1plus) or laser (PDT2plus). The small differences in efficacy between PDT1plus and PDT2plus may be related to the different TBO concentrations in the systems.
A synergistic antibacterial effect of oxygen-supplemented photosensitizer without light exposure could be observed for S1plus (higher dose toluidine with H2O2) applied on planktonic and biofilm periodontal pathogens. This could be due to the specific activation mechanism of toluidine in the presence of hydrogen peroxide because TBO without additive is described to be a more effective bactericide at darkness than MB. 34
With regard to MB, a synergistic antibacterial effect of the modified photosensitizer exceeding the sum of individual effects of pure H2O2 and default PDT could also be detected for planktonic bacteria but to a lesser extent compared to TBO. However, after treatment of biofilm-associated bacteria, the antibacterial effect was stronger than that of TBO-based systems. These findings are surprising because mostly antiseptic procedures are more effective against non-sessile cells than against bacterial biofilms which represent a barrier to eradication strategies. 32
The high antibacterial efficacy of MB on biofilm periodontopathogens in the present study may result from the 100 times higher photosensitizer concentration compared to TBO, which may support more effective diffusion across the biofilm layers to sensitize bacteria before irradiation. This concentration-dependent effect may account for the findings that MB showed the highest dark toxicity among the photosensitizers, the highest growth inhibition among default PDT treatments and among oxygen-enhanced PDTplus procedures but only concerning periodontal biofilm-associated target bacteria, not the free living planktonic counterparts.
The relationship between photosensitizer concentration and antibacterial PDT efficacy could be shown for several microorganisms. 35
The system- and light source-independent synergistic antibacterial effect of oxygen-enriched thiazine dyes showed the maximum antibacterial impact only during a simultaneous application of both components photosensitizer and H2O2, as shown in the present study. In the study of Eick et al., H2O2 exposure of a periodontal biofilm separately before administration of TBO-based PDT enhanced the phototoxic effect from a CFU reduction of 1.41 log10 units after conventional PDT to 1.88 log10 units after pretreatment with pure H2O2 followed by PDT. 29 From these findings it is evident that the subsequent application of the two components showed an increasing antibacterial effect, but it was far less effective than the simultaneous application.
As demonstrated in a recent study dealing with MB-based PDT, spectroscopy experiments showed that the quantity of photosensitizer inside cells of Escherichia coli was higher in the presence of H2O2, which was applied before PDT or during PDT. 36 Based on the results of the present study and additional to other study findings, it can be assumed that oxygen enrichment of especially TBO and also MB in combination with light irradiation boosts the oxygen-dependent phototoxic reactions and the generation of highly ROS compared to unsupplemented thiazine dye-associated PDT.
Several other PDT modifications have been established by photosensitizer conjugation to different agents or actions to increase the phototoxic efficiency of PDT at different levels. Barra et al. applied PDT followed by antibiotic exposure (gentamicin) successfully against biofilms consisting of several gram-positive bacteria. 37 The antibacterial efficacy of MB-based PDT against a very resistant endodontic pathogen, E. faecalis, could be increased by a combination therapy of first photodynamic treatment with subsequent exposure to sodium hypochlorite (NaOCl 2.5%). 38
Tennert et al. developed an antibacterial strategy against the same endodontic pathogen combining different irrigation solutions (EDTA, NaOCl, citric acid) with subsequent TBO- and LED-based PDT. 39 However, in this study, the antimicrobial efficacy attained by the combinations was at the same level as sole NaOCl irrigation (99.9%). A further disinfection approach was performed using a combination of PDT with antiseptic mouthrinses. 38,40 Friedberg et al. specifically targeted Pseudomonas aeruginosa and achieved elimination by binding a photosensitizer with a monoclonal antibody and additional light activation. 41
George and Kishen modified the photosensitizer formulation of MB by including an oxygen carrier in various combinations with an oxidizer and a solubilizing detergent. 32 The antibacterial efficacy of the combined components against E. faecalis biofilms grown in vitro or after ex vivo collection was superior to conventional PDT. This could be due to higher oxygen concentration and facilitated penetration of MB into the biofilm contrasting to the conventional PDT involving MB dissolved in water. However, toxicological aspects concerning unknown interactions between the active ingredients in this mixture and endodontic tissues are given little or no consideration.
Encapsulated nanoparticles loaded with the photosensitizer were also prepared to enhance the phototoxic elimination of bacteria. 30 Another antibacterial improvement strategy of PDT was developed by Verma et al. in a targeted approach, where on the one hand, TBO was modified molecularly by side chain functionalization to new derivatives. 42 On the other hand, TBO was used as inactive photodrug conjugated to a cephalosporin scaffold and in the presence of bacterial β-lactamase activity, contrary to conventional antibiotics, the lactam ring opening released the photosensitizer and light activated the drug for photodestruction. 42
The advantage of the modified PDTplus introduced in the present study is that the external supply of H2O2 corresponds to the similarly reduced reactive metabolite H2O2, which is supposed to be intrinsically converted from the ROS superoxide anion (•O2) during phototoxic-induced cell damage by the enzyme superoxide dismutase. 43,44 Therefore, it can be assumed that the photochemical mechanisms in the PDT and PDTplus may be similar because no other external chemical compounds are involved. Nonetheless, the efficacy of the modified PDTplus has been shown to be far superior, due to the higher amount and availability of reactive oxygen molecules on-site by conversion of hydrogen peroxide contributing to the PDT efficacy. 44
As hydrogen peroxide is a widely used agent also for oral debridement, 36 the PDTplus procedure is suggested to be toxicologically safe and, further, easy to use.
Conclusions
Within the experimental limitations of the present study, the results revealed that the photosensitizer enrichment with hydrogen peroxide during PDTplus promotes antimicrobial photodynamic activities to a statistically significant high degree against periodontal pathogens in planktonic and biofilm life forms first of all for TBO, and also for MB, although less effectively. This is in contrast to using the photosensitizers TBO or MB as the sole agents in the conventional PDT. For TBO, the increased antiseptic effect by synergistic mechanisms seemed to be independent from the therapy system and type of light source, because the results could be shown by using two different concentrations in two different commercial PDT systems regardless of LED or laser irradiation.
The PDTplus procedure may become an adjunctive, highly effective antibacterial approach for the treatment of periodontitis and peri-implantitis without the danger of drug-resistant bacteria or undesirable side effects. Further studies are needed concerning the antibacterial efficiency against other oral pathogens and for future clinical application.
Footnotes
Author Disclosure Statement
No competing financial interests exist.